

Abstract
The recent influenza pandemic, caused by a novel H1N1 influenza A virus, as well as the seasonal influenza outbreaks caused by varieties of influenza A and B viruses, are responsible for hundreds of thousands of deaths worldwide. Few studies have evaluated the utility of real-time reverse transcription-PCR to detect influenza virus RNA from formalin-fixed, paraffin-embedded tissues obtained at autopsy. In this work, respiratory autopsy tissues from 442 suspect influenza cases were tested by real-time reverse transcription-PCR for seasonal influenza A and B and 2009 pandemic influenza A (H1N1) viruses and the results were compared to those obtained by immunohistochemistry. In total, 222 cases were positive by real-time reverse transcription-PCR, and of 218 real-time, reverse transcription-PCR-positive cases also tested by immunohistochemistry, only 107 were positive. Although formalin-fixed, paraffin-embedded tissues can be used for diagnosis, frozen tissues offer the best chance to make a postmortem diagnosis of influenza because these tissues possess nucleic acids that are less degraded and, as a consequence, provide longer sequence information than that obtained from fixed tissues. We also determined that testing of all available respiratory tissues is critical for optimal detection of influenza virus in postmortem tissues.
Influenza viruses (Orthomyxoviridae family) are negative-sense, single-strand RNA viruses. There are three genera of influenza viruses: A, B, and C. Influenza A and B are more common and cause respiratory illness of increased severity, whereas influenza C is thought to result in a milder upper respiratory tract infection.1,2 Although there are only two lineages of influenza B (Yamagata and Victoria),3 the influenza A viruses are characterized further by their hemagglutinin and neuraminidase into subtypes, with 16 different hemagglutinin and 9 different neuraminidase subtypes.4 Seasonal influenza infections are caused primarily by influenza A/H1N1, A/H3N2, and both lineages of influenza B,5 and have been estimated to cause greater than 200,000 hospitalizations and 36,000 deaths each year in the United States.6–8 Severe complications often arise from influenza infection, which include secondary bacterial pneumonia, viral myocarditis, and encephalitis.6,9–11 The recent pandemic, caused by a novel H1N1 influenza A virus [2009 pandemic influenza A (H1N1)],12,13 has claimed thousands of lives worldwide and has continued to cause disease throughout the traditional influenza season. The ability to easily distinguish the genera and subtypes of influenza infections responsible for mortality is becoming increasingly important.
Diagnostic assays for influenza infection are numerous and include, among others, culture and direct fluorescent antibody staining,14–17 conventional reverse transcription-PCR (RT-PCR) and real-time RT-PCR (rRT-PCR),14,15,17–23 microarrays,5,15,16,19 and a large number of commercially available rapid diagnostic tests.19,24,25 However, these assays have diverse ranges in sensitivity and specificity, depending on the nature of the sample and duration of illness.6 Further, specimens sampled for testing are typically sputum, swabs of the throat, and nasopharyngeal aspirates, swabs, and washes.4
Detection of influenza RNA in frozen postmortem specimens is relatively straightforward,26 and has even been used in the detection and sequencing of the 1918 influenza virus genes from human bodies frozen in the permafrost.27 Molecular analyses on formalin-fixed tissues, particularly those that require RNA, can be quite difficult because formalin fixation strongly cross-links nucleic acids, and the embedding process can introduce ribonucleases, resulting in significant RNA degradation and smaller amplifiable fragments.28,29 Most research that demonstrates evidence of the influenza virus in formalin-fixed or formalin-fixed, paraffin-embedded (FFPE) tissues from fatal human seasonal influenza cases has used assays such as immunohistochemistry (IHC),30 in situ hybridization,31 or conventional RT-PCR.26,32–36 However, because of the amplicon size limitations presented by FFPE tissues, rRT-PCR methods for detection of pathogens are the most ideal. Although recent reports containing limited details of the detection of influenza by conventional RT-PCR37 and rRT-PCR38–40 in FFPE tissues have been published, there are no detailed reports describing routine methods to extract RNA from and performance of rRT-PCR to detect influenza A, its H1 and H3 subtypes, and influenza B in FFPE autopsy tissues. We also compared IHC assays to rRT-PCR to routinely characterize postmortem influenza infections.
Materials and Methods
Specimen Information
Respiratory tissues from 442 cases suspected for influenza infection by clinical history or on histological review at the Centers for Disease Control (CDC) were included in this study. Clinical features of suspect seasonal influenza include high fever, cough, headache, coryza, prostration, malaise, and pneumonic involvement in some cases. Some histopathological features of seasonal influenza include tracheobronchitis, bronchopneumonia, and interstitial pneumonitis.2 Clinical and histopathological features of 2009 H1N1 have been described previously.37,40 Autopsy reports were reviewed when available.
RNA Extraction and rRT-PCR
Ten-μm sections were cut from blocks containing FFPE tissues and placed into microcentrifuge tubes using RNase-free conditions. Control tubes lacking tissue were included during the extraction process to ensure no reagent contamination occurred. The tissue sections were deparaffinized with xylene and washed twice with absolute ethanol. After allowing the residual ethanol to evaporate for 10 minutes, 130 μL of Buffer PKD (Qiagen, Valencia, CA) and 10 μL of proteinase K (Qiagen) were added to each tissue sample. The tissues were homogenized with a pellet pestle and allowed to digest for 15 minutes at 55°C, then at 45°C overnight. The samples were incubated at 80°C for 15 minutes, followed by centrifugation at 16,000 × g for 3 minutes to pellet any undigested material. The supernatant was transferred to an appropriate tube for placement onto either Qiagen's BioRobot EZ1 (using the EZ1 RNA Tissue Mini Kit and EZ1 RNA card) or BioRobot M48 (using the MagAttract RNA Tissue Mini M48 Kit and the Gene Expression Application Package's Total RNA Tissue Protocol), and the RNA was eluted into a 50-μL volume.
Frozen tissue samples (about 1 mm3 to 3 mm3 in size) were minced and placed into a microcentrifuge tube containing 300 μL of buffer RLT (Qiagen). Tubes containing only buffer RLT were used as extraction controls to ensure no contamination of reagents occurred. Tissues were homogenized further using a pellet pestle, and the lysate then was passed through a QIAshredder column (Qiagen). The RNeasy Mini Kit (Qiagen) was used to complete the RNA extraction as per the provided protocol, with the RNA eluted into a final volume of 50 μL of RNase-free water.
The CDC rRT-PCR influenza assay is designed to detect influenza A and influenza B viruses and characterizes influenza A–positive samples as either seasonal H1 or H3 (unpublished protocol, details are available from the CDC on request). To detect 2009 H1N1 in samples, the CDC's rRT-PCR Protocol for Detection and Characterization of Swine Influenza (available from the World Health Organization, http://www.who.int/csr/resources/publications/swineflu/CDCRealtimeRTPCR_SwineH1Assay-2009_20090430.pdf, accessed May 14, 2010) was used, which contains cycling conditions and primers/probes for the universal detection of influenza A, swine influenza A, and swine-like H1. For influenza A cases received during 2009 that could not be subtyped by the CDC assays, primers and probes from a recently published assay,23 which discriminates seasonal H1 from novel H1 in a single tube, were used with modified cycling conditions as follows: 30 minutes reverse transcription at 50°C, 2 minutes incubation at 95°C, and 45 cycles of 95°C for 15 seconds and 60°C for 1 minute. All reactions were performed with 5 μL of RNA extract and the Superscript III Platinum One-Step qRT-PCR Kit (Invitrogen, Carlsbad, CA) on the Stratagene Mx3000P or Mx3005P QPCR System. RNase P or B2-microglobulin41 was used as an internal control to ensure effective RNA extraction; samples having threshold cycle values of 40 or fewer for these targets were considered adequate for influenza testing.
Immunohistochemistry
IHC assays for influenza A (including 2009 H1N1 influenza A) and influenza B, when sufficient tissues were available, were performed on 3-μm sections of FFPE tissues from the trachea/bronchi and peripheral lung as previously described.31,40,42 Primary antibodies were detected using the Ultra Vision LP Detection System with Alkaline Phosphatase Polymer and Fast Red Chromogen (Lab Vision, Fremont, CA) or the LSAB2-labeled streptavidin biotin system with biotinylated link antibody, alkaline phosphatase-labeled streptavidin (Dako, Carpinteria, CA), and Fast Red Chromogen (Dako). Counterstaining was performed with Mayer's hematoxylin (Fisher Scientific, Pittsburgh, PA). IHC evaluation criteria have been described previously.31,40,43
Results
The 442 cases tested in this study were obtained between 2000 and 2009, and the patients ranged in age from 10 days to 84 years (median, 25 years). These patients came from 44 different states plus 1 patient from the District of Columbia and 9 patients from Puerto Rico. Suspect influenza cases received between 2000 and 2008 and tested by rRT-PCR totaled 137; 70 cases were negative, 9 were seasonal influenza A/H1, 21 were influenza A/H3, 3 were influenza A/unsubtypeable, and 34 were influenza B. A total of 305 cases were received in 2009; 150 cases were negative, 10 were seasonal influenza A/H1, 2 were influenza A/H3, 8 were influenza A/unsubtypeable, 9 were influenza B, and 126 were 2009 H1N1. In total, 222 cases were positive by rRT-PCR for influenza.
A comparison of IHC to rRT-PCR (seasonal and 2009 H1N1) is shown in Table 1, and representative photomicrographs of IHCs for seasonal influenza A, influenza B, and 2009 H1N1 influenza are shown in Figure 1, A, B, and C, respectively. Of 218 rRT-PCR–positive cases also tested by IHC, 107 (49%) were IHC positive. Only one case from 2009 was positive by IHC but negative by rRT-PCR. In 138 of the 218 rRT-PCR–positive cases that also were tested by IHC, both IHC and rRT-PCR were performed on the same FFPE blocks. Eighty blocks were both IHC and rRT-PCR positive, 8 blocks were IHC positive but rRT-PCR negative, 96 blocks were IHC negative but rRT-PCR positive, and 77 blocks were negative by both assays. Calculations using this data demonstrate a sensitivity of 45% for IHC (confidence interval, 38% to 53% by the Newcombe-Wilson method).44 Of 176 rRT-PCR–positive cases with a known duration of illness and IHC results, 75 of 136 (55%) cases with a duration of 10 days or fewer were positive by IHC and only 8 of 40 (20%) cases with a duration of more than 10 days were IHC positive. The dependency of the IHC result on an illness duration of 10 days or fewer was statistically significant by χ2 analysis (P < 0.0001). This dependency of duration of illness is stronger for IHC than it is for rRT-PCR.40
Table 1.
IHC Results Among 218 rRT-PCR–Positive Cases⁎
| IHC result |
||
|---|---|---|
| rRT-PCR result | Positive | Negative |
| 2009 H1N1 | 60 | 63 |
| Seasonal influenza A/H1 | 6 | 13 |
| Seasonal influenza A/H3 | 13 | 10 |
| A/unsubtypeable | 2 | 8 |
| B | 26 | 17 |
| Total | 107† | 111 |
Four rRT-PCR–positive cases (3 were 2009 H1N1, 1 was A/unsubtypeable) were not tested by IHC because of insufficient amounts of tissue for testing.
One IHC-positive case included in the study was rRT-PCR negative.
Figure 1.
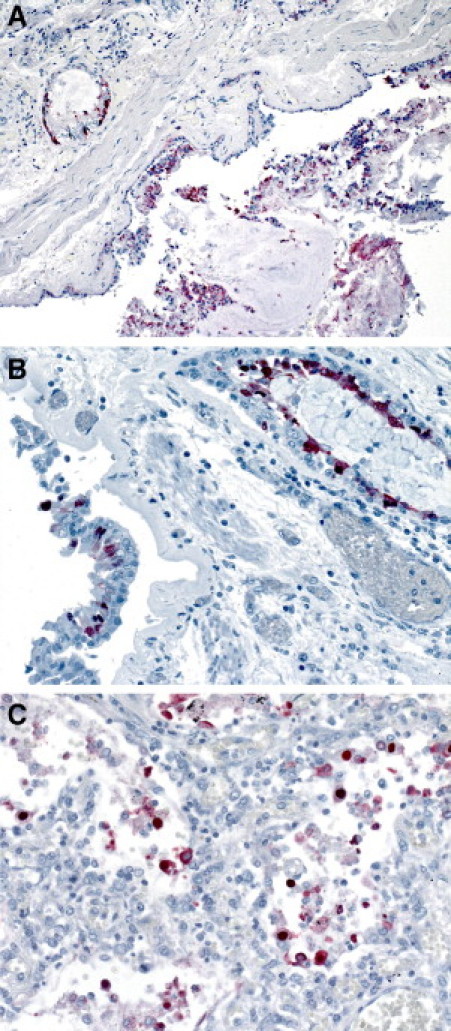
Representative immunohistochemistry staining for seasonal (A and B) and 2009 H1N1 influenza (C). Viral antigens are seen in respiratory epithelial cells and in submucosal glands in seasonal influenza A/H1 (original magnification, 10×) (A) and influenza B–positive cases (original magnification, 20×) (B). C: In 2009 H1N1 influenza A cases, viral antigens are observed in alveolar lining cells, including type I and II pneumocytes (original magnification, 20×).
By examination of the medical records submitted from 220 of the rRT-PCR–positive cases that had sufficient medical history, the number of cases also tested for influenza by techniques other than rRT-PCR of autopsy tissues was assessed. A diagnosis had been made using other specimens (ie, rRT-PCR of RNA from a nasopharyngeal swab, culture, rapid antigen test, etc) from 136 cases, and testing of the autopsy tissues served to confirm the diagnosis of influenza by detection of influenza RNA in the tissues. In 84 cases a diagnosis of influenza infection as a contributor to the death of the patient was obtained solely by testing of autopsy tissues with rRT-PCR because other tests were either negative or had not been performed. If IHC of the autopsy tissues had been used solely, only 42 cases would have received a diagnosis.
Both frozen and FFPE tissues were used to obtain RNA extracts for testing. All tissues tested from 2000 to 2008, except from a single case, were from FFPE tissues. The number of cases from 2009 tested using frozen tissues only, FFPE tissues only, or both frozen and FFPE tissues are summarized in Table 2 along with their rRT-PCR results. When possible, rRT-PCR testing for 2009 H1N1 was performed using frozen tissues because of the ease and speed with which the tissues could be extracted and tested. In this study, 52 cases were positive for 2009 H1N1 based on results from FFPE tissues alone, 74 cases were positive based on results from frozen tissues, and 24 of those cases also had corresponding FFPE tissues that were tested. Of those 24, the FFPE tissues from 18 cases also were positive, whereas the FFPE tissues were negative in the remaining 6 cases.
Table 2.
Number of Cases Tested by rRT-PCR Using FFPE and Frozen Autopsy Tissues in 2009
| rRT-PCR result | FFPE only tested | Frozen only tested | Both FFPE and frozen tested |
|---|---|---|---|
| Seasonal influenza A/H1 | 10 | 0 | 0 |
| Seasonal influenza A/H3 | 2 | 0 | 0 |
| 2009 H1N1 | 52 | 50 | 24⁎ |
| A/unsubtypeable | 8 | 0 | 0 |
| B | 9 | 0 | 0 |
| Negative | 108 | 38 | 4 |
| Total | 189 | 88 | 28 |
Although 24 cases ultimately were tested using frozen and FFPE tissues, 18 were positive in both frozen and FFPE tissues, whereas 6 cases were positive in the frozen tissue but negative in the FFPE tissue.
Tissues from either trachea/bronchi, peripheral lung, or both (in both frozen and FFPE forms) routinely were tested by rRT-PCR for influenza when provided by the submitter. In 15 cases of seasonal influenza, both trachea/bronchi and peripheral lung were available on different blocks of FFPE tissues such that comparisons could be made to determine the best tissue type for future rRT-PCR analyses. In seven cases, rRT-PCR positives were found in the trachea and bronchi whereas peripheral lung was negative. Five cases were rRT-PCR positive in the peripheral lung only, whereas the remaining three cases were positive in both portions of the airway. With respect to 2009 H1N1, a similar analysis was performed on 30 cases from throughout the pandemic. Twelve cases were positive only in the trachea/bronchi, 6 were positive only in the peripheral lung, and 12 cases were positive in trachea/bronchi and peripheral lung.
Discussion
The detection of influenza viruses by RT-PCR in formalin-fixed tissues has been explored with limited detail,35–38 and has potential for great utility in diagnostic pathology. In this work, we demonstrate that both human seasonal influenza and 2009 H1N1 influenza viruses can be detected in FFPE tissues using the CDC's TaqMan assays, both of which have been widely distributed to state and local entities for seasonal and 2009 H1N1 influenza testing.13,45 In 35 cases in which subtyping could not be accomplished using the CDC assay, addition of a subtyping rRT-PCR assay that detects both seasonal H1 and 2009 H1N1 in a single tube aided in making definitive diagnoses in 26 of those cases. It is possible that subtyping could not be accomplished with the CDC assay in the 35 cases obtained during the 2009 H1N1 pandemic because of mismatches in the H1 hemagglutinin sequence in which the reverse primer anneals.23 For the eight cases that still could not be subtyped, in most instances the influenza A threshold cycle values were close to the cut-off of 40, implying that the viral titer in the sample was quite low and near the limit of detection.
When compared to IHC, rRT-PCR is better able to detect influenza; of the 218 positive cases detected by rRT-PCR that also were tested by IHC, only 107 were positive by IHC. Only one case was positive by IHC but negative by rRT-PCR, likely because there was insufficient tissue remaining when processed for rRT-PCR. This enhanced detection by rRT-PCR may be owing to the results presented here that suggest that positive IHC results are more dependent on the duration of illness because the viral antigens in the tissues may be cleared by the host immune response after 10 days, whereas rRT-PCR can detect small amounts of nucleic acids remaining in tissues after 10 days.40
In general, detection of influenza nucleic acid in FFPE tissues can be accomplished but is optimal when fixation time is kept to a minimum. However, we have seen one positive case, which tested positive for influenza A but could not be subtyped further, for which tissues were stored in formalin for 11 months. More often than not, overfixation results in an inability to obtain viable RNA from tissue specimens, as determined by positive housekeeping gene control rRT-PCR. Further, samples fixed in formalin at concentrations greater than 10%, which may occur under unusual circumstances, or where extensive tissue degradation has occurred, often do not provide rRT-PCR–positive results with the housekeeping gene control (data not shown), indicating the RNA is of insufficient quality for analysis. Studies examining tissue fixation times and processing after collection suggest that fixation should commence as soon as possible but proceed no longer than 48 hours after collection.46,47 With these data in mind, standardized protocols for efficient and effective tissue fixation and processing should be made available to pathologists and other public health professionals worldwide so as to provide high-quality tissue specimens that are ideal for use in both IHC and rRT-PCR assays.
Of the cases that tested positive in this study by rRT-PCR, 38% had no other testing performed as discerned by analysis of accompanying medical records. Without testing of the autopsy tissues by rRT-PCR, a definitive diagnosis may not have been made on these cases; if IHC testing of the autopsy tissues had been performed alone, only 19% of the cases identified in this series would have received a positive diagnosis. Furthermore, additional analyses of autopsy tissues by PCR and IHC for secondary bacterial infections can help to ascertain whether influenza was the primary cause of death or if other contributing factors were likely, thereby more precisely determining the cause of death. As witnessed by the 2009 H1N1 influenza outbreak, active surveillance and testing is critical in detecting novel infectious diseases early.48 Routine testing and evaluation of autopsy tissues could help identify novel outbreaks of disease.43,49,50 Several excellent programs have created surveillance systems to examine fatal cases with possible infectious etiologies.51,52
This study also demonstrates that, although testing of FFPE tissues is useful, testing of frozen autopsy tissues provides the best chance for establishing a diagnosis. In this study, of the 24 rRT-PCR–positive cases in which both frozen and FFPE tissues were tested, 6 cases would have been deemed negative if only FFPE tissues had been available for analysis. Although the sample set is small, this suggests that a possible 25% of cases could be missed if analyzing FFPE tissues alone. Furthermore, frozen tissues are beneficial for sequencing of influenza RNA because much longer sequences can be obtained from frozen tissues with less effort than those from FFPE tissues. In addition, especially when using FFPE tissues for analysis, there is a necessity for testing both trachea/bronchi and lung parenchyma, when available, by rRT-PCR to optimize the chances of detecting influenza. In the absence of pronounced gross pathology or when the degree of pathology cannot be assessed, as was sometimes the case in this study because these samples were submitted to the CDC for evaluation by state and local entities, there is a need to test all available respiratory tissues.
Although 93% of the FFPE tissue specimens used for this study were obtained between the years of 2007 and 2009, there are instances of older cases in which suspicion of influenza remains although a diagnosis has been elusive. This work and other studies have demonstrated that RNA can be obtained from archived FFPE tissues, and evidence has been presented on the identification of influenza viral RNA using RT-PCR and sequencing of small products.35,36,53 With the large number of FFPE blocks available for retrospective studies, this opens a greater opportunity for research into influenza pathogenesis and other host–pathogen relationship studies.
Acknowledgments
We thank Amy Greene for her assistance with IHCs and analysis of medical records, Reema P. Dedania for her assistance with IHC, and Eric Shattuck for his assistance with RNA extractions. We also thank the state health departments and clinicians who contributed specimens to the Infectious Diseases Pathology Branch of the CDC. The work presented here was completed as part of routine public health studies performed at the CDC.
Footnotes
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the CDC.
References
- 1.Hirsila M., Kauppila J., Tuomaala K., Grekula B., Puhakka T., Ruuskanen O., Ziegler T. Detection by reverse transcription-polymerase chain reaction of influenza C in nasopharyngeal secretions of adults with a common cold. J Infect Dis. 2001;183:1269–1272. doi: 10.1086/319675. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Taubenberger J.K., Morens D.M. The pathology of influenza virus infections. Annu Rev Pathol. 2008;3:499–522. doi: 10.1146/annurev.pathmechdis.3.121806.154316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Rota P.A., Wallis T.R., Harmon M.W., Rota J.S., Kendal A.P., Nerome K. Cocirculation of two distinct evolutionary lineages of influenza type B virus since 1983. Virology. 1990;175:59–68. doi: 10.1016/0042-6822(90)90186-u. [DOI] [PubMed] [Google Scholar]
- 4.Petric M., Comanor L., Petti C.A. Role of the laboratory in diagnosis of influenza during seasonal epidemics and potential pandemics. J Infect Dis. 2006;194(Suppl 2):S98–S110. doi: 10.1086/507554. [DOI] [PubMed] [Google Scholar]
- 5.Huang Y., Tang H., Duffy S., Hong Y., Norman S., Ghosh M., He J., Bose M., Henrickson K.J., Fan J., Kraft A.J., Weisburg W.G., Mather E.L. Multiplex assay for simultaneously typing and subtyping influenza viruses by use of an electronic microarray. J Clin Microbiol. 2009;47:390–396. doi: 10.1128/JCM.01807-08. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Beigel J.H. Influenza. Crit Care Med. 2008;36:2660–2666. doi: 10.1097/CCM.0b013e318180b039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Thompson W.W., Comanor L., Shay D.K. Epidemiology of seasonal influenza: use of surveillance data and statistical models to estimate the burden of disease. J Infect Dis. 2006;194(Suppl 2):S82–S91. doi: 10.1086/507558. [DOI] [PubMed] [Google Scholar]
- 8.Thompson W.W., Shay D.K., Weintraub E., Brammer L., Cox N., Anderson L.J., Fukuda K. Mortality associated with influenza and respiratory syncytial virus in the United States. JAMA. 2003;289:179–186. doi: 10.1001/jama.289.2.179. [DOI] [PubMed] [Google Scholar]
- 9.Mamas M.A., Fraser D., Neyses L. Cardiovascular manifestations associated with influenza virus infection. Int J Cardiol. 2008;130:304–309. doi: 10.1016/j.ijcard.2008.04.044. [DOI] [PubMed] [Google Scholar]
- 10.Finelli L., Fiore A., Dhara R., Brammer L., Shay D.K., Kamimoto L., Fry A., Hageman J., Gorwitz R., Bresee J., Uyeki T. Influenza-associated pediatric mortality in the United States: increase of Staphylococcus aureus coinfection. Pediatrics. 2008;122:805–811. doi: 10.1542/peds.2008-1336. [DOI] [PubMed] [Google Scholar]
- 11.Lee N., Wong C.K., Chan P.K., Lindegardh N., White N.J., Hayden F.G., Wong E.H., Wong K.S., Cockram C.S., Sung J.J., Hui D.S. Acute encephalopathy associated with influenza A infection in adults. Emerg Infect Dis. 2010;16:139–142. doi: 10.3201/eid1601.090077. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Garten R.J., Davis C.T., Russell C.A., Shu B., Lindstrom S., Balish A., Sessions W.M., Xu X., Skepner E., Deyde V., Okomo-Adhiambo M., Gubareva L., Barnes J., Smith C.B., Emery S.L., Hillman M.J., Rivailler P., Smagala J., de Graaf M., Burke D.F., Fouchier R.A., Pappas C., Alpuche-Aranda C.M., Lopez-Gatell H., Olivera H., Lopez I., Myers C.A., Faix D., Blair P.J., Yu C., Keene K.M., Dotson P.D., Jr, Boxrud D., Sambol A.R., Abid S.H., ST George K., Bannerman T., Moore A.L., Stringer D.J., Blevins P., Demmler-Harrison G.J., Ginsberg M., Kriner P., Waterman S., Smole S., Guevara H.F., Belongia E.A., Clark P.A., Beatrice S.T., Donis R., Katz J., Finelli L., Bridges C.B., Shaw M., Jernigan D.B., Uyeki T.M., Smith D.J., Klimov A.I., Cox N.J. Antigenic and genetic characteristics of swine-origin 2009 A (H1N1) influenza viruses circulating in humans. Science. 2009;325:197–201. doi: 10.1126/science.1176225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Dawood F.S., Jain S., Finelli L., Shaw M.W., Lindstrom S., Garten R.J., Gubareva L.V., Xu X., Bridges C.B., Uyeki T.M. Emergence of a novel swine-origin influenza A (H1N1) virus in humans. N Engl J Med. 2009;360:2605–2615. doi: 10.1056/NEJMoa0903810. [DOI] [PubMed] [Google Scholar]
- 14.Gharabaghi F., Tellier R., Cheung R., Collins C., Broukhanski G., Drews S.J., Richardson S.E. Comparison of a commercial qualitative real-time RT-PCR kit with direct immunofluorescence assay (DFA) and cell culture for detection of influenza A and B in children. J Clin Virol. 2008;42:190–193. doi: 10.1016/j.jcv.2008.01.013. [DOI] [PubMed] [Google Scholar]
- 15.Chiu C.Y., Urisman A., Greenhow T.L., Rouskin S., Yagi S., Schnurr D., Wright C., Drew W.L., Wang D., Weintrub P.S., DeRisi J.L., Ganem D. Utility of DNA microarrays for detection of viruses in acute respiratory tract infections in children. J Pediatr. 2008;153:76–83. doi: 10.1016/j.jpeds.2007.12.035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Takahashi H., Norman S.A., Mather E.L., Patterson B.K. Evaluation of the NanoChip 400 system for detection of influenza A and B, respiratory syncytial, and parainfluenza viruses. J Clin Microbiol. 2008;46:1724–1727. doi: 10.1128/JCM.01947-07. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Percivalle E., Rovida F., Piralla A., Rognoni V., Zavattoni M., Baldanti F., Marchi A., Gerna G. Rapid typing, subtyping and RNA quantification of influenza virus type A strains in respiratory secretions. New Microbiol. 2008;31:319–327. [PubMed] [Google Scholar]
- 18.Hymas W.C., Hillyard D.R. Evaluation of Nanogen MGB Alert detection reagents in a multiplex real-time PCR for influenza virus types A and B and respiratory syncytial virus. J Virol Methods. 2009;156:124–128. doi: 10.1016/j.jviromet.2008.11.004. [DOI] [PubMed] [Google Scholar]
- 19.Mehlmann M., Bonner A.B., Williams J.V., Dankbar D.M., Moore C.L., Kuchta R.D., Podsiad A.B., Tamerius J.D., Dawson E.D., Rowlen K.L. Comparison of the MChip to viral culture, reverse transcription-PCR, and the QuickVue influenza A+B test for rapid diagnosis of influenza. J Clin Microbiol. 2007;45:1234–1237. doi: 10.1128/JCM.02202-06. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Carr M.J., Gunson R., Maclean A., Coughlan S., Fitzgerald M., Scully M., O'Herlihy B., Ryan J., O'Flanagan D., Connell J., Carman W.F., Hall W.W. Development of a real-time RT-PCR for the detection of swine-lineage influenza A (H1N1) virus infections. J Clin Virol. 2009;45:196–199. doi: 10.1016/j.jcv.2009.06.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Poon L.L., Chan K.H., Smith G.J., Leung C.S., Guan Y., Yuen K.Y., Peiris J.S. Molecular detection of a novel human influenza (H1N1) of pandemic potential by conventional and real-time quantitative RT-PCR assays. Clin Chem. 2009;55:1555–1558. doi: 10.1373/clinchem.2009.130229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Whiley D.M., Bialasiewicz S., Bletchly C., Faux C.E., Harrower B., Gould A.R., Lambert S.B., Nimmo G.R., Nissen M.D., Sloots T.P. Detection of novel influenza A (H1N1) virus by real-time RT-PCR. J Clin Virol. 2009;45:203–204. doi: 10.1016/j.jcv.2009.05.032. [DOI] [PubMed] [Google Scholar]
- 23.Wang R., Sheng Z.M., Taubenberger J.K. Detection of novel (swine origin) H1N1 influenza A virus by quantitative real-time reverse transcription-PCR. J Clin Microbiol. 2009;47:2675–2677. doi: 10.1128/JCM.01087-09. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Chan K.H., Maldeis N., Pope W., Yup A., Ozinskas A., Gill J., Seto W.H., Shortridge K.F., Peiris J.S.M. Evaluation of the Directigen Flu A+B test for rapid diagnosis of influenza virus type A and B infections. J Clin Microbiol. 2002;40:1675–1680. doi: 10.1128/JCM.40.5.1675-1680.2002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Dale S.E., Mayer C., Mayer M.C., Menegus M.A. Analytical and clinical sensitivity of the 3M rapid detection influenza A+B assay. J Clin Microbiol. 2008;46:3804–3807. doi: 10.1128/JCM.01779-08. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Bajanowski T., Rolf B., Jorch G., Brinkmann B. Detection of RNA viruses in sudden infant death (SID) Int J Legal Med. 2003;117:237–240. doi: 10.1007/s00414-003-0367-6. [DOI] [PubMed] [Google Scholar]
- 27.Taubenberger J.K., Reid A.H., Lourens R.M., Wang R., Jin G., Fanning T.G. Characterization of the 1918 influenza virus polymerase genes. Nature. 2005;437:889–893. doi: 10.1038/nature04230. [DOI] [PubMed] [Google Scholar]
- 28.McKinney M.D., Moon S.J., Kulesh D.A., Larsen T., Schoepp R.J. Detection of viral RNA from paraffin-embedded tissues after prolonged formalin fixation. J Clin Virol. 2009;44:39–42. doi: 10.1016/j.jcv.2008.09.003. [DOI] [PubMed] [Google Scholar]
- 29.Foss R.D., Guha-Thakurta N., Conran R.M., Gutman P. Effects of fixative and fixation time on the extraction and polymerase chain reaction amplification of RNA from paraffin-embedded tissue: Comparison of two housekeeping gene mRNA controls. Diagn Mol Pathol. 1994;3:148–155. doi: 10.1097/00019606-199409000-00003. [DOI] [PubMed] [Google Scholar]
- 30.Guarner J., Paddock C.D., Shieh W.J., Packard M.M., Patel M., Montague J.L., Uyeki T.M., Bhat N., Balish A., Lindstrom S., Klimov A., Zaki S.R. Histopathologic and immunohistochemical features of fatal influenza virus infection in children during the 2003–2004 season. Clin Infect Dis. 2006;43:132–140. doi: 10.1086/505122. [DOI] [PubMed] [Google Scholar]
- 31.Guarner J., Shieh W.J., Dawson J., Subbarao K., Shaw M., Ferebee T., Morken T., Nolte K.B., Freifeld A., Cox N., Zaki S.R. Immunohistochemical and in situ hybridization studies of influenza A virus infection in human lungs. Am J Clin Pathol. 2000;114:227–233. doi: 10.1309/HV74-N24T-2K2C-3E8Q. [DOI] [PubMed] [Google Scholar]
- 32.Bowles N.E., Ni J., Kearney D.L., Pauschinger M., Schultheiss H.-P., McCarthy R., Hare J., Bricker J.T., Bowles K.R., Towbin J.A. Detection of viruses in myocardial tissues by polymerase chain reaction: evidence of adenovirus as a common cause of myocarditis in children and adults. J Am Coll Cardiol. 2003;42:466–472. doi: 10.1016/s0735-1097(03)00648-x. [DOI] [PubMed] [Google Scholar]
- 33.Takahashi M., Yamada T., Nakashita Y., Saikusa H., Deguchi M., Kida H., Tashiro M., Toyoda T. Influenza virus-induced encephalopathy: clinicopathologic study of an autopsied case. Pediatr Int. 2000;42:204–214. doi: 10.1046/j.1442-200x.2000.01203.x. [DOI] [PubMed] [Google Scholar]
- 34.Kyto V., Vuorinen T., Saukko P., Lautenschlager I., Lignitz E., Saraste A., Voipio-Pulkki L.-M. Cytomegalovirus infection of the heart is common in patients with fatal myocarditis. Clin Infect Dis. 2005;40:683–688. doi: 10.1086/427804. [DOI] [PubMed] [Google Scholar]
- 35.Reid A.H., Fanning T.G., Hultin J.V., Taubenberger J.K. Origin and evolution of the 1918 “Spanish” influenza virus hemagglutinin gene. Proc Natl Acad Sci U S A. 1999;96:1651–1656. doi: 10.1073/pnas.96.4.1651. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Taubenberger J.K., Reid A.H., Krafft A.E., Bijwaard K.E., Fanning T.G. Initial genetic characterization of the 1918 “Spanish” influenza virus. Science. 1997;275:1793–1796. doi: 10.1126/science.275.5307.1793. [DOI] [PubMed] [Google Scholar]
- 37.Mauad T., Hajjar L.A., Callegari G.D., da Silva L.F., Schout D., Galas F.R., Alves V.A., Malheiros D.M., Auler J.O., Jr, Ferreira A.F., Borsato M.R., Bezerra S.M., Gutierrez P.S., Caldini E.T., Pasqualucci C.A., Dolhnikoff M., Saldiva P.H. Lung pathology in fatal novel human influenza A (H1N1) infection. Am J Respir Crit Care Med. 2010;181:72–79. doi: 10.1164/rccm.200909-1420OC. [DOI] [PubMed] [Google Scholar]
- 38.Gu J., Xie Z., Gao Z., Liu J., Korteweg C., Ye J., Lau L.T., Lu J., Zhang B., McNutt M.A., Lu M., Anderson V.M., Gong E., Yu A.C., Lipkin W.I. H5N1 infection of the respiratory tract and beyond: a molecular pathology study. Lancet. 2007;370:1137–1145. doi: 10.1016/S0140-6736(07)61515-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Gill J.R., Sheng Z.M., Ely S.F., Guinee D.G., Beasley M.B., Suh J., Deshpande C., Mollura D.J., Morens D.M., Bray M., Travis W.D., Taubenberger J.K. Pulmonary pathologic findings of fatal 2009 pandemic influenza A/H1N1 viral infections. Arch Pathol Lab Med. 2010;134:235–243. doi: 10.5858/134.2.235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Shieh W.J., Blau D.M., Denison A.M., Deleon-Carnes M., Adem P., Bhatnagar J., Sumner J., Liu L., Patel M., Batten B., Greer P., Jones T., Smith C., Bartlett J., Montague J., White E., Rollin D., Gao R., Seales C., Jost H., Metcalfe M., Goldsmith C.S., Humphrey C., Schmitz A., Drew C., Paddock C., Uyeki T.M., Zaki S.R. 2009 pandemic influenza A (H1N1): pathology and pathogenesis of 100 fatal cases in the United States. Am J Pathol. 2010;177:166–175. doi: 10.2353/ajpath.2010.100115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Watzinger F., Suda M., Preuner S., Baumgartinger R., Ebner K., Baskova L., Niesters H.G., Lawitschka A., Lion T. Real-time quantitative PCR assays for detection and monitoring of pathogenic human viruses in immunosuppressed pediatric patients. J Clin Microbiol. 2004;42:5189–5198. doi: 10.1128/JCM.42.11.5189-5198.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Paddock C., Shieh W.J., Guarner J., Uyeki T.M., Fischer M., Reagan S., Park B., Greer P., Packard M., Zaki S. Histopathology and immunohistochemical localization of influenza virus in patients with fatal influenza B (abstract 1218) Mod Pathol. 2005;18(Suppl 1S):263A. [Google Scholar]
- 43.Guarner J., Zaki S.R. Histopathology and immunohistochemistry in the diagnosis of bioterrorism agents. J Histochem Cytochem. 2006;54:3–11. doi: 10.1369/jhc.5R6756.2005. [DOI] [PubMed] [Google Scholar]
- 44.Newcombe R.G. Improved confidence intervals for the difference between binomial proportions based on paired data. Stat Med. 1998;17:2635–2650. [PubMed] [Google Scholar]
- 45.Jamieson D.J., Honein M.A., Rasmussen S.A., Williams J.L., Swerdlow D.L., Biggerstaff M.S., Lindstrom S., Louie J.K., Christ C.M., Bohm S.R., Fonseca V.P., Ritger K.A., Kuhles D.J., Eggers P., Bruce H., Davidson H.A., Lutterloh E., Harris M.L., Burke C., Cocoros N., Finelli L., MacFarlane K.F., Shu B., Olsen S.J. H1N1 2009 influenza virus infection during pregnancy in the USA. Lancet. 2009;374:451–458. doi: 10.1016/S0140-6736(09)61304-0. [DOI] [PubMed] [Google Scholar]
- 46.Chung J.Y., Braunschweig T., Williams R., Guerrero N., Hoffmann K.M., Kwon M., Song Y.K., Libutti S.K., Hewitt S.M. Factors in tissue handling and processing that impact RNA obtained from formalin-fixed, paraffin-embedded tissue. J Histochem Cytochem. 2008;56:1033–1042. doi: 10.1369/jhc.2008.951863. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.von Ahlfen S., Missel A., Bendrat K., Schlumpberger M. Determinants of RNA quality from FFPE samples. PLoS One. 2007;2:e1261. doi: 10.1371/journal.pone.0001261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Centers for Disease Control and Prevention Swine influenza A (H1N1) infection in two children—Southern California, March-April 2009. MMWR Morb Mortal Wkly Rep. 2009;58:400–402. [PubMed] [Google Scholar]
- 49.Zaki S.R., Greer P.W., Coffield L.M., Goldsmith C.S., Nolte K.B., Foucar K., Feddersen R.M., Zumwalt R.E., Miller G.L., Khan A.S., Rollin P.E., Ksiazek T.G., Nichol S.T., Mahy B.W.J., Peters C.J. Hantavirus pulmonary syndrome: Pathogenesis of an emerging infectious disease. Am J Pathol. 1995;146:552–579. [PMC free article] [PubMed] [Google Scholar]
- 50.Shieh W.J., Guarner J., Layton M., Fine A., Miller J., Nash D., Campbell G.L., Roehrig J.T., Gubler D.J., Zaki S.R. The role of pathology in an investigation of an outbreak of West Nile encephalitis in New York, 1999. Emerg Infect Dis. 2000;6:370–372. doi: 10.3201/eid0604.000407. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.DeVries A., Lees C., Rainbow J., Lynfield R. Explaining the unexplained: identifying infectious causes of critical illness and death in Minnesota. Minn Med. 2008;91:34–36. [PubMed] [Google Scholar]
- 52.Nolte K.B., Lathrop S.L., Nashelsky M.B., Nine J.S., Gallaher M.M., Umland E.T., McLemore J.L., Reichard R.R., Irvine R.A., McFeeley P.J., Zumwalt R.E. “Med-X”: a medical examiner surveillance model for bioterrorism and infectious disease mortality. Hum Pathol. 2007;38:718–725. doi: 10.1016/j.humpath.2007.02.003. [DOI] [PubMed] [Google Scholar]
- 53.Ribeiro-Silva A., Zhang H., Jeffrey S. RNA extraction from ten year old formalin-fixed paraffin-embedded breast cancer samples: a comparison of column purification and magnetic bead-based technologies. BMC Mol Biol. 2007;8:118. doi: 10.1186/1471-2199-8-118. [DOI] [PMC free article] [PubMed] [Google Scholar]