

Abstract
BACKGROUND:
Stomach cancer is one of the most common malignancies worldwide. In Iran, the mortality of stomach cancer is the first cause of death due to cancer in both sexes. This study was designed to estimate survival rate of stomach cancer at national level.
METHODS:
From the national cancer registry file, 3439 cases of stomach cancer that had telephone number and were diagnosed between years 2001 and 2005 were called to obtain information about their life status. Survival estimates were calculated using the Kaplan-Meier method, and the survival probability was calculated for the overall cohorts and also for gender and anatomical sites of tumor. Relative ratios (RR) according to demographic and risk variables were calculated by Cox's proportional hazard model.
RESULTS:
The overall 5-year survival rate was 12.8%. The likelihood of death was higher in men (RR = 1.21; 95% CI: 1.11-1.33) and patients more than 70 years old had worse prognosis rather than those below fifty years old (RR = 1.67; 95% CI: 1.46-1.91). The 5-year survival rate for tumors located in antrum was significantly higher than corpus and cardia (p = 0.009). Patients with lymphoma had a significantly higher 5-year survival rate compared to those with adenocarcinoma (RR = 0.46; 95% CI: 0.31-0.66).
CONCLUSIONS:
The status of stomach cancer, including relative low survival rate in Iran, indicates the extremely urgent needs for health authorities to adopt measures of cancer prevention that proved effective in other countries.
Keywords: Gastric Cancer, Survival Rate, Histopathologic Type, Anatomical Site, Iran
Cancer of the stomach is amongst the common malignancies worldwide, with some 870,000 new cases every year.1 Patients are often diagnosed with advanced disease and five-year survival rates are poor, usually less than 30%.1 Approximately 60% of all cases occur in developing countries with the highest rate in eastern Asia.1 In Iran, the incidence is around 7300 cases per year, which is the most common cancer in men.2–8 Mortality from stomach cancer is also the first cause of death due to cancer in both sexes in Iran.8,9 During 2000-2005, incidence rate was highest in Northern provinces: Guilan, Mazandaran and Ardabil.10 A few studies have already investigated the survival pattern of stomach cancer in different regions of Iran 11–14 with limited cases but are not representative to stomach cancer status in Iran. The aim of this study was to estimate survival rate of stomach cancer regarding to histopathologic type and anatomical site in 3439 patients with stomach cancer diagnosed between years 2001 and 2005 across the country.
Methods
The data from national cancer registry department in Ministry of Health and Medical Education (MOH&ME) was used as the main source of incident for stomach cancer in Iran from 2001 to 2005 which was based on pathology reports (lab based registry). The data in the maximum capability consists 81% of incident cases, and in the first year of registration less than 40%.2–8
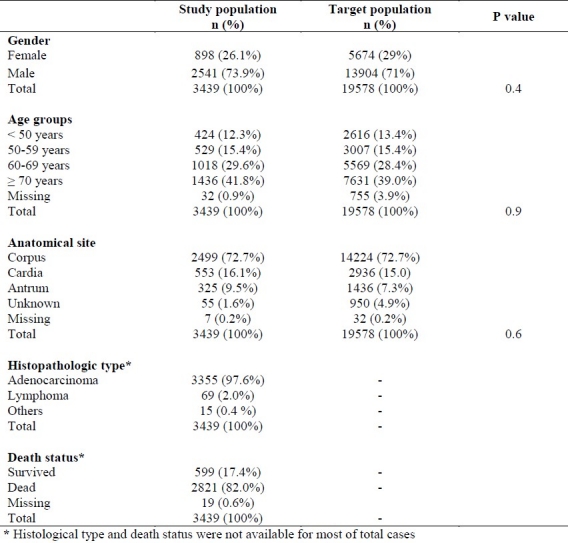
Totally 19578 cases were identified as stomach cancer between years 2001 to 2005. Telephone numbers were available for 8733 families (44.6%). To obtain information about patients, a trained nurse called and interviewed all patients or their families. With this method, we collected data from 3439 cases as the study population (40%). To find whether the study cases are the representative of target population, their demographic features of age group and gender and also the anatomical site were compared with those of the whole 19578 cases across the country as the target population (Table 1).
Table 1.
Comparing the basic characteristics of target population and study subjects
The demographic features were precise and complete, items such as age, sex, name and father name, address, telephone number, cancer site and its pathology report with the name and address of responsible doctor and hospital were well recorded. All registered cases with tumor in cardia, fundus, corpus (lesser curvature, greater curvature) and antrum (including prepyloric region) were considered as stomach cancer. International Classification of Disease for Oncology (ICD-O-3) was used for coding morphology and topography of tumors.
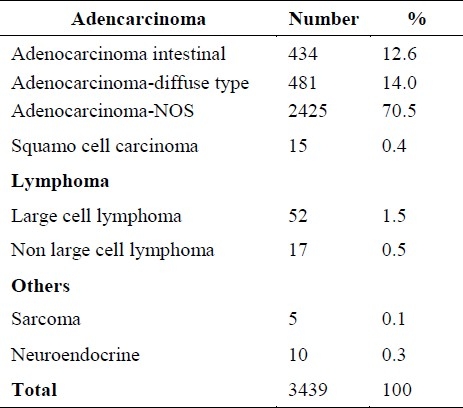
For statistical analyses, the continuous quantitative variable of age was categorized into four age groups: less than 50 year, 50-59, 60-69 and 70 or more. The anatomical sites of cancer were divided into four main categories of cardia and fundus, corpus or body, antrum or pre pyloric and unknown region. According to the number of patients in each pathologic type, the patients were categorized into three main groups: adenocarcinoma, lymphoma and others (Table 2).
Table 2.
Pathologic type categorization of 3439 study cases
The period between diagnosis and date of death or end time of the study (March 2005) has been considered as follow up time (days). By definition, survival means the time extend from diagnosis to the time of death or last visit.
Statistical Analysis
Survival rates were calculated using the Kaplan-Meier method, and the survival probability was estimated for overall cohorts and also for gender, anatomical sites and pathologic type. The significant differences in survival rates among gender and age group classifications were tested by the log rank test for trends. Relative ratios (RRs) according to demographic and risk variables were calculated by Cox's proportional hazard model, with 95% Confidence Interval (CI) up to the longest follow-up time of 2495 days. Four variables of gender, anatomical site, histopathologic type and age groups were entered in Cox's model for multivariate analysis. The log minus log plotted against survival time for each covariate did not show any deviation from the proportionality assumption. Of 3439, 250 cases had a date of death before the time of diagnosis. Thus to avoid any possible bias in results these cases were dropped. The data were analyzed with SPSS V.15.0J. All reported significance levels are from two tailed tests.
Results
The number of patients with stomach cancer recorded in data set was 3189 between years 2001 and 2005 of whom, 599 (18.8 %) cases survived during the follow-up time. Table 1 shows the baseline characteristics of the patients. Of all, 833 (26.1%) cases were women and 2273 (71.3%) cases were more than 60 years old. The mean age was 64.72 ± 12.72 years old.
The crude one-year, 2 years, 3 years, 4 years and 5 years survival rate for the whole cohorts was 47.6%, 27.2%, 19.3%, 15.7% and 12.8 % respectively. Half of the patients died after 346 days of follow-up. The median for survival time were 396 and 329 days for women and men respectively. This difference was statistically significant (p < 0.001). The difference of the median for survival time by age group was also statistically significant (p < 0.001; 494 and 281 days for less than 50 years and more than 70 years respectively). The 5-year survival rate for men and women was 11.5% and 16.4% respectively with overall survival rate of 12.8%. (Figure 1) In terms of anatomical site, the 5-year survival rate for tumors located in antrum was significantly higher than corpus and cardia (15.3%, 13.2%, 7% respectively; p = 0.009). The univariate and multivariate analysis for gender, age group, anatomical site and histopathologic types are shown in table 3. The likelihood of death was higher in men compared to women (RR = 1.21; 95% CI: 1.11-1.33). Patients in age group more than 70 years old had a worse prognosis rather than those of fifty years old (RR = 1.67; 95% CI: 1.46-1.91).
Figure 1.
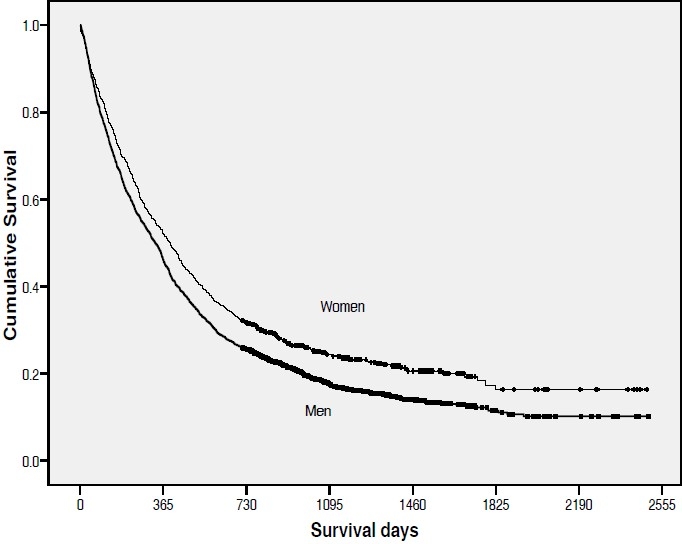
The Kaplan-Mayer overall survival curve by gender (p < 0.001)
Table 3.
Relative ratios (RR) (95+ CI) estimated from univariate and multivariate survival analysis of stomach cancer
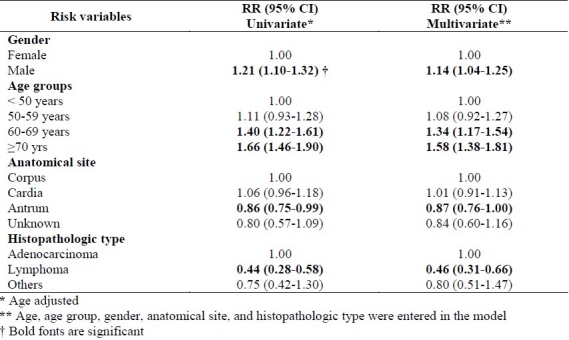
The likelihood of death was lower in patients with tumor located in antrum compared to those had tumor in corpus site (RR = 0.87; 95% CI: 0.76-1.00; p = 0.05). In terms of histopathologic type of tumor, patients with lymphoma type had a significantly higher 5-year survival rate compared to those with adenocarcinoma (RR = 0.46; 95% CI: 0.31-0.66; p < 0.001). Among patients with lymphoma type, the mean (median) survival rate of those with large cell type was 1280 (median = 427) days and for non-large cell type was 1195 (median = 1836) days. Of whole cases, 2% had lymphoma (Table 2). Only five and ten cases were diagnosed histopathologically as sarcoma and neuroendocrine tumors and the mean survival time for them was 545 (median = 501) and 674 (median = 598) days, respectively. The number of cases diagnosed histopathologically as signet cell ring, mucinous adenocarcioma and papillary adenocarcinoma was 360, 142 and 15 cases respectively. The mean (median) survival time for them was 696 (median = 324), 640 (median = 334) and 514 (median = 349) days, respectively.
Discussion
Gastric cancer is one of the most common malignancies in Iran and its incidence is particularly high in the northwest of the country.8,10,12,15,16 Patterns of gastric cancer in our country are similar to those reported from high-risk regions worldwide.17 In this national level study, the male to female ratio was 2.8:1 and the peak incidence was in the age group more than 60 years old, followed by the age group 50-59 years old. Approximately 12% of patients were younger than 50 years old. Among study groups adenocarcinoma was the commonest histological type. This is similar to western countries. Over the past decades, there has been a dramatic decrease in gastric cancer incidence in western countries18 which has been mostly in “intestinal type” rather than “diffuse type” and is comparable to present results. (Table 2) Intestinal type is more related to preventable environmental factors rather than diffuse type.
Lymphoma was seen in 2% of whole cancers in this study and in 3% in developed countries. Sarcoma in the western countries accounts for 1.5-1.7% but in present study it was less than 10%.
The most frequent primary site of tumor in present study cases was corpus followed by cardia and then pre-pyloric (Antrum) area with better survival rate and some manageable predicting factors. A shift in distribution of anatomical site of tumor within the stomach is a considerable issue in the epidemiology of gastric cancer. In the first quarter of 20th century two third of gastric cancers were located in the antrum and prepyloric area and only 10% arose in the cardia or the esophagogastric junction. Since 1970s, however, adenocarcinoma of the proximal stomach has become increasingly common worldwide; such anatomical trend has been followed by Iranian patients. Over 36 years, the prevalence of cancers in the upper and middle third of the stomach has increased and that of the lower third has decreased. These changes were seen in both genders and age groups under and over 50 years old and it was more significant in younger people.19
Understanding survival rate of the disease is important for health care planning and may also suggest opportunities for research in cancer prevention. Although gastric cancer is the most common cancer among men in China, Japan and many other Asian countries, the mortality rate is lower in these countries and in Europe rather than Iran.20 The findings of present study showed that the median survival time of all patients was 346 days. Overall survival rate for both sexes was 12.8% in this study which is approximately half of the rate of western countries (23%). The survival rate was relatively low particularly among men and age group of 70 + years. Other few survival studies showed the same results. A study on 413 patients were registered with gastric cancer referred to the Medical Oncology Department of the Cancer Institute from 1998 to 2003 found that the median survival time of all patients (with or without treatment) was 10 months overall.14
Only 3189 of 19578 (16.3% response rate) were accessible to follow their survival status which make it difficult to generalize easily the results of study to target population. However, there was no statistically significant difference between study population and target group, so the subjects might be considered as a representative of the whole target population of patients with stomach cancer across the country. (Table 1) On the other hand data were obtained from cancer office in Ministry of Health which is pathologic-based. The coverage rate of cancer in this office varies between 40 and 80 percents. Thus there is some possibility of existence of selection bias for this study, but due to sample size it will not affect the results.
In terms of histopathologic types of gastric cancer, since they have been reported by various pathologists across the country, inter-observation variation is another possible limitation for this study which might affect the results.
Conclusions
In conclusion, this study highlights the relatively low survival rate of gastric cancer and changing in anatomical site pattern for Iranian patients at national level. The status of stomach cancer in Iran indicates the extremely urgent needs for health authorities to adopt measures of cancer prevention that proved effective in other countries.
Authors’ Contributions
MEA is the coordinator of project. AA, JKh and AM have supported the project scientifically and technically. MM and ANM have analyzed the data. FF has gathered the data and prepared the data set. All writers have contributed in writing the manuscript. All authors have read and approved the content of manuscript.
Acknowledgments
Authors would like to thank the cancer office staff of Centre for Diseases Control in Ministry of Health and Medical Education for their help in providing the data for this study.
Footnotes
Conflict of Interests:
Authors have no conflict of interests.
References
- 1.Stewart BW, Kleihues P. Lyon: IARC Press-WHO; 2003. World cancer report; pp. 198–202. [Google Scholar]
- 2.Tehran Iran: Cancer Office, Center for Disease Control, Deputy for Health, Ministry of Health and Medical Education; 2002. Iranian Annual of Cancer Registration 2001-2002. (Persian) [Google Scholar]
- 3.Tehran, Iran: Cancer Office, Center for Disease Control, Deputy for Health, Ministry of Health and Medical Education; 2003. Iranian Annual of Cancer Registration 2002-2003. (Persian) [Google Scholar]
- 4.Tehran, Iran: Cancer Office, Center for Disease Control, Deputy for Health, Ministry of Health and Medical Education; 2004. Iranian Annual of Cancer Registration 2003-2004. (Persian) [Google Scholar]
- 5.Tehran, Iran: Cancer Office, Center for Disease Control, Deputy for Health, Ministry of Health and Medical Education; 2005. Iranian Annual of Cancer Registration 2004-2005. (Persian) [Google Scholar]
- 6.Tehran, Iran: Cancer Office, Center for Disease Control, Deputy for Health, Ministry of Health and Medical Education; 2006. Iranian Annual of Cancer Registration 2005-2006. (Persian) [Google Scholar]
- 7.Iranian Annual of Cancer Registration 2006-2007. Tehran, Iran: Cancer Office, Center for Disease Control, Deputy for Health, Ministry of Health and Medical Education; 2008. (Persian) [Google Scholar]
- 8.Akbari ME, Abachizadeh K, Tabatabaei SM, Ghanbari Motlagh A, Majd Jabari Z, Khaiamzadeh M, et al. Cancer in Iran. 1st ed. Qom: Darolfekr Publications; 2008. Available at: http://www.crc.ir/cancer_book.htm#id. (Persian) [Google Scholar]
- 9.Naghavi M. Iranian annual of national death registration report. Tehran: Ministry of Health and Medical Education; 2005. (Persian) [Google Scholar]
- 10.Mosavi M, Ramezani H. National report on registered cancer cases in 2005. Tehran, Iran: Cancer Office, Centre for Disease Control, Deputy for Health, Ministry of Health and Medical Education; 2005. (Persian) [Google Scholar]
- 11.Hajiani E, Sarmast Shooshtari MH, Masjedizadeh R, Hashemi J, Azmi M, Rajabi T. Clinical profile of gastric cancer in Khuzestan, southwest of Iran. World J Gastroenterol. 2006;12(30):4832–5. doi: 10.3748/wjg.v12.i30.4832. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Samadi F, Babaei M, Yazdanbod A, Fallah M, Nouraie M, Nasrollahzadeh D, et al. Survival rate of gastric and esophageal cancers in Ardabil province, North-West of Iran. Arch Iranian Med. 2007;10(1):32–7. [PubMed] [Google Scholar]
- 13.Zeraati H, Mahmoudi M, Kazemnejad A, Mohammed K. Postoperative life expectancy in gastric cancer patients and its associated factors. Saudi Med J. 2005;26(8):1203–7. [PubMed] [Google Scholar]
- 14.Sadighi S, Raafat J, Mohagheghi M, Meemary F. Gastric carcinoma: 5 year experience of a single institute. Asian Pac J Cancer Prev. 2005;6(2):195–6. [PubMed] [Google Scholar]
- 15.Sadjadi A, Malekzadeh R, Derakhshan MH, Sepehr A, Nouraie M, Sotoudeh M, et al. Cancer occurrence in Ardabil: results of a population-based cancer registry from Iran. Int J Cancer. 2003;107(1):113–8. doi: 10.1002/ijc.11359. [DOI] [PubMed] [Google Scholar]
- 16.Mohebbi M, Mahmoodi M, Wolfe R, Nourijelyani K, Mohammad K, Zeraati H, et al. Geographical spread of gastrointestinal tract cancer incidence in the Caspian Sea region of Iran: spatial analysis of cancer registry data. BMC Cancer. 2008;8:137. doi: 10.1186/1471-2407-8-137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Correa P. Clinical implications of recent developments in gastric cancer pathology and epidemiology. Semin Oncol. 1985;12(1):2–10. [PubMed] [Google Scholar]
- 18.Dempsey DT. In: Schwartz's principles of surgery. 8th ed. Brunicardi F, Andersen D, Billiar T, Dunn D, Hunter J, Pollock RE, editors. New York: McGraw-Hill Professional; 2004. pp. 971–2. [Google Scholar]
- 19.Abdi-Rad A, Ghaderi-Sohi S, Nadimi-Barfroosh H, Emami S. Trend in incidence of gastric adenocarcinoma by tumor location from 1969-2004: a study in one referral center in Iran. Diagn Pathol. 2006;1:5. doi: 10.1186/1746-1596-1-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Negri E, La Vacchia C, Franceschi S, Levi F. Pattern of mortality from major cancers in Europe. Cancer Epidemiology, Biomarks and Prevention. 1994;3(7):531–6. [PubMed] [Google Scholar]