

Abstract
Cancellation tasks are popular clinical and scientific tools for identifying spatial neglect, with neglect patients tending to miss targets on the contralesional side of the test. However, methods for analysis are not well established. Indeed, these tests are often used as a binary classifier to simply identify the presence or absence of spatial neglect, even though it is clear that there is a spectrum of disability on these tasks. We suggest that the Center of Cancellation (CoC) provides an intuitive, continuous and robust measure of neglect severity. First employed by Binder and colleagues [Arch Neurol. 1992; 49: 1187–1194], its use has not been replicated since. Our aim was to ease deployment of this measure through validation, development of software and focused exposition. To validate this index, we evaluated a group of 110 individuals with right hemisphere injury. For two different cancellation tasks (the Bells Test and the Letter Cancellation Task) we predicted spatial neglect (as defined by independent measures) using the new CoC index. Examining each individual’s performance on a single cancellation task, we were able to correctly determine with better than 98% accuracy whether three tests with binary classifiers would define them as having spatial neglect. Specifically, an acute CoC score greater than 0.081 on the Bells Test or 0.083 on the Letter Cancellation Task turned out to indicate neglect behavior after a right hemisphere brain lesion. Finally, we provide free software allowing other groups not only to rapidly analyze new but also previously existing (paper-and-pencil based) datasets using this measure.
Introduction
Since being introduced by Denny-Brown (1963) and popularized by Albert (1973), cancellation tasks have become one of the most widespread methods for diagnosing spatial neglect. Classically, the individual is shown a piece of paper with a cluttered array of items, and asked to mark all of the target items, while ignoring other distractors. The prevalence of these tests stems from many factors including the ease of describing the task to participants in a clinical situation and speed of administration (a couple of minutes). In addition, cancellation tests appear to be strong predictors of other clinical manifestations of neglect such as errors on copying or drawing tasks and biased spontaneous exploratory behavior (Ferber and Karnath, 2001).
Despite widespread usage, the interpretation of these tests has remained somewhat arbitrary. Often, these tests are used as a simple binary classifier to detect the presence or absence of neglect. However, behavioral performance of neglect patients as well as visual inspection of cancellation tests suggests that this disorder exhibits a continuous spectrum of severity desiring quantification.
One simple method that has been used to derive a continuous measure from the cancellation task is to count the number of target omissions (or hits) and use this value as a measure of neglect severity. An illustration of this approach is the Behavioral Inattention Test (BIT, Wilson et al., 1987). Unfortunately, the standardized scoring system of the BIT does not reflect lateralized bias. As a result, this analysis cannot distinguish between spatially biased performance versus inattentive performance. For example, some patients may miss items specifically on the contralesional side of the test sheet whereas others may miss the same number of targets but evenly distributed across the sheet. While the first observation is indicative of spatial neglect; the latter does not support this diagnosis because it does not exhibit the spatial bias that is so unique to spatial neglect. Therefore, the simple number of omissions (or hits) alone is not an unambiguous measure of the disorder. Differential diagnosis on this measure still requires an experienced observer evaluating the pattern of omissions produced in addition.
To deal with this problem, Halligan and colleagues (1991) proposed a continuous measure that should reflect the spatial bias observed in spatial neglect. They suggested using Friedman’s (1992) lateralization index to measure spatial biases in cancellation tasks (see van Kessel et al., 2009 for a similar measure). This ratio reflects the number of targets detected on the left half of the test divided by the total number of targets detected (so the score ranges from zero to one with values near 0.5 suggesting unbiased performance). However, this measure may not be a particularly reliable measure of severe neglect. For example, consider two patients, one who misses all items on the left half of the page, versus another more severe patient who misses items on the left three-quarters of the test. Both patients receive a score of 0 even though one appears to have a more severe deficit. Further, this index can even misclassify the relative severity of patients. For example, consider two patients, one who misses all but one items on the left half of the page, versus another more severe patient who misses all but one items on the left half of the page as well as most of the leftmost items on the right side of the page. In this case, the more severe patient will get a less severe laterality index. Moreover, it should be noted that Halligan et al. (1991) actually described the laterality index as a binary classifier for neglect, and a continuous classifier for milder biased inattention. According to their method, for a patient to be considered to have spatial neglect they must have a laterality index of zero, missing all of the items on the left side of the page. Therefore, the laterality index does not actually attempt to gauge the severity of neglect.
Chatterjee and colleagues have suggested using power functions (1992) and later logistic regression (1999) to provide parametric analyses of cancellation tasks. In this context, the logistic regression attempts to model the probability of detecting targets across a continuous variable (such as horizontal position of each target) using a sigmoid function. This sigmoid curve is described by three parameters, one that determines the steepness of slope (how quickly performance improves) a constant and finally a goodness-of-fit. The utility of this approach is that one can model multiple interacting factors, for example the influence of both near-far as well as left-right position of a target. However, the output of the logistic regression cannot be easily quantified as a single intuitive measure that can be used as an index of neglect severity and used in subsequent analyses such as lesion-behavior mapping (Rorden et al., 2007). In theory, for a single variable (horizontal position of targets), one can determine the 50% crossing point (e.g. the horizontal location where the participant detects half of all targets.) However, the range of this value can be unintuitive (this hypothetical location could be outside the bounds of the paper test) and this value will not be meaningful in individuals where the model is not accurately fitting the data (e.g. patients without neglect or with non-spatial attentional deficits leading to errors evenly distributed across space). Therefore, while this method is useful for sophisticated analyses, it is not suitable for most studies as well as daily clinical usage.
Mark and Monson (1997) suggested measuring the ‘neglect center’ – that is, the center of mass for the neglected items. Specifically, this allowed them to calculate both the angle and distance from the center of the display to the center of the neglected items. The intention of this measure was to examine changes in the direction of neglect, and the authors noted that this measure is not a direct measure of neglect severity. For example, consider a patient who misses three targets directly to the left of the display center at −6, −4, and −2cm.. This patient receives an identical neglect center score as a less severe patient or even a healthy subject who only misses a single target located at −4cm. This feature limits the utility of this measure.
In a paper focused on the anatomy of neglect, Binder and colleagues (1992) described a clever method for measuring the severity of neglect. Specifically, they measured the mean horizontal location of the cancelled items. At first glance, this ‘center of cancellation’ (CoC) appears to offer the same information as Mark and Monson’s ‘center of neglect’ measure. However, the CoC provides a direct measure of neglect severity, and it would be able to distinguish between the two patients described in the previous paragraph. In the case of the (healthy) individual who simply forgot to mark a single target, the ‘center of neglect’ will be pulled all the way to this location, which might be on the extreme edge of the test. In contrast, the CoC for this individual is heavily weighted by the (large) number of correct marks, and therefore will not be substantially different from the center of the display.
Curiously, Binder et al.’s attractive measure for cancellation tasks has not been widely adopted. We speculate that four factors may have contributed to this. First, the paper by Binder and colleagues was focused on the anatomical differences between individuals with biased performance on the line bisection task relative to cancellation tasks, with no discussion regarding the novel method for measuring cancellation. Second, computing the CoC score by hand as they did is time consuming and the authors provided no means for replicating their results. Third, they did not provide any normative data for interpreting this measure. Finally, even though the CoC is a continuous measure, Binder and colleagues used it as a binary classifier to merely identify the presence or absence of neglect.
Our aim is to further develop this measure and directly address these factors. We developed an easy to use piece of software, which allows the scientist or clinician to intuitively enter data from (paper-and-pencil based) cancellation tasks in less than one minute. This program calculates a calibrated center of cancellation statistic that is easy to interpret. With this measure, healthy individuals as well as individuals who omit items with an unbiased spatial distribution (identifying as many objects on both sides of the test) score near zero, while scores approaching positive or negative one indicate left- or right-sided neglect, respectively. This continuous score is sensitive to both the number of omissions as well as the location of these omissions. Therefore, this score will not generate some of the paradoxical results seen from other measures such as the laterality index. In our previous thought example, consider two hypothetical patients who each only find one item on the left half of the page: the less severe patient sees all items on the right half of the page and has a score near 0.5 (mean for targets on the right half), whereas the more severe patient who misses all other targets on the left ¾ of the page will receive a score near 0.75 (mean for targets on the right ¼). Figure 1 shows performance for a patient who scores near 0.5 on this measure. The range of the CoC index is easy to interpret and is similar to popular measures such as correlation ratios.
Figure 1.
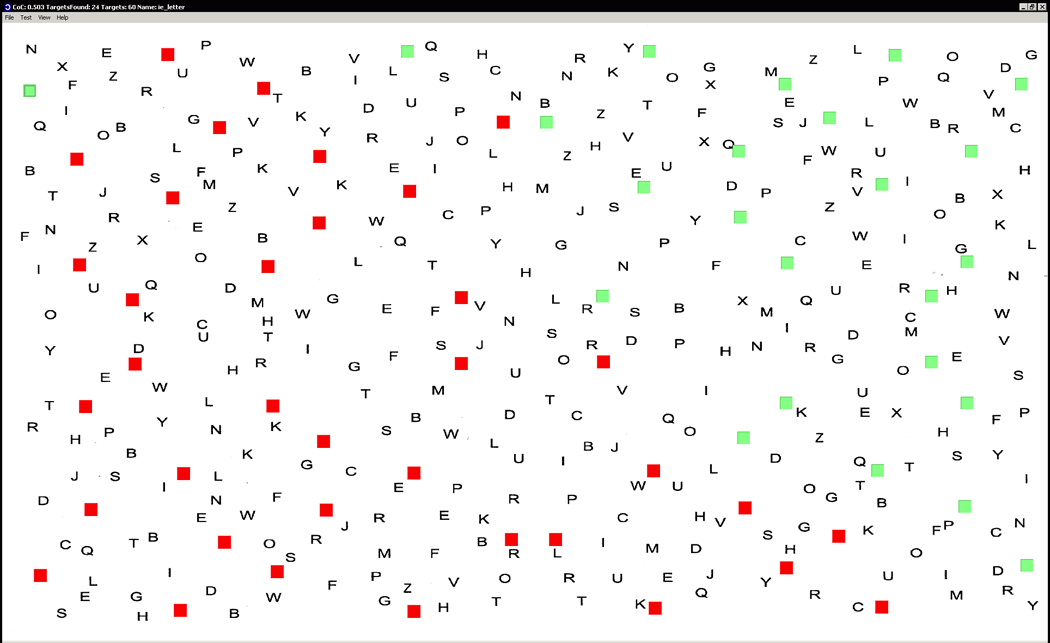
A screenshot of our software. The basis of the analysis is a participant's performance obtained from a traditional paper-and-pencil test presented on a regular sheet of paper (e.g., at the bedside). After the participant completed the paper-and-pencil test, the evaluator enters the patient's performance into the computer by toggling checkboxes to green (detected) or red (missed) targets on top of a digital illustration of the respective test sheet (here the Letter Cancellation Task; Weintraub and Mesulam, 1985). In the figure, the target letters "A" are obscured behind the checkboxes. The data can be saved electronically. Descriptive statistics such as the center of cancellation (CoC) are reported in the title bar, and can be batch-converted to a spreadsheet.
While our software can be trained on any cancellation task, we present normative data on two popular cancellation tasks: the Bells Test (Gauthier et al., 1989) and the Letter Cancellation Task (Weintraub and Mesulam, 1985).
Methods
We re-evaluated data from 110 stroke patients with focal right-hemisphere brain lesions admitted to the Center of Neurology at Tübingen Univesity, Germany (Table 1). The lesions were demonstrated by magnetic resonance imaging (MRI) or by computed tomography (CT). Patients with diffuse or bilateral brain injury, patients with tumors, as well as patients in whom MRI or CT scans revealed no obvious lesion were excluded.
Table 1.
Descriptive details for the 110 individuals with right hemisphere damage included in this study.
| Neglect | No Neglect | |||
|---|---|---|---|---|
| Number | 57 | 53 | ||
| Sex | 31 f, 26 m | 18 f, 35 m | ||
| Age (Years) | Mean (SD) | 62.7 (13.1) | 61.7 (13.8) | |
| Etiology | Infarct | 47 | 42 | |
| Haemorrhage | 10 | 11 | ||
| Time since lesion (d) | Mean (SD) | 16.7 (19) | 8.4 (11.9) | |
| Visual field defect | % present | 23 | 26 | |
| Contralateral paresis | % present | 89 | 57 | |
| Neglect | % present | 100 | 0 | |
| Letter cancellation | left | Mean (SD) | 4.4 (6.7) | 28.7 (1.7) |
| right | Mean (SD) | 18 (8.7) | 29.2 (1.2) | |
| Bells test | left | Mean (SD) | 2 (3.6) | 13.9 (1.5) |
| right | Mean (SD) | 8.8 (2.1) | 14.2 (1.5) | |
| Copying (% correct) | Mean (SD) | 47 (27) | 96 (10) |
We examined the performance of patients on three traditional paper-and-pencil tests: two cancellation tasks and a copying task, each presented on a horizontally oriented 21 × 29.7 cm sheet of paper. The Letter Cancellation Task (Weintraub and Mesulam, 1985) requires marking 60 target letters 'A' distributed amid distractors letters. The Bells Test (Gauthier et al., 1989) requires identifying 35 bell symbols distributed on a field of other symbols. Further, patients were asked to copy a complex multi-object scene consisting of four figures (a fence, a car, a house and a tree) (Copying task; Johannsen & Karnath, 2004).
In order to validate the CoC index, we used an independent clinical diagnosis of spatial neglect. This allowed us to determine if CoC scores reliably discriminate patients with neglect from those without neglect. Therefore, for the Bells Test we identified an individual as having spatial neglect if they showed biased performance on the Letter Cancellation Task or the Copying task, whereas for the Letter Cancellation Task this diagnosis was based on the performance on the Bells Test or the Copying task (for the 107 individuals where results for this test was available). We used previously established thresholds for the diagnosis of spatial neglect. The disorder was diagnosed when patients omitted more than four contralateral located targets in the Letter Cancellation Task, more than five contralateral targets in the Bells Test, or when they showed a score higher than 1 (i.e. > 12.5% omissions) in the copying task. The basis for these criteria are as follows. Weintraub and Mesulam (1985) found that four targets on each side may go undetected in normal subjects over the age of 80 in their Letter Cancellation Task. A comparable criterion was reported by Gauthier et al. (1989) for their Bells Test. They found that more than five omitted bells indicate visual neglect. For the Copying task we followed the criterion reported by Johannsen and Karnath (2004).
To analyze the severity of spatial neglect as a continuous variable, we developed a simple computer program for coding responses and measuring the CoC index (www.mricro.com/cancel/). With this program, the test image is displayed with a checkbox at each target position (Fig. 1). The investigator denotes how the participant performed by clicking the checkboxes, toggling the targets, e.g., green (if detected by the patient) or red (if missed by the patient). Subsequently, the program calculates the mean horizontal coordinate for the detected items. This center of mass is internally calculated in terms of pixels in the test image. However, this value is not intuitive and would vary between tests and with the resolution of the test image (e.g. an image that was 2048 pixels wide would provide different scores than the same image scaled to be 1024 pixels wide). Therefore, we translated and scaled this test score to provide a normalized value. Specifically, we scaled the horizontal range so that the distance between the leftmost and rightmost item is two and then translated the values so the mean horizontal position of all possible targets is zero. For perfectly symmetrical tests, this normalization ensures that an individual who only detects the leftmost target will get a score of minus one, an individual who only detects the rightmost item will receive a score of one, and individuals who miss no items or have a symmetrical pattern of errors will receive a score near zero. In practice, many cancellation tests are slightly asymmetrical, either by design or due to orientation errors when the test images are scanned to a computer. In these cases, the score for detecting all items will always be zero, but the maximum and minimum scores might not be precisely (but rather very close to) −1 and +1.
Our present analysis focused on the Letter Cancellation Task and the Bells Test. We computed CoC measures for the two cancellation tasks separately, as numerous factors influence performance on cancellation tasks (Sarri et al., 2009), for example the number and density of items. However, our algorithm and software can be applied to any other cancellation dataset. One simply needs to scan a single copy of the test to a computerized image (e.g., JPEG format) and then plot the location of each target by clicking the relevant location on the image. Once this test is saved, individual performance can be rapidly entered, stored and analyzed. The software calculates the CoC score and other statistics in a format that can be copied to any popular spreadsheet for further analysis. In addition, target coordinates and performance can be exported allowing regression analyses as described by Chatterjee et al. (1999).
Results
Our first analysis was designed to see if the CoC is a robust continuous measure of neglect severity. To accomplish this, we examined each individual’s CoC scores on two clinical tests. Across both groups, an individual’s CoC for the Letter Cancellation Task was significantly correlated with his/her CoC for the Bells Test, R = 0.9387, p < 0.0001 (t = 28.31, DF = 108), as shown in Figure 2A. The slope of this correlation was 0.8661. While this result demonstrates that CoC performance on one cancellation task is predictive of CoC on a different cancellation task, we also wanted to see how the CoC correlated with a conceptually different task. We found that performance on the copying task was predictive of CoC scores for both the Bells Test (R = 0.809, p < 0.0001, t = 14.1, DF = 105) and the Letter Cancellation Task (R = 0.8305, p < 0.0001, t = 15.28, DF = 105). We also computed the Receiver Operating Characteristics (ROC) value known as the ‘Area Under the Curve’ (AUC) using a formula described by Obuchowski (2006), and found that both the Letter and Bells CoC values were moderate accuracy predictors of each other (0.825458288192749). Note that this non-parametric measure is based on ranking of data and may be somewhat influenced by the noise of the large number of samples with values near zero on both measures.
Figure 2.

Center of cancellation (CoC) scores provide reliable and accurate measure for neglect severity. Left panel (A) compares each individual’s CoC score for the Bells Test and the Letter Cancellation Task. This suggests that the continuous CoC index of neglect severity has re-test reliability between tasks. Right panel (B) shows mean CoC scores for individuals who have been rated with the absence (control) or presence (neglect) of spatial neglect for both the Bells Test and the Letter Cancellation Task. Error bars show standard deviation. This suggests that the CoC score is an accurate predictor for conventional binary classifiers of neglect.
Our second analysis compares the CoC measure against two independent traditional clinical binary classifiers for spatial neglect. The acute right-sided stroke patients without spatial neglect had a mean CoC score of 0.0098, with a standard deviation of 0.0306 for the Bells Test, and a mean of 0.0105 with a standard deviation of 0.0313 for the Letter Cancellation Task. To assess the sensitivity of the CoC index, we examined the CoC scores for the remaining 57 patients who were classified as having neglect. Specifically, we used 2.326 standard deviations to create cutoff thresholds of 0.0809 and 0.0833 respectively – this value corresponds to p < 0.01 for a one-tailed test. To validate the sensitivity of this measure, we applied this threshold to the remaining patients who were classified as having neglect based on independent measures. The CoC threshold was able to correctly detect all 57 of the individuals with neglect based solely on their performance on either one of the two cancellation tasks (with mean CoC scores of 0.632 [SD = 0.278] for the Bells Test and 0.583 [SD = 0.258] for the Letter Cancellation Task). On the other hand, when this threshold was applied to the 53 patients without neglect (the population used to define our threshold), a total of three individuals were classified as having neglect (two based on the performance in the Bells test and one based on performance on the Letter Cancellation task). Therefore, of the 110 individuals, our binary CoC cutoff based on the performance from a single cancellation test (Letter Cancellation Task or Bells Test) agreed with the independent traditional scoring method applied to three tests in 98.6% of the cases. Mean and standard deviation values for the CoC index of both patient groups are shown in Figure 2B. We also computed the Receiver Operating Characteristics (ROC) value known as the ‘Area Under the Curve’ (AUC) using a formula described by Obuchowski (2006), and found that both the Letter and Bells CoC values were high accuracy predictors of neglect as defined on the other tests (with Letter CoC having a AUC of 0.998427673 for predicting neglect detected by either the Bells or Copy task, where the Bells CoC had a ‘perfect’ AUC of 1.0 for neglect as detected by either the letter or copy task).
Discussion
We examined the CoC for both the Bells Test and the Letter Cancellation Task in a large group of 110 individuals who had acute right hemisphere stroke. We used independent binary classifiers from two clinical tests to generate normative data for the CoC scores. These values proved accurate at detecting the neglect patients in our sample of acute stroke patients. Crucially, our data suggests that this measure is a robust continuous measure of neglect severity; we wish to emphasize the strong correlation of CoC scores observed on two independent cancellation tasks (see Figure 2B).
Our aim was to provide a simple, rapid, and intuitive index for measuring the severity of spatial neglect using cancellation tasks. One could argue that an alternative route for this aim would be to use other tests such as line bisection, copying, clock drawing or computerized tasks measuring reaction times. Below we briefly describe the strengths and weaknesses of each of these alternatives. However, we wish emphasize that we do not feel that cancellation tasks should be seen as competing against these other tasks; rather, that these tests complement each other. Our objective is to simply enhance the utility of the prevalent cancellation tasks, rather than discourage the use of other tasks.
The line bisection task is an easy to administer paper-and-pencil task that provides a continuous measure for spatial biases, depending on the respective line length. In this task, the participant is asked to determine the midpoint of horizontal lines. With long line lengths, many individuals with right hemisphere injury incorrectly identify a location to the right of the true midpoint. This continuous measure is sensitive to the severity of deficit. However, there is evidence that the line bisection taps different cognitive skills than the cancellation task (Ferber and Karnath, 2001; though see Azouvi et al., 2002) and that different brain regions subserve performance on these two tests. Specifically, Binder et al. (1992) and Rorden et al. (2006) found that neglect patients who exhibited line bisection deficits exhibited more posterior injury than neglect patients who showed biased performance on the cancellation task. Therefore, while the line bisection task provides an intriguing insight into spatial perception, it is clearly dissociable from other components of neglect.
There are other popular paper-and-pencil tasks that are sensitive to spatial neglect, such as the copying task and clock-drawing task (e.g. Friedman, 1991; Johannsen and Karnath, 2004). However, performance on these tasks tends to have many of the same issues as traditional measures for the cancellation tasks. For example, evenly distributed omissions of elements and missing elements on only one side of the drawings result in the same omission score.
The Behavioral Inattention Test (BIT) includes a combination of different tasks including cancellation, bisection, copying, and card sorting. As previously mentioned, standard scoring for this test does not dissociate between spatial and non-spatial attentional deficits. Therefore, this battery can be enhanced using measures of spatial bias such as the CoC index we propose. On the other hand, by using multiple tests, the BIT is able to detect a broad range of attentional deficits. One consequence of this breadth, however, is that the BIT requires approximately forty minutes to administer which often precludes conducting the full test, in particular in the acute period of a stroke.
Beyond paper-and-pencil based procedures, measuring response times to the occurrence of spatially distributed targets can detect subtle attentional biases. Several groups (e.g. Zimmermann & Fimm, 2002; Deouell et al. 2005; van Kessel et al., 2009) have developed visual tasks where participants watch a computer screen and press a button when a target item appears in a cluttered array. However, these tasks tend to be more time consuming (e.g., the procedure described by Deouell et al. requires the better part of an hour) and therefore are not always easy to apply in acute clinical settings. Moreover, the application of these procedures requires a computer and response button to be brought to the bedside, which also is not always convenient, particularly in the acute period of the stroke.
We wish to stress that the present work and thresholds were based on the pen-and-paper performance of acute patients, and it is reasonable to assume that computerized tasks may be more appropriate for examining chronic deficits. Support for this notion comes from recent work by Rengachary et al. (2009) who found that reaction time tests administered at the chronic stage were more sensitive than paper-and-pencil tasks for discriminating between patients who were diagnosed as having acute neglect from aged-matched neurologically-healthy controls. Hopefully, future work will conduct a similar analysis to contrast the performance of chronic stroke patients who experienced acute neglect to those who did not exhibit acute neglect, as the analysis conducted by Rengachary et al. (2009) can not distinguish between neglect-specific biases versus more general deficits observed following stroke that could lead to abnormal response times. This caveat emphasizes that the choice of a control group directly influences the inference that can be drawn from an analysis, an issue relevant to our own findings.
Note that our normative data is based on individuals who have suffered right hemisphere stroke but do not exhibit overt signs of neglect on standard binary classifiers. One of the underlying assumptions for the present work is that spatial biases represent a continuum, and therefore our control population of non-neglecting patients is likely to include individuals with subtle biases. An alternative approach would be to collect normative data from neurologically healthy aged matched controls (e.g. Lowery et al., 2004). However, stroke victims may perform differently from healthy adults, as brain injury often directly causes (non-spatial) changes in performance. This population may exhibit abnormal performance for a wide range of unspecific reasons related to their hospitalization including new medications, disrupted sleep, fatigue from regular testing, etc. Therefore, we feel that using an acute stroke patient group without neglect is the most appropriate control. In any case, accidental inclusion of sub-acute attentional bias to our control group should decrease the sensitivity of our observed results. Therefore, the observed accuracy of our classification suggests that this is not a major limitation for the CoC thresholds we report. In addition, future studies could always employ the actual continuous CoC score without an arbitrary binary cutoff. Doing so should include the variability explained by the subacute symptoms.
Our aim was to validate the CoC measure using two established measures for horizontal spatial biases. However, our software can generate additional CoC values that may prove useful. First, neurological patients may exhibit spatial biases not only in horizontal directions but also in the anterior-posterior direction. These effects are often referred to as ‘altitudinal neglect’ (Rapcsak et al., 1988) when seen in isolation or ‘diagonal neglect’ (Mark and Monson, 1997) when seen in combination with horizontal biases. To capture these effects, our software generates CoC measures for both the horizontal and anterior-posterior dimensions. In addition, some cancellation tasks include different forms of target stimuli with the aim of dissociating different patterns of neglect. For example, Ota and colleagues (2001) used tests where some targets were defined by features on their left side, while others were defined by right-sided features. They suggest that some patients show body-centered biases while others show stimulus-centered biases. Our software allows the user to define different forms of targets, computing the CoC values independently for each target type.
The strength of our proposal is that we do not require a new method for data collection. Rather, we are proposing a new tool for analysis for widely distributed and well-established clinical paper-and-pencil tests. Therefore, the CoC index can be applied to decades worth of data, and does not require any modification of ongoing data collection. The computer program that were are providing can calculate the 'center of cancellation' measure not only for the Bells Test and the Letter Cancellation Task but for any other cancellation test.
Acknowledgements
This work was supported by the National Institutes of Health (R01 NS054266) and the Bundesministerium für Bildung und Forschung (BMBF-Verbund 01GW0641 "Räumliche Orientierung") and the Deutsche Forschungsgemeinschaft (KA 1258/10-1). We are grateful to Johannes Rennig and Sabrina Oelschlaeger for their help with table 1 and with entering data by using the new CoC software.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Albert ML. A simple test of visual neglect. Neurology. 1973;23:658–664. doi: 10.1212/wnl.23.6.658. [DOI] [PubMed] [Google Scholar]
- Azouvi P, Samuel C, Louis-Dreyfus A, Bernati T, Bartolomeo P, Beis JM, Chokron S, Leclercq M, Marchal F, Martin Y, De Montety G, Olivier S, Perennou D, Pradat-Diehl P, Prairial C, Rode G, Siéroff E, Wiart L, Rousseaux M. Sensitivity of clinical and behavioural tests of spatial neglect after right hemisphere stroke. J Neurol Neurosurg Psychiatry. 2002 Aug;73(2):160–166. doi: 10.1136/jnnp.73.2.160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Binder J, Marshall R, Lazar R, Benjamin J, Mohr JP. Distinct syndromes of hemineglect. Arch. Neurol. 1992;49:1187–1194. doi: 10.1001/archneur.1992.00530350109026. [DOI] [PubMed] [Google Scholar]
- Chatterjee A, Mennemeier M, Heilman KM. A stimulus-response relationship in unilateral neglect: the power function. Neuropsychologia. 1992;30:1101–1108. doi: 10.1016/0028-3932(92)90101-q. [DOI] [PubMed] [Google Scholar]
- Chatterjee A, Thompson KA, Ricci R. Quantitative analysis of cancellation tasks in neglect. Cortex. 1999;35:253–262. doi: 10.1016/s0010-9452(08)70798-6. [DOI] [PubMed] [Google Scholar]
- Denny-Brown D. The physiological basis of perception and speech. In: Halpern L, editor. Problems of dynamic neurology. Jerusalem: Hebrew University Medical School Publications; 1963. pp. 30–62. [Google Scholar]
- Deouell LY, Sacher Y, Soroker N. Assessment of spatial attention after brain damage with a dynamic reaction time test. J Int Neuropsychol Soc. 2005;11:697–707. doi: 10.1017/S1355617705050824. [DOI] [PubMed] [Google Scholar]
- Ferber S, Karnath HO. How to assess spatial neglect-line bisection or cancellation tasks? J Clin Exp Neuropsychol. 2001;23:599–607. doi: 10.1076/jcen.23.5.599.1243. [DOI] [PubMed] [Google Scholar]
- Friedman PJ. Clock drawing in acute stroke. Age and Ageing. 1991;20:140–145. doi: 10.1093/ageing/20.2.140. [DOI] [PubMed] [Google Scholar]
- Friedman PJ. The star cancellation test in acute stroke. Clinical Rehabilitation. 1992;6:23–30. [Google Scholar]
- Gauthier L, Dehaut F, Joanette Y. The bells test: A quantitative and qualitative test for visual neglect. International Journal of Clinical Neuropsychology. 1989;11:49–54. [Google Scholar]
- Halligan P, Robertson IH, Pizzamiglio L, Hömberg V, Weber E, Bergego C. The laterality of visual neglect after right brain damage. Neuropsychological Rehabilitation. 1991;1:281–301. [Google Scholar]
- Johannsen L, Karnath HO. How efficient is a simple copying task to diagnose spatial neglect in its chronic phase? J Clin Exp Neuropsychol. 2004;26:251–256. doi: 10.1076/jcen.26.2.251.28085. [DOI] [PubMed] [Google Scholar]
- Lowery N, Ragland JD, Gur RC, Gur RE, Moberg PJ. Normative data for the symbol cancellation test in young healthy adults. Appl Neuropsychol. 2004;11:218–221. doi: 10.1207/s15324826an1104_8. [DOI] [PubMed] [Google Scholar]
- Mark VW, Monson N. Two-dimensional cancellation neglect - A review and suggested method of analysis. Cortex. 1997;33:553–562. doi: 10.1016/s0010-9452(08)70236-3. [DOI] [PubMed] [Google Scholar]
- Obuchowski NA. An ROC-type measure of diagnostic accuracy when the gold standard is continuous-scale. Statistics in Medicine. 2006;25:481–493. doi: 10.1002/sim.2228. [DOI] [PubMed] [Google Scholar]
- Ota H, Fujii T, Suzuki K, Fukatsu R, Yamadori A. Dissociation of body-centered and stimulus- centered representations in unilateral neglect. Neurology. 2001;57:2064–2069. doi: 10.1212/wnl.57.11.2064. [DOI] [PubMed] [Google Scholar]
- Rapcsak SZ, Cimino CR, Heilman KM. Altitudinal neglect. Neurology. 1988;38:277. doi: 10.1212/wnl.38.2.277. [DOI] [PubMed] [Google Scholar]
- Rengachary J, d'Avossa G, Sapir A, Shulman GL, Corbetta M. Is the posner reaction time test more accurate than clinical tests in detecting left neglect in acute and chronic stroke? Arch Phys Med Rehabil. 2009;90:2081–2088. doi: 10.1016/j.apmr.2009.07.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rorden C, Fruhmann Berger M, Karnath HO. Disturbed line bisection is associated with posterior brain lesions. Brain Res. 2006;1080:17–25. doi: 10.1016/j.brainres.2004.10.071. [DOI] [PubMed] [Google Scholar]
- Sarri M, Greenwood R, Kalra L, Driver J. Task-related modulation of visual neglect in cancellation tasks. Neuropsychologia. 2009;47:91–103. doi: 10.1016/j.neuropsychologia.2008.08.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- van Kessel ME, van Nes IJ, Brouwer WH, Geurts AC, Fasotti L. Visuospatial asymmetry and non-spatial attention in subacute stroke patients with and without neglect. 2009 doi: 10.1016/j.cortex.2009.06.004. in press. [DOI] [PubMed] [Google Scholar]
- Weintraub S, Mesulam MM. Mental state assessment of young and elderly adults in behavioral neurology. In: Mesulam MM, editor. Principles of behavioral neurology. Philadelphia: Davis Company; 1985. pp. 71–123. [Google Scholar]
- Wilson B, Cockburn J, Halligan P. Behavioral inattention test manual. London, England: Tames Valley Test Company; 1987. [Google Scholar]
- Zimmermann P, Fimm B. A test battery for attentional performance. In: Leclercq M, Zimmermann P, editors. /Applied Neuropsychology of Attention. Theory, Diagnosis and Rehabilitation. London: Psychology Press; 2002. pp. 110–151. [Google Scholar]