

Abstract
The purpose of the study was to report a case of choroidal neovascularization (CNV) secondary to ocular toxoplasmosis in an 18-year-old female patient. She was treated with a single intravitreal injection of ranibizumab. The CNV resolved as confirmed by fluorescein angiography and optical coherence tomography (OCT). The visual acuity improved to 20/30, which was maintained till the last follow-up visit at two years, without requisition of a repeat injection.
Keywords: Choroidal neovascularization, intravitreal injection, ocular toxoplasmosis, ranibizumab, vascular endothelial growth factor
Treatment of choroidal neovascularization (CNV) secondary to ocular toxoplasmosis includes laser photocoagulation, photodyamic therapy (PDT), and intravitreal injection of the anti-vascular endothelial growth factor (VEGF) agent.[1–6] Ranibizumab in combination with anti parasitic agents has been used in the treatment of toxoplasmosis associated neovascular lesions.[7] We report a case of CNV secondary to ocular toxoplasmosis, in an 18-year-old female, which resolved with a single intravitreal injection of ranibizumab alone.
Case Report
An 18-year-old female patient was referred to us with sudden blurring of vision in the right eye. She was a known case of bilateral toxoplasmosis, and was treated elsewhere for right eye macular retinochoroiditis a year before. The clinical notes were referred to and they suggested that it was mainly a clinical diagnosis, with positive serum IgG and negative IgM titers [IgG - 3.88 OD (Optical density) ratio, IgM-0.40 OD (Optical density) ratio, ELISA]. The clinical response to a combination of oral sulfadiazine and pyrimethamine along with systemic steroids also supports the diagnosis. On examination the best corrected Snellens visual acuity was 20/80 in the right eye and 20/400 in the left eye. The anterior chamber and vitreous cavity were quiet. The intraocular pressure was 12 mm Hg (applanation), in both eyes. On fundus examination, both eyes showed macular retinochoroidal scars, which in the right eye was bordered by subretinal fluid [Fig. 1]. Fundus fluorescein angiography (FFA) and OCT confirmed the presence of CNV in the right eye [Fig. 2], which was treated with a single intravitreal ranibizumab injection (0.5 mg). The visual acuity improved to 20/30 at the four-week follow-up visit. This was maintained till the last follow-up visit at two years. FFA and OCT confirmed the resolution of CNV [Fig. 3].
Figure 1.
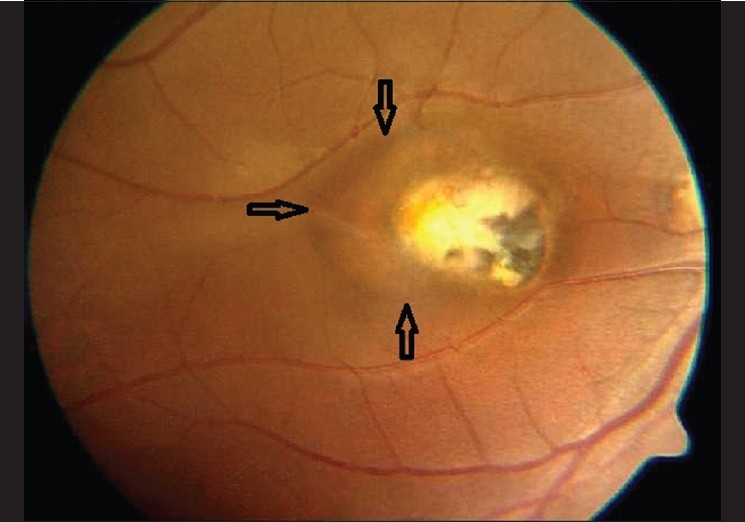
Fundus photograph of the right eye shows a macular retinochoroidal scar bordered temporally by subretinal fluid (delineated by hollow arrows)
Figure 2.
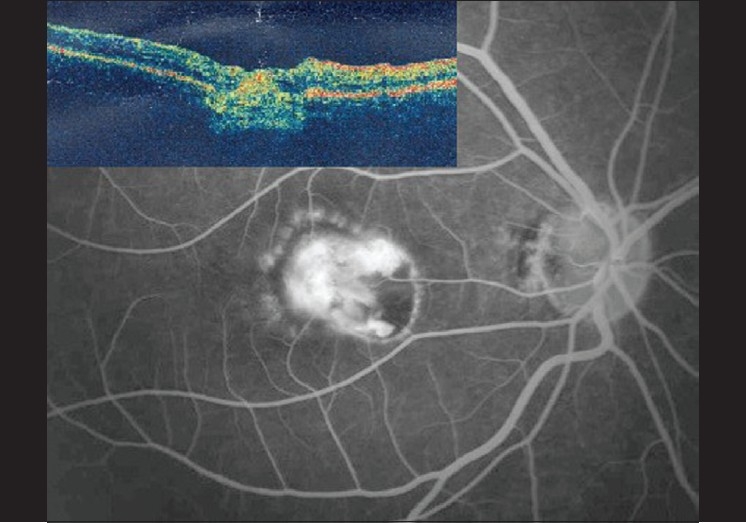
Fluorescein angiogram (late venous phase) of the right eye showing leakage from the subfoveal choroidal neovascularization. Inset shows the corresponding optical coherence tomography with an increased reflectivity of the retinal pigment epithelium-choriocapillaris complex, suggestive of a choroidal neovascular membrane
Figure 3.
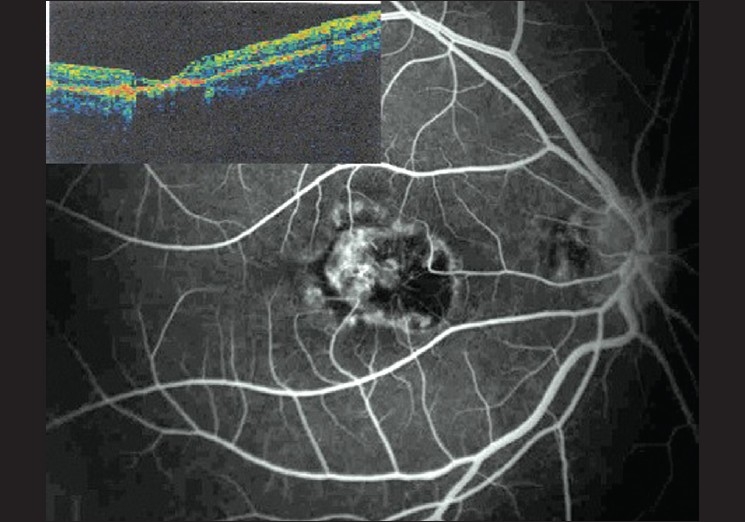
Fluorescein angiogram (venous phase -5 minutes 37 seconds) and Optical coherence tomography (inset) of the right eye showing resolution of the choroidal neovascularization
Discussion
Choroidal neovascularization is a known complication of ocular toxoplasmosis.[1–6] In the recent past, PDT has been introduced in the treatment of CNV secondary to ocular toxoplasmosis. Although, an early recovery of visual acuity has been observed with PDT, multiple treatments have been required.[5,6] VEGF has been seen to play a role in the development of inflammatory CNV.[8] The role of ranibizumab in the treatment of CNV due to age-related macular degeneration (AMD) has been well-established. Bevacizumab, an economically viable option to ranibizumab, has been reported to be effective in the treatment of CNV due to ocular toxoplasmosis.[4] Treatment with ranibizumab alone has not been reported to be used in the treatment of CNV secondary to ocular toxoplasmosis.
Based on the understanding that active infectious retinitis may be obscured by hemorrhage or it may be difficult or impossible to distinguish it from the choroidal neovascular membrane (CNVM), and because injections may reactivate chorioretinitis, the concurrent therapy with oral anti-toxoplasma medicine and ranibizumab has been prescribed.[7]
However, in our patient we did not combine anti-parasitic treatment, as there was no active vitreous reaction suggesting active retinochoroiditis. Also, there was no hemorrhage in the obscure underlying retinochoroidal lesion, which would merit treatment with anti-parasitic agents.
In our case a single intravitreal injection of ranibizumab was effective in resolving the CNV secondary to ocular toxoplasmosis, unlike the repeated injections generally needed in cases of CNV secondary to AMD. However, a long-term study is required to substantiate the role of ranibizumab and its frequency of administration in the treatment of CNV secondary to ocular toxoplasmosis.
References
- 1.Adan A, Mateo C, Wolley-Dod C. Surgery for subfoveal choroidal neovascularization in toxoplasmic retinochoroiditis. Am J Ophthalmol. 2003;135:386–7. doi: 10.1016/s0002-9394(02)01947-5. [DOI] [PubMed] [Google Scholar]
- 2.Wirthlin R, Song A, Song J, Rosenfeld PJ. Verteporfin photodynamic therapy of choroidal neovascularization secondary to ocular toxoplasmosis. Arch Ophthalmol. 2006;124:741–3. doi: 10.1001/archopht.124.5.741. [DOI] [PubMed] [Google Scholar]
- 3.Perentes Y, Van Tran T, Sickenberg M, Herbort CP. Subretinal neovascular membranes complicating uveitis: Frequency, treatments and visual outcome. Ocul Immunol Inflamm. 2005;13:219–24. doi: 10.1080/09273940490518883. [DOI] [PubMed] [Google Scholar]
- 4.Ben Yahia S, Herbort CP, Jenzeri S, Hmidi K, Attia S, Messaoud R, et al. Intravitreal bevacizumab (Avastin) as primary and rescue treatment for choroidal neovascularization secondary to ocular toxoplasmosis. Int Ophthalmol. 2008;28:311–6. doi: 10.1007/s10792-008-9218-2. [DOI] [PubMed] [Google Scholar]
- 5.Nessi F, Guex-Crosier Y, Ambresin A, Zografos L. Photodynamic therapy with verteporfin for subfoveal choroidal neovascularization secondary to toxoplasmic chorioretinal scar. Klin Monbl Augenheilkd. 2004;221:371–3. doi: 10.1055/s-2004-812860. [DOI] [PubMed] [Google Scholar]
- 6.Oliveira LB, Reis PA. Photodynamic therapy-treated choroidal neovascular membrane secondary to toxoplasmic retinochoroiditis. Graefes Arch Clin Exp Ophthalmol. 2004;242:1028–30. doi: 10.1007/s00417-004-0894-y. [DOI] [PubMed] [Google Scholar]
- 7.Benevento JD, Jager RD, Noble AG, Latkany P, Mieler WF, Sautter M, et al. Toxoplasmosis-associated neovascular lesions treated successfully with ranibizumab and antiparasitic therapy. Arch Ophthalmol. 2008;126:1152–6. doi: 10.1001/archopht.126.8.1152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kwak N, Okamoto N, Wood JM, Campochiaro PA. VEGF is major stimulator in model of choroidal neovascularization. Invest Ophthalmol Vis Sci. 2000;41:3158–64. [PubMed] [Google Scholar]