

Abstract
Background:
Subdural posttraumatic collections are called usually Traumatic Subdural Hygroma (TSH). TSH is an accumulation of cerebrospinal fluid (CSF) in the subdural space after head injury. These collections have also been called Traumatic Subdural Effusion (TSE) or External Hydrocephalous (EHP) according to liquid composition, or image features. There is no agreement about the pathogenesis of these entities, how to define them or if they are even different phenomena at all.
Case Description:
We present a case of a complex posttraumatic subdural collection, the role of cranioplasty as definite solution and review the literature related to this complication.
Conclusion:
Patients who undergo decompressive craniectomy (DC) have a risk of suffering a subdural collection of 21-50%. Few of these collections will become symptomatic and will need evacuation. When this happens, cranioplasty might be the definitive solution.
Keywords: Cranioplasty, decompressive craniectomy, subdural effusion, subdural hygroma, traumatic head injury
INTRODUCTION
The incidence rate of subdural collections after head trauma is between 7 and 12%.[17] The incidence of this complication rises to 21-50% of head injury patients if a decompressive craniectomy (DC) is performed.[25] Subdural collections are fluid accumulations with higher or lower protein content, which are normally asymptomatic, and course with spontaneous resolution. Nevertheless, they become occasionally symptomatic due to mass effect. In those cases it is important to know the characteristics of the collection, its etiology, and natural history in order to apply the right treatment. We present the case of a symptomatic subdural collection, in a patient in whom a decompressive craniectomy was performed, which was resolved by the repair of the skull defect.
CASE REPORT
A 28 year-old male was admitted to the trauma Intensive Care Unit (ICU) of ′12 de Octubre′ Hospital after having suffered a traffic accident. He had been run over by a car suffering a severe head trauma, and deteriorated to Glasgow Coma Scale (GCS) 3 and bilateral reactive mydriasis. He was transferred to the hospital hemodynamically stable, and presented a GCS of 3 and bilateral reactive mydriasis. A head Computed Tomography (CT) was performed, showing a left frontotemporal subdural hematoma 11 mm width, collapsed quadrigeminal cistern and a 3 mm midline shift[Figure 1]. A left fronto-parieto-temporal craniotomy was performed and a subdural hematoma was evacuated. Due to intraoperative brain swelling, the bone flap was not replaced. A control CT scan showed improvement of visualization of basal cisterns and resolution of the midline shift. He was treated under the Brain Trauma Foundation guidelines,[2] showing good intracranial pressure (ICP) control. His condition gradually improved, and 25 days after trauma the patient was tracheostomized, partially recovering from a right hemiparesis and presented a GCS of 11. During the following days, several CT scans were performed, showing a growing liquid collection under the skin flap[Figure 1]. The patient was scheduled for cranioplasty, but before the operation could be performed, the patient′s condition deteriorated to a GCS of 4 (M2). Dysautonomic changes in patient′s vital signs occurred, along with bilateral decerebration posture and bilateral reactive mydriasis. A new CT scan was obtained, showing a greater subdural hygroma, with a left to right midline shift of 13 mm[Figure 1]. A subdural catheter was placed percutaneously to evacuate this collection. This catheter was linked to a pressure gauge, which showed pressures between 0 and 5 mmHg at all moments. Subdural collection biochemistry analysis showed high levels of protein (1.96 g/L), without decreased glucose. Patient condition improved, and draining was stopped, but patient condition started to deteriorate again, therefore it was decided to keep it draining until cranioplasty was eventually performed. During surgery, a depressed brain parenchyma was found with neomembranes with thick vessels[Figure 2]. Those membranes were removed but brain did not recover to its normal volume. On the assumption that the patient could present another episode of deterioration, a closed subdural drainage was kept in place for 5 days[Figure 1]. It didn΄t have to be open at any time. The cranioplasty completely resolved the subdural hygroma, and the patient΄s condition improved drastically, so that he could be discharged with GCS 14 and very mild right hemiparesis. At 6 months follow up the patient had recovered and could independently carry out his basic daily activities. Control Magnetic Resonance Image (MRI) showed only subcortical white matter lesions related to diffuse axonal injury, and no recurrence of the hygroma.
Figure 1.

Evolution of Subdural Collection through sequential computed tomography scans. The collection reaches its peak volume by day 31, then, a subdural catheter is placed by day 32. By day 35, cranioplasty is performed and then the collection steadily decreases until complete resolution by day 56
Figure 2.
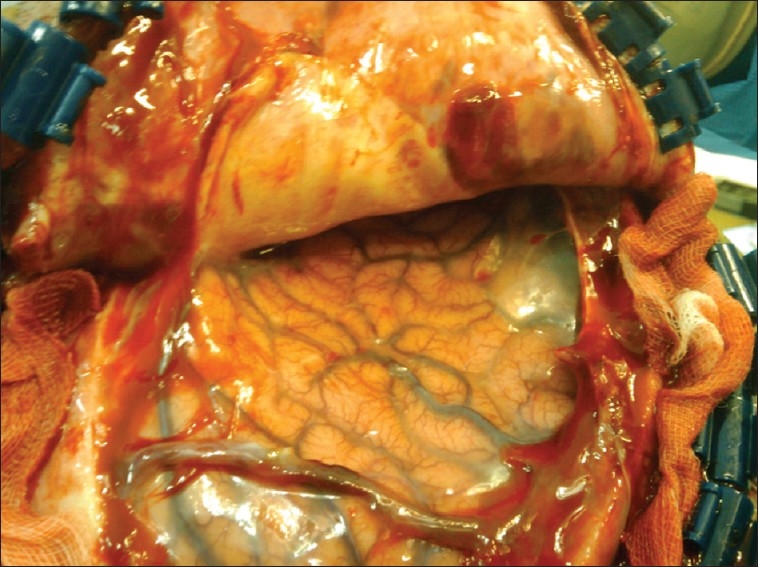
Surgical view: Brain parenchyma is depressed, and neomembranes are seeing in the operative field with thick vessels
DISCUSSION
DC is increasingly being used as a life saving procedure in head injury and brain ischemia. However, it is not a procedure without complications. The incidence of CSF circulation derangements is high after DC, as hydrocephalus and the presence of subdural collections are frequent complications after this procedure. Natural history of subdural collections has been described by Arabi et al.,[1] They appear along the first week, reach their peek volume by 4th week, and disappear around the 17th week. 92% of patients who have undergone DC harbor the TSH ipsilateral to the surgery side.[10,19,23,24,27] High dynamic accidents and diffuse traumatic brain injuries have been pointed out as risk factors for a subdural hygroma (SDG) following DC.[6–8,10,12,16,18,23,25] On the other hand, duraplasty at the time of DC has been observed to lower the incidence of TSH.[1,17,23] Most of these collections resolve spontaneously,[1,24,25] as the need for surgical evacuation of the collection is low in different series ranging from 30 to 8%. It seems more likely the collection will need to be drained if it is contralateral to DC, since it is more likely to become symptomatic.[1,17,20,23]
In those cases, burr hole drainage resolve most of them, a subduroperitoneal shunt being the choice if it is recurrent. To the best of our knowledge, the resolution of these collections after cranioplasty have been suggested,[7] but never documented before.
The etiology of these collections is not clear. Three different physiopathological mechanisms have been proposed as responsible for their production and maintenance:
A subarachnoid - dura interface tear produced either by shear stress generated by kinetic energy or by surgical injury, allowing unidirectional pass of CSF (valve effect) could create and perpetuate the collection.[1,6,12,18,23]
The presence of a vascular or parenchymal injury could originate the effusion to the subdural space.
An increased arachnoid permeability due to physical disruption or higher transmembrane pressure.
Zanini et al. proposed a new classification of TSH according to the presence of mass effect and hydrocephalus.[26,27] They divided TSH into group I without mass effect, and II with mass effect. A subdivision was made in group I into Ia without hydrocephalus, and Ib with hydrocephalus. They proposed a continuum of CSF absorption impairment as the origin of the different types of collections, the group Ia showing a disruption of subarachnoid membrane without absorption impairment, Ib with impairment, and II the most severe cases, presenting with marked mass effect. They did not correlate this classification with CSF composition.
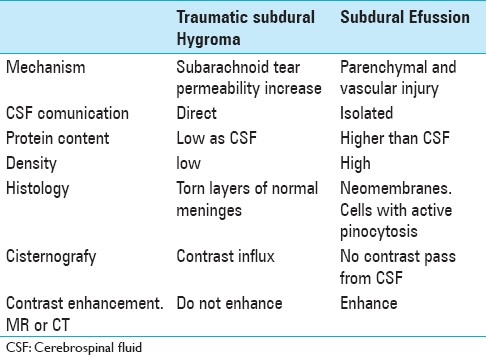
Stone et al. stated that the protein content of the subdural collection was higher than CSF,[18] and, based on that, Miranda et al. classified them into TSH if composition was similar to CSF, and Subdural effusion (SEF) if it had a higher protein content.[14] According to cisternography and gammagraphic studies,[11,18] TSH presents communication with CSF, while SEF presents tracer activity after vascular injection but not after lumbar puncture injection[Table 1]. Summarizing what have been exposed, we think Zanini classification is useful and it might have a histological and physiopathological correlation. Type Ia and Ib would be what other called TSH as a result of subarachnoid injury, either traumatic or surgically. Type Ib would be a result of a more severe injury so the CSF absorption mechanism is impaired. Type II would be even a more severe injury affecting the vessels also. These vessels would leak proteins that would induce an inflammatory reaction, which distorts the already altered permeability, perpetuating the process. This increase in protein content will raise the oncotic pressure, thus drawing water from the space with lower oncotic pressure, the CSF.
Table 1.
Traumatic Subdural Hygroma and subdural effusion differences
Waziri et al. pointed out that decompressive craniectomy flattens the normal dicrotic ICP waveform.[21] Since the arachnoid granulations are believed to function as pressure-dependent one-way valves from the subarachnoid space to the draining venous sinuses,[3] it is possible that disruption of pulsatile ICP dynamics secondary to opening the cranial vault results in decreased CSF outflow. It has been documented by Welch and Friedman from light microscopic studies that arachnoid villi opens at a CSF pressure of 2-5 cm H2O,[3,22] thus implying that the normal dicrotic ICP waveform might be necessary for CSF reabsorption. This would explain why, once the collection is formed, it is not reabsorbed[Figure 3], and how cranioplasty might play a role resolving most symptomatic effusions. We believe that is the situation in our case. The high containing protein liquid in the subdural space draws water from the CSF, dehydrating the brain parenchyma. The pressure inside the collection was always lower than 5 mmHg, but, based on Waziri et al. suggestions, it can be speculated that if pressure had been higher, then hydrostatic pressure would have pushed water away into the vessels. It is remarkable that, at the time of patient deterioration, no asymmetric neurologic signs were observed. Decerebration posture was bilateral from the beginning, and no pupil asymmetries were present. It can be speculated that patient condition could have been caused by a relatively local ionic disturbance due to parenchyma dehydration. The fact that patient hemiparesis, prior to the deterioration episode, was slowly recovering despite the growing subdural effusion reinforces this opinion.
Figure 3.
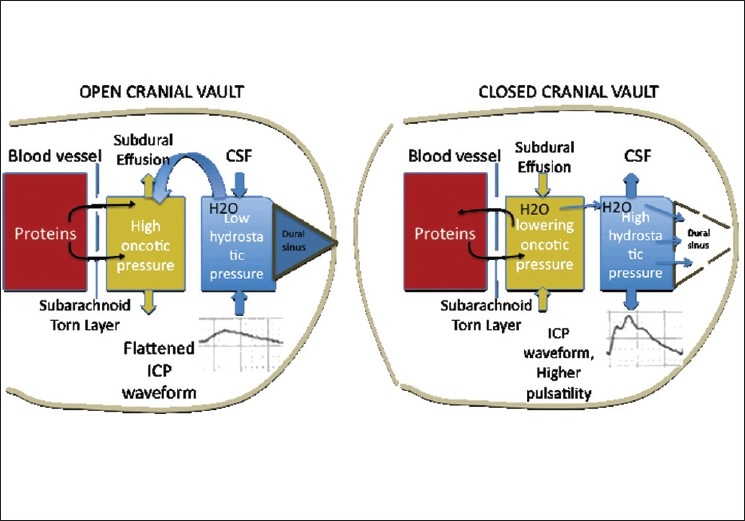
Open cranial Vault: the abnormal permeability allows the protein leakage, thus increasing the oncotic pressure of the subdural effusion, and drawing water. With the decompressive craniectomy, the arterial pulsatility does not properly transmit to the Cerebrospinal fluid, and normal reabsorption through the arachnoid villi is impaired. Closed Cranial Vault: the Intracranial Pressure waveform resumes its shape, and water reabsorption restarts, solving the collection
Electron microscopy studies have indicated that there is no dead space between the dura and arachnoid layers.[5,15] If either the trauma or the surgery breaks the inner layer of the dura, CSF will fill a virtual space between the aforementioned dura and arachnoid layers. Separating these layers will alter its permeability properties. The higher permeability will perpetuate the process. Normal permeability will not be restored until those layers are put together again. It can be hypothesized that cranioplasty reduces compliance and increases the amplitude of the dicrotic ICP waveform,[1,4 7,9,13 17,23] leading to reabsorption, progressive reduction of the fluid collection, and restoration of normal microanatomy, and thus permeability.
CONCLUSION
The incidence rate of subdural collections in head trauma is between 7 and 12%, and it is between 21 and 50% after DC. 92% of them are ipsilateral to the DC. Most of them resolve spontaneously, but are more likely not to resolve if they are contralateral to DC. Few subdural czollections will become symptomatic and will need evacuation. Symptoms might be due to the mass effect or local ionic disturbances. When they become symptomatic, cranioplasty might be the definitive solution. Further studies are needed to assess the role of cranioplasty in the resolution of these collections. Further validation of this classification and nomenclature is needed, and detailed understanding of underlying pathogenesis will be helpful to predict what patients will develop a subdural collection, and which ones will require aggressive treatment.
Contributor Information
Igor Paredes, Email: igorparedes@gmail.com.
Marta Cicuendez, Email: marta.cicuendez@gmail.com.
Manuel A. Delgado, Email: manuelamosadelgado@hotmail.com.
Rafael Martinez-Pérez, Email: rafa11safin@hotmail.com.
Pablo M Munarriz, Email: pablomunarriz@hotmail.com.
Alfonso Lagares, Email: algadoc@yahoo.com.
REFERENCES
- 1.Aarabi B, Chesler D, Maulucci C, Blacklock T, Alexander M. Dynamics of subdural hygroma following decompressive craniectomy: A comparative study. Neurosurg Focus. 2009;26:E8. doi: 10.3171/2009.3.FOCUS0947. [DOI] [PubMed] [Google Scholar]
- 2.Eide PK, Brean A. Cerebrospinal fluid pulse pressure amplitude during lumbar infusion in idiopathic normal pressure hydrocephalus can predict response to shunting. Cerebrospinal Fluid Res. 2010;7:5. doi: 10.1186/1743-8454-7-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Eide PK, Sorteberg W. Association among intracranial compliance, intracranial pulse pressure amplitude and intracranial pressure in patients with intracranial bleeds. Neurol Res. 2007;29:798–802. doi: 10.1179/016164107X224132. [DOI] [PubMed] [Google Scholar]
- 4.Guidelines for the Management of Severe Traumatic Brain Injury. J Neurotrauma. 2007;24(Suppl 1):S1–S106. doi: 10.1089/neu.2007.9999. [DOI] [PubMed] [Google Scholar]
- 5.Haines DE, Harkey HL, al-Mefty O. The “subdural” space: A new look at an outdated concept. Neurosurgery. 1993;32:111–20. doi: 10.1227/00006123-199301000-00017. [DOI] [PubMed] [Google Scholar]
- 6.Herold TJ, Taylor S, Abbrescia K, Hunter C. Post-traumatic subdural hygroma: Case report. J Emerg Med. 2004;27:361–6. doi: 10.1016/j.jemermed.2004.03.018. [DOI] [PubMed] [Google Scholar]
- 7.Honeybul S. Complications of decompressive craniectomy for head injury. J Clin Neurosci. 2010;17:430–5. doi: 10.1016/j.jocn.2009.09.007. [DOI] [PubMed] [Google Scholar]
- 8.Honeybul S, Ho KM, Lind CR, Gillett GR. Decompressive craniectomy for neurotrauma: The limitations of applying an outcome prediction model. Acta Neurochir (Wien) 2010;152:959–64. doi: 10.1007/s00701-010-0626-5. [DOI] [PubMed] [Google Scholar]
- 9.Kaen A, Jimenez-Roldan L, Alday R, Gomez PA, Lagares A, Alen JF, et al. Interhemispheric hygroma after decompressive craniectomy: Does it predict posttraumatic hydrocephalus? J Neurosurg. 2010;113:1287–93. doi: 10.3171/2010.4.JNS10132. [DOI] [PubMed] [Google Scholar]
- 10.Kilincer C, Hamamcioglu MK. Surgical complications of decompressive craniectomy for head trauma. Acta Neurochir (Wien) 2010;152:557–8. doi: 10.1007/s00701-009-0476-1. [DOI] [PubMed] [Google Scholar]
- 11.Lee KS. The pathogenesis and clinical significance of traumatic subdural hygroma. Brain Inj. 1998;12:595–603. doi: 10.1080/026990598122359. [DOI] [PubMed] [Google Scholar]
- 12.Lee KS, Bae WK, Bae HG, Yun IG. The fate of traumatic subdural hygroma in serial computed tomographic scans. J Korean Med Sci. 2000;15:560–8. doi: 10.3346/jkms.2000.15.5.560. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Li G, Wen L, Zhan RY, Shen F, Yang XF, Fu WM. Cranioplasty for patients developing large cranial defects combined with post-traumatic hydrocephalus after head trauma. Brain Inj. 2008;22:333–337. doi: 10.1080/02699050801958353. [DOI] [PubMed] [Google Scholar]
- 14.Miranda P, Lobato RD, Rivas JJ, Alen JF, Lagares A. [Postraumatic subdural collections: Case report and review of the literature] Neurocirugia (Astur) 2004;15:67–71. [PubMed] [Google Scholar]
- 15.Schachenmayr W, Friede RL. The origin of subdural neomembranes.I.Fine structure of the dura-arachnoid interface in man. Am J Pathol. 1978;92:53–38. [PMC free article] [PubMed] [Google Scholar]
- 16.John JN, Dila C. Traumatic subdural hygroma in adults. Neurosurgery. 1981;9:621–6. doi: 10.1227/00006123-198112000-00002. [DOI] [PubMed] [Google Scholar]
- 17.Stiver SI. Complications of decompressive craniectomy for traumatic brain injury. Neurosurg Focus. 2009;26:E7. doi: 10.3171/2009.4.FOCUS0965. [DOI] [PubMed] [Google Scholar]
- 18.Stone JL, Lang RG, Sugar O, Moody RA. Traumatic subdural hygroma. Neurosurgery. 1981;8:542–50. doi: 10.1227/00006123-198105000-00005. [DOI] [PubMed] [Google Scholar]
- 19.Su FW, Ho JT, Wang HC. Acute contralateral subdural hygroma following craniectomy. J Clin Neurosci. 2008;15:305–7. doi: 10.1016/j.jocn.2006.08.019. [DOI] [PubMed] [Google Scholar]
- 20.Wang HK, Lu K, Liang CL, Tsai YD, Wang KW, Liliang PC. Contralateral subdural effusion related to decompressive craniectomy performed in patients with severe traumatic brain injury. Injury. 2010 Jul 6; doi: 10.1016/j.injury.2010.06.004. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 21.Waziri A, Fusco D, Mayer SA, McKhann GM, Connolly ES Jr. Postoperative hydrocephalus in patients undergoing decompressive hemicraniectomy for ischemic or hemorrhagic stroke. Neurosurgery. 2007;61:489–93. doi: 10.1227/01.NEU.0000290894.85072.37. [DOI] [PubMed] [Google Scholar]
- 22.Welch K, Friedman V. The cerebrospinal fluid valves. Brain. 1960;83:454–69. doi: 10.1093/brain/83.3.454. [DOI] [PubMed] [Google Scholar]
- 23.Yang XF, Wen L, Li G, Zhan RY, Ma L, Liu WG. Contralateral subdural effusion secondary to decompressive craniectomy performed in patients with severe traumatic brain injury: Incidence, clinical presentations, treatment and outcome. Med Princ Pract. 2009;18:16–20. doi: 10.1159/000163040. [DOI] [PubMed] [Google Scholar]
- 24.Yang XF, Wen L, Shen F, Li G, Lou R, Liu WG, et al. Surgical complications secondary to decompressive craniectomy in patients with a head injury: A series of 108 consecutive cases. Acta Neurochir (Wien) 2008;150:1241–7. doi: 10.1007/s00701-008-0145-9. [DOI] [PubMed] [Google Scholar]
- 25.Yang XJ, Hong GL, Su SB, Yang SY. Complications induced by decompressive craniectomies after traumatic brain injury. Chin J Traumatol. 2003;6:99–103. [PubMed] [Google Scholar]
- 26.Zanini MA, de Lima Resende LA, de Souza Faleiros AT, Gabarra RC. Traumatic subdural hygromas: proposed pathogenesis based classification. J Trauma. 2008;64:705–713. doi: 10.1097/TA.0b013e3180485cfc. [DOI] [PubMed] [Google Scholar]
- 27.Zanini MA, Resende LA, Freitas CC, Yamashita S. Traumatic subdural hygroma: Five cases with changed density and spontaneous resolution. Arq Neuropsiquiatr. 2007;65:68–72. doi: 10.1590/s0004-282x2007000100015. [DOI] [PubMed] [Google Scholar]