An official website of the United States government
Here's how you know
Official websites use .gov
A
.gov website belongs to an official
government organization in the United States.
Secure .gov websites use HTTPS
A lock (
) or https:// means you've safely
connected to the .gov website. Share sensitive
information only on official, secure websites.
As a library, NLM provides access to scientific literature. Inclusion in an NLM database does not imply endorsement of, or agreement with,
the contents by NLM or the National Institutes of Health.
Learn more:
PMC Disclaimer
|
PMC Copyright Notice
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
There are marked disparities in the frequency of spinal surgery performed within the United States over time, as well as across different geographic areas. One possible source of these disparities is the criteria for surgery.
Methods
During a one-year period [November 2009-October 2010], the senior author, a neurosurgeon, saw 274 patients for cervical and lumbar spinal, office consultations. A patient was assigned to the “unnecessary surgery” group if they were told they needed spinal surgery by another surgeon, but exhibited pain alone without neurological deficits and without significant abnormal radiographic findings [dynamic X-rays, MR scans, and/or CT scans].
Results
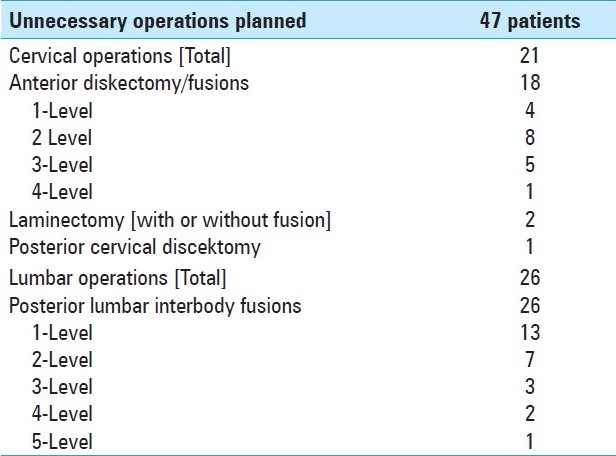
Of the 274 consults, 45 patients were told they needed surgery by outside surgeons, although their neurological and radiographic findings were not abnormal. An additional 2 patients were told they needed lumbar operations, when in fact the findings indicated a cervical operation was necessary. These 47 patients included 21 [23.1%] of 91 patients with cervical complaints, and 26 [14.2%] of 183 patients with lumbar complaints. The 21 planned cervical operations included 1-4 level anterior diskectomy/fusion [18 patients], laminectomies/fusions [2 patients], and a posterior cervical diskectomy [1 patient]. The 26 planned lumbar operations involved single/multilevel posterior lumbar interbody fusions: 1-level [13 patients], 2-levels [7 patients], 3-levels [3 patients], 4-levels [2 patients], and 5-levels [1 patient]. In 29 patients there were one or more overlapping comorbidities.
Conclusions
During a one-year period, 47 [17.2%] of 274 spinal consultations seen by a single neurosurgeon were scheduled for “unnecessary surgery”.
Keywords: Cervical, frequency, lumbar, unnecessary spinal surgery
INTRODUCTION
Although one spine surgeon may decide that a patient needs surgery, another surgeon [e.g. a second opinion] might decide that surgery is “unnecessary”. Here we define “unnecessary surgery” as spinal surgery based upon “pain alone”. That is, the patient has no neurological deficit and no significant abnormal radiographic findings on dynamic X-rays, MR, and/or CT. Surgeons can, and do, debate whether it is appropriate to operate on patients with pain alone. To put this debate in context, however, we need to better understand the number of patients involved and the type of procedures recommended. In this prospective study performed over a one-year period, a single neurosurgeon documented the “unnecessary” lumbar and cervical surgeries planned by other spinal surgeons.
MATERIALS AND METHODS
A single neurosurgeon prospectively evaluated all office-based neurosurgical consultations performed for cervical or lumbar disease over a one-year period, from November 2009 to October 2010. A subset of patients, seen as “second opinions” [as requested by the patient], was scheduled by outside surgeons for spinal operations. Of this group, those who did not warrant, in the opinion of the senior author, spinal surgery were identified. All of these patients reported pain alone. The opinion that these proposed spinal procedures were “unnecessary” was based on 2 criteria: [1] there were no focal neurological deficits, and [2] there was no significant abnormal surgical pathology on radiographic studies [dynamic X-rays, and MR and/or CT]. This included MR-documented “black discs” which reflect resorption without herniation, wherein degenerative changes are confined to the disc space without attendant neural compression [nerve root, cauda equina, conus].
The types of operations scheduled by other spinal surgeons were ascertained from the patient. In addition, the frequencies of major co-morbid factors were also assessed, as performing surgery in such cases could place these individuals at increased risk.
RESULTS
During the one-year period, other spinal surgeons recommended “unnecessary surgery” for 47 [17.2%] of 274 patients seen with cervical or lumbar complaints [Table 1]. The average age of this group was 50.5±12.6 yrs and 28 were male, while 19 were female. All 47 patients complained of pain and 45 of them were without focal neurological deficits and radiographic abnormalities. The remaining two had clear neurological and radiographic findings consistent with cervical disease, but were told they needed lumbar operations.
Of the 91 patients seen for cervical complaints, 21 [23%] were told they needed the following operations: 1-4 level anterior cervical diskectomy/fusions [18 patients]; laminectomies [with/without fusion: 2 patients], and a posterior diskectomy [1 patient] [Table 1]. Of interest, two patients had been told that they needed emergency cervical operations, when they in fact had no neurological deficits or significant radiographic abnormalities. Of the 183 patients seen for lumbar complaints, 26 [14.2%] were told they needed one to 5 level posterior lumbar interbody fusions [Table 1].
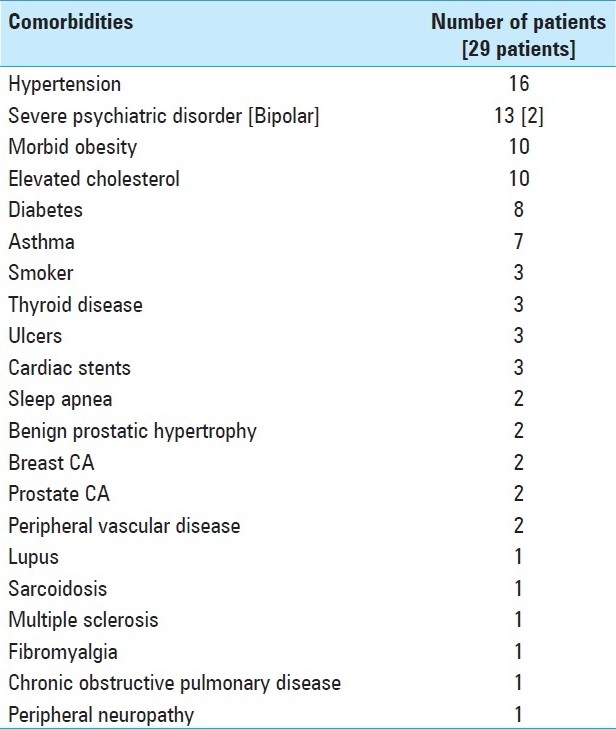
Twenty-nine of these 47 patients also exhibited significant and often multiple, overlapping comorbidities, while only 18 were without comorbidities [Table 2]. The most common comorbidities were: hypertension [16 patients], psychiatric disorders [13; 2 with bipolar disorder], morbid obesity [10 patients], elevated cholesterol [10 patients], diabetes [8 patients], and asthma [7 patients].
Table 2.
Major Co-morbid Factors in 29 [62%] of 47 Patients Scheduled For Unnecessary Spinal Surgery
Some of the 47 patients actually had other diseases that might have been the cause of their pain. These included lupus [1 patient], multiple sclerosis [1 patient], and fibromyalgia [1 patient]. In addition, 2 patients scheduled for “unnecessary” lumbar surgery, in fact had cervical disease; they later successfully underwent cervical surgery.
DISCUSSION
There are marked disparities in the frequency of spinal surgery performed within the United States over time, as well as across different geographic areas.[1–3] One study cited a 20% increase in the US hospitalization rate for low back surgery between 1978 and 1985.[2] Another study, based on the annual national survey of hospitalization from 1979-1985, documented that cervical spine operations increased by 45%, cervical fusions by 70%, lumbar surgery by 33%, and lumbar fusions by 60%.[1] Utilizing the Utah Medicare database (1984-1990), a 20% greater incidence of laminectomy and disc removal was documented in the state of Utah compared with the national average, with a 50% disparity in surgical rates observed for different geographical areas within Utah itself.[3] Similarly, variations were observed in the number of patients undergoing surgery for lower back pain in different geographical areas in Iowa.[2]
One possible source of these disparities is the criteria for spine surgery. For example, while some surgeons will operate on a patient with pain alone, [i.e. without neurological or radiographic abnormalities], other surgeons consider such surgery “unnecessary”. To get a better understanding of this population, this prospective study was performed.
Of the 274 patients seen in consultation in a single year, 45 were scheduled for “unnecessary surgery”, [i.e. based upon pain alone]. While these 45 patients experienced pain, they exhibited no neurological deficits, and, based upon review of the X-ray, MR, and/or CT studies showed no significant abnormal radiographic findings. Therefore, there was no clear surgical procedure that would benefit the patient. Nevertheless, spinal surgery, often quite extensive was recommended. Furthermore, an additional 2 patients were scheduled for unnecessary lumbar operations, when in fact they needed cervical surgery.
Three of the 45 patients with only pain had other disease entities that may have caused their pain e.g. multiple sclerosis, fibromyalgia, and lupus. In addition, 29 of these patients had overlapping comorbidities, many major, which would have increased the risks associated with “unnecessary” spinal surgery.
Some surgeons will argue that pain alone, particularly in patients who have exhausted conservative treatment modalities [e.g. anti-inflammatories, physical therapy, epidural steroids] over a 3-6 month period, justifies spinal surgery. Even if we accept this argument, which we do not, it does not justify the wrong operation, or extensive multi-level procedures. Furthermore, how do you justify operating on a patient with pain alone, when there are major, overlapping, potentially life-threatening co-morbidities? For example, three of the patients in this study had cardiac stents and were on both aspirin and Plavix. Why would you risk a fatal myocardial infarction for an operation on these patients?
In summary, one cannot use these numbers to get a regional, much less national, estimate of the frequency of recommended “unnecessary” spinal surgery. In this study, 47 out of 274, or 17.2%, of the total number of patients seen in a single year were scheduled for unnecessary surgery. This is an underestimate of the percentage of unnecessary surgeries as the 274 patients include those coming for first opinions. If we only considered the patients coming for second opinions, then the percentage of unnecessary operations would have been considerably larger. Unfortunately, we did not keep track of the total number of consults for whom surgery was recommended. In any case, it is clear that it is rather common. Many spine surgeons would agree with the senior author that none of the 47 patients seen in a single year should undergo the surgery proposed. Many would also agree that “unnecessary” surgical procedures are uncalled for in the presence of serious comorbidities. In the interest of our patients, as well as in the interest of reducing medical costs, a better understanding of frequency of “unnecessary” spinal surgery is needed.
1.Davis H. Increasing rates of cervical and lumbar spine surgery in the United States, 1979-1990. Spine. 1994;19:1117–23. doi: 10.1097/00007632-199405001-00003. [DOI] [PubMed] [Google Scholar]
3.Nilasena DS, Vaughn RJ, Mori M, Lyon JL. Surgical trends in the treatment of disease of the lumbar spine in Utah's Medicare population, 1984-1990. Med Care. 1995;33:585–97. doi: 10.1097/00005650-199506000-00002. [DOI] [PubMed] [Google Scholar]
Unnecessary.- “used for describing something that should not have happened because it could have been avoided”. A strong ‘statement’ - particularly if coming from one professional criticizing another. Although, I fundamentally agree with the principles addressed by the author, I question the validity of the methodology employed to justify such. Let's face it, we (Neurosurgeons) collectively do far too much spine surgery. The most challenging aspect of the ‘unnecessary spine surgery discussion’, however, is the clarification of the definition of ‘unneccessary’. Unfortunately, what is ‘unnecessary’ to some, may be ‘necessary’ to others. We have much to learn in this arena. We should all ‘stay tuned’.
This paper is interesting in that virtually every neurosurgeon has had similar experiences to a greater or lesser degree. There are three reasons for unnecessary spinal fusions: greed, ignorance and stupidity. To illustrate this are situations that I have come across in my 46 years in practice.
Greed: A hospital reviewing surgical procedures noted that a significant number of patients scheduled for anterior lumbar interbody fusions did not meet criteria. The committee requested that any spine surgeon contemplating this surgery had to have the chart reviewed by another spine surgeon at that hospital. ALIF procedures dropped by 75%. Greed is not a malady of just spine surgeons. The same committee began to investigate cardiac catheterizations, which had a very high rate of normal studies. This is a big money maker for a hospital. The solution for the administration was to disband the committee. Most physicians will remember the number of cataract operations that were being done on nursing home residents, many of whom were confined to wheelchairs. At that time Medicare paid $1800 per eye – a gold mine for the ophthalmologist. Medicare solved the problem by reducing the fee to $600. And then there is the greed of the medical supply company. When the spine surgeons in a hospital were requested by the administration to utilize one or two pedicle screws determined by bid, all the companies suddenly cut the price in half – for screws that nobody would pay $50 for at the Home Depot.
Ignorance: As this paper also notes, the wrong operation is sometimes suggested. For another example is the middle-aged lady who was told by a spine surgeon she needed a four level anterior cervical discectomy and fusion for degenerative disease reported on MRI. Her complaint was radiating pain into her left forefinger. She sought out a second opinion. This spine surgeon noted weakness of the left triceps and reviewed the MRI, which showed a foraminal ruptured disc at left C6-C7 and missed by the radiologist. The problem was resolved by simple discectomy. The primary surgeon failed to listen to the patient, examine her adequately and put too much faith in the radiologist.
Stupidity: I guess we all do something that in retrospect we realize was probably stupid. But this case I think has to be a classic. A well-respected spine surgeon was challenged for having, over the period of a few years, fused every vertebrae but one in a patient. When challenged, his answer was that ‘the patient wanted it’. I hope that a physician can have a better reason for treating a patient than that.
I’m not sure what can be done to eliminate the sporadic cases of ignorance and stupidity. Maybe to some degree the fear of legal action may be of value. I doubt it, however, because the truth is learned after the fact.
The big problem is greed. I hate to say it but most neurosurgeons want to do spine surgery because, at this time, it is lucrative. What is the solution – and there will be one. Either we solve the problem or the government will. I suggest that every hospital doing spine fusions establish a review committee to which the chart on every patient to be scheduled for fusion is reviewed to be sure that appropriate criteria are met. I suspect that this will reduce spine fusions by 20% or more. If we continue to ignore the problem then the government will step in, in a global fashion, by severely cutting the reimbursement for spinal fusion to the point that it will not pay to do that operation. Or worse, we will all be employees of the hospital or government.
My biggest concern is with the authors determination of what constitutes unnecessary surgery. The author claims that if he doesn’t feel there is a significant disc abnormality and in the absence of a neurological deficit, surgery should not have been recommended. Clinically significant disc disease is misinterpreted as “normal” or “insignificant” on a daily basis by physicians everywhere. I cannot possibly overemphasize this point. Many surgeons overlook significant disc injuries or brush them off as “normal” because they are misreading the MRI study. It is an unfortunate but real issue we deal with regularly. For example, most surgeons focus on central stenosis in the lumbar spine but I have found lateral recess and foramenal stenosis to be far more symptomatic and prevalent. Unfortunately clinically significant lateral recess and foramenal stenosis are frequently missed by both radiologists and surgeons alike and the patients are left to suffer with the symptoms for years before anyone recognizes the mistake. This author claims that the MRIs were without significant disease but obviously the surgeons recommending treatment would likely disagree. I can’t help but wonder how many patients may be suffering needlessly right now because they were denied definitive treatment by this author.
Back and neck pain come from specific sources. Successful treatment and cure are possible in over 95% of patients suffering with back and neck pain. The difficulty is in making the right diagnosis. Back pain most commonly originates from facet joints, sacroiliac joints, piriformis muscle, paraspinal muscles, and the disc (discogenic back pain). Fractures, infection and tumors are much less common. Facet pain is best treated with facet block and therapy with or without rhizotomy. Muscular pain is best treated with behavioral modification, therapy, medications and injections into the affected muscle. Sacroileitis or inflammation of the sacroiliac joint is best treated with injection directly into the joint combined with therapy while recurrent pain responds well to rhizotomy. Discogenic back pain in my experience requires surgery to eliminate the pain. Discogenic back pain is pain emanating from a pain sensitive structure within an abnormal disc. The pain generator in the disc is almost always the annulus and the pathophysiology is an annular tear with sensitized nerve fibers from the sinovertebral nerve.
In my opinion, discogenic pain responds best to surgery that addresses the abnormal disc material and pain generator. Surgery that removes or repairs the pain sensitive structures within the abnormal disc is very successful at curing the patients discogenic back or neck pain.
When more than one source of pain is present, I recommend treating the nonoperative causes first with therapy and injections. Patients with medically refractory discogenic back pain and an abnormal disc with annular tear on MRI do very well with surgery including fusion.
1Associate Professor, Neurosurgery, University of Illinois, Chicago (Ret.) Center for Pain Treatment and Rehabilitation, Lake Forest Hospital, Lake Forest, Illinois (Ret.) E-mail: ron@pawl.com
1Associate Professor, Neurosurgery, University of Illinois, Chicago (Ret.) Center for Pain Treatment and Rehabilitation, Lake Forest Hospital, Lake Forest, Illinois (Ret.) E-mail: ron@pawl.com
In the Pain Treatment and Rehabilitation Center of Lake Forest Hospital in Lake Forest, Illinois, where I served as Senior Neurosurgical Consultant and Medical Director for 30 years, the most common chronic pain disorders were related to low back conditions and the second most common were from other spinal conditions. Every patient referred into the Center is evaluated by a multidisciplinary team consisting of a nurse, a physical and/or occupational therapist, a physician and a psychologist. All patients, with few exceptions for linguistic reasons, take the Minnesota Multiphasic Personality Inventory. The most common physical findings are, as is described in this paper in those patients deemed to have been scheduled for unnecessary surgery, no evidence of a neurologic disorder that could explain the pain. Too many had already been subjected to surgical intervention and there were findings consistent with the intervention itself, such as scarring and stiffness of segments fused. The most common psychological finding on exam and testing is somatization, the conversion of emotional stress into bodily complaints and a bodily focus so intense that normal bodily functions are interpreted as painful. Secondary gains psychologically also play a significant role. Some patients, as in this paper, did have severe psychiatric disorders, but somatization is not usually considered a severe psychiatric disorder.
Unnecessary spinal surgery has been recognized as an important issue in spine surgery.[5] In workman's compensation cases it has become common for patients to be sent by the insurance carrier for a second opinion when spine surgery has been recommended, at least in Illinois. Trauma is known to cause somatiform pain disorders,[4] hence a good reason for caution by the insurance carriers when spinal surgery is recommended after a job related injury.
Although these authors did not make any specific recommendations to correct the situation of unnecessary spinal surgery, outside of making the readership aware of the problem by the publication, in Europe a spine registry has been opened[6] with the thought that such a registry will make the study of spine surgery more general. That idea might be a beginning to evaluating and hopefully resolving the issue of unnecessary surgery.
References
4.Schmelzer-Schmied N, Henningsen P, Schiltenwolf M. Somatoform pain disturbance as the result of trauma. Orthopade. 2006 Dec;35(12):1265–8. doi: 10.1007/s00132-006-1009-8. [DOI] [PubMed] [Google Scholar]
5.Deyo RA, Mirza SK. The case for restraint in spinal surgery: does quality management have a role to play? Eur Spine J. 2009 Aug;18(Suppl 3):331–7. doi: 10.1007/s00586-009-0908-x. Epub 2009 Mar 6. [DOI] [PMC free article] [PubMed] [Google Scholar]
6.Roder C, Muller U, Aebi M. The rationale for a spine registry. Eur Spine J. 2006 Jan;15(Suppl 1):S52–6. doi: 10.1007/s00586-005-1050-z. Epub 2005 Nov 16. [DOI] [PMC free article] [PubMed] [Google Scholar]
The current article describes the problem of the surgical indications in degenerative spine diseases. The goal of such a surgery is to treat the pain the outlines of which are difficult to define without an absolute medical criterion allowing to retain an indisputable surgical indication. However, a multidisciplinary approach[7] and the respect of the state of art permit one to obtain good functional results particularly when there is a mechanical compression of the cord or the nerve roots consistent with the clinical, radiological and neurophysiological picture. All spine surgeons retain the following criteria that weigh down the results: a psychiatric background, occupational accidents, a medico-legal context and an “ambiguous” clinical examination.
This series includes psychiatric patients, cases without radiological precision and a predominance of “fusions” justified essentially on the notion of “instability” whose criteria are not established[8]. The results of this kind of surgical procedure are poor with a significant morbidity leading to a therapeutic and financial higher bid. This article challenges: either the surgeons are inefficient or they are driven by commercialism. The first assumption seems unlikely considering that their technicality has been validated by various examinations and competitions. The second assumption can be retained. Consequently, it is advisable to suggest an inhibiting system targeting the financial aspect. The US spent approximately $2.2 trillion on health care in 2007.[10] Health care costs doubled from 1996 to 2006.[9] The incidence of spinal fusion procedures increased from 60,973 cases in 1993 to 350,754 cases in 2007.[11] Thus, the refunding of the acts should be carried out only after validation of a decision which must be collegial and multidisciplinary associating neurosurgeons, physiotherapists, psychological clinicians as well as a study of the socio-economic situation of the patient.
References
7.Chou R, et al. Interventional therapies, surgery, and interdisciplinary rehabilitation for low back pain. An evidence-based Clinical Practice Guideline from the American Pain Society. Spine. 2009;34:066–1077. doi: 10.1097/BRS.0b013e3181a1390d. [DOI] [PubMed] [Google Scholar]
9.Orszag PR. Growth in Health Care Costs: Testimony before the Committee on the Budget, United States Senate. 2008. Jan 31, [Accessed March 10, 2010]. (
http://www.cbo.gov/doc.cfm?index=8948.
)
The authors retrospectively reviewed a one year experience with patients presenting for a second opinion on spinal surgery and report that “unnecessary surgery” was recommended by the primary surgeon 17.4% of the time. Unnecessary surgery was defined as surgery to treat pain without focal neurological deficits in the setting of no significant abnormal surgical pathology on radiographic studies (dynamic X-rays, and MR and/or CT). It is not clear if all patients had all studies. There is no description of sagittal alignment, facet arthropathy, or other less frequent pathologies. All spine surgeons try to filter through secondary gain issues and biases which may influence patient behavior but if one accepts the premise that these patients truly have pain then there must be a source. The first and foremost task is to identify this source and in addition to standard imaging studies a comprehensive evaluation may include bone scans and diagnostic injections which were not mentioned in this article.
Experienced and respected spinal surgeons regularly debate in conference forums how to manage specific cases. Disagreement on what to do, when to do it, and how to do it occurs more frequently than consensus. These debates highlight the deficiencies in our knowledge and understanding of degenerative, inflammatory, and mechanical spinal pathology. It is not surprising that the author came to a different conclusion in almost a fifth of the cases and it could be that a portion of these patients really could be managed with or without surgery. However, that cannot be true for all. The real message here is that there are surgeons recommending procedures without identifying the causative factor. Most of these procedures involved fusion which is more aggressive both biologically and economically as compared to nonoperative management or simple decompressions. Fusion was recommended for all of the lumbar procedures and half of these procedures were multilevel. The evidence supporting multilevel lumbar fusion for axial pain is very weak and even if the authors missed some cases of facet arthropathy this entity does not require a multilevel fusion.
The majority of spinal surgeons strive to diagnose and manage patients in a responsible, professional, and ethical manner consistent with the evidence that is available. Unfortunately there are outliers who either provide suboptimal evaluation and treatment or, more frequently, perform unnecessary expensive and potentially dangerous procedures. Some control is achieved by denials from insurance carriers and from fear of litigation but this is not enough. The specialty must continue to search for ways to identify and either re-educate or limit the privileges of rogue surgeons while sending a strong message to society that spine surgery can be effective when reserved for the proper indications.
1Professor Emeritus Aichi Medical University President, Global Spine Inc. 2-83-602 Issha, Meito-ku, Nagoya 465-0093 Japan E-mail: h-nakagawa@mediacat.ne.jp
1Professor Emeritus Aichi Medical University President, Global Spine Inc. 2-83-602 Issha, Meito-ku, Nagoya 465-0093 Japan E-mail: h-nakagawa@mediacat.ne.jp
This is a very interesting and invaluable paper which clarified the present situation of the practices in spinal surgery in the United States.
I have been practicing spinal surgery in Japan since 1980, when I came back after a 12-year clinical experience of Neurosurgery in the United States. Since that time the clinical practice of spinal surgery has greatly changed in the United States and in Japan with further development of advanced neuroimaging, microsurgery and instrumentation.
Through the communication with friends practicing neurosurgery in the US and with information from journals and meetings, I have noticed many different points in the rate and method of spinal surgery in the US and the other countries including Japan.
As pointed out by the author, “unnecessary” spinal surgery was 17.2% in spinal consultation for the second opinion and overlapping comorbidities are as many as 29 out of 47 (62%).
Significant increase of the rate of spinal surgery is attributed mainly to the development of diagnostic tools and operative techniques and implants in addition to increasing aged population in most countries. However, the situation in the US seems to be a little bit different because of unusually high rate of spinal surgery.
I am afraid that “unnecessary” spinal surgery and also “oversurgery” may be related to the money-oriented society which will subsequently jack up the medical costs and increase the rate of malpractice insurance.
This kind of a vicious cycle has to be avoided in the US and any other countries.
In this sense this paper is of great value and each neurosurgeon including me reevaluate our stance of surgical indication in our practice of spinal surgery.