

Abstract
Community-acquired pneumonia due to Pseudomonas aeruginosa in previously healthy individuals is a rare disease that is associated with high fatality. On 14 February 2010 a previously healthy 49-year-old woman presented to an emergency room with signs and symptoms of pneumonia, 2 days after returning from a spa holiday in a wellness hotel. Blood cultures and respiratory specimens grew P. aeruginosa. Despite adequate antimicrobial therapy, the patient died of septic multiorgan failure on day nine of hospitalization. On February 26, nine water samples were taken from the hotel facilities used by the patient: In the hot tub sample 37,000 colony-forming units of P. aeruginosa/100 ml were detected. Two of five individual colonies from the primary plate used for this hot tub water sample were found to be genetically closely related to the patients’ isolates. Results from PFGE, AFLP and MLST analysis allowed the two lung isolates gained at autopsy and the whirlpool bathtub isolates to be allocated into one cluster. The patient most likely acquired P. aeruginosa from the contaminated water in the hotel’s hot tub. The detection of P. aeruginosa in high numbers in a hot tub indicates massive biofilm formation in the bath circulation and severe deficiencies in hygienic maintenance. The increasing popularity of hot tubs in hotels and private homes demands increased awareness about potential health risks associated with deficient hygienic maintenance.
Keywords: Pseudomonas aeruginosa, Pneumonia, Community acquired, Whirlpool, Hot tub, Jacuzzi, PFGE, AFLP, MLST
Introduction
Pseudomonas aeruginosa is widespread in soil, water and other moist environments. It is extremely adaptable, has low nutrient requirements and can live at variable pH and temperature conditions [1]. It is also an important opportunistic pathogen, especially in the hospital setting, and the respiratory tract is the most frequent site of such infections [1]. The typical patient presenting with nosocomial P. aeruginosa infection is ventilated mechanically, has slowly progressive lung infiltrates and has been colonized with this pathogen for days [1]. However, acute pneumonia due to P. aeruginosa has also been seen in the community, for example, among individuals who have inhaled contaminated hot tub steam [2].
We report here on a fatal case of community-acquired P. aeruginosa pneumonia in a previously healthy 49-year-old German woman following a vacation at a wellness resort in Austria. Water samples from the whirlpool bathtub (hot tub) in the implicated apartment yielded high numbers of P. aeruginosa genetically closely related to isolates that had grown in lung samples obtained post mortem.
Case report
On 14 February 2010 a previously healthy 49-year-old woman presented to the emergency room of a German hospital, 2 days after returning from a spa holiday in a wellness hotel in Austria. She complained of severe chest pain with productive cough, supposedly without fever or chills. With the exception of smoking (at least 25 pack-years), there were no underlying risk factors. Initial physical examination revealed normal body temperature, blood pressure 60/40 mmHg, pulse 120/min and a respiratory frequency of 20/min. Laboratory examinations demonstrated elevated C-reactive protein (38.1 mg/dl, normal <0.5 mg/dl) and a white blood cell count of 3.94/nl (normal 4–11/nl). Antibiotic treatment was initiated with piperacillin/sulbactam [piperacillin 4 g three times daily plus sulbactam 1 g twice daily, intravenous (IV)] and moxifloxacin (400 mg once daily, IV). Blood cultures and respiratory specimens were taken and grew P. aeruginosa susceptible to piperacillin, piperacillin/sulbactam, ciprofloxacin and gentamicin when tested according to Clinical and Laboratory Standards Institute criteria [3]. PCR tests for influenza A virus, influenza B virus, cytomegalovirus, Epstein–Barr virus, herpes simplex virus and adenovirus were negative. A chest X-ray and computed tomography scan showed subtotal infiltration of the left lung. Due to rising partial pressure of carbon dioxide in the blood (pCO2) and respiratory acidosis the patient was transferred to a university hospital several hours after initial admission and extra-corporal membrane oxygenation (ECMO) was initiated. Blood cultures and respiratory specimens again grew P. aeruginosa. On February 22, day 9 of hospitalization, the patient died of septic multiorgan failure. Two lung specimens gained at autopsy grew P. aeruginosa.
Environmental investigation
The patient fell ill 2 days after returning from a 6-day vacation at an Austrian wellness resort. According to her companion, she had repeatedly used the apartment’s hot tub. On February 26, 1 day after receiving a request issued by a German court to investigate a possible causative role of the spa, nine water samples were taken by health officers from the hotel facilities used by the patient: (1) in the apartment, from the shower, the sink and the hot tub (usually with a working water temperature of 35°C); (2) in the hotel’s wellness area, from a sauna basin, two showers, a shower in a rest room (toilet area), a small outdoor pond (created for swimming) and a knee-deep pine bath. In the hot tub sample (water temperature at the time of sampling: 18°C) 37,000 colony-forming units (CFU) of P. aeruginosa/100 ml were detected. Another strain of P. aeruginosa was isolated at 5 CFU/100 ml from the shower in the patient’s room. All other samples were negative for P. aeruginosa.
Typing of isolates
Two P. aeruginosa isolates were available for typing from the patient. The isolates originated from the two lung samples taken at autopsy. Six water isolates comprising five individual colonies from the primary plate used for the hot tub water sample and one colony from the primary plate used for the water sample of the shower were arbitrarily selected for comparative analysis. Species identity was confirmed by biochemical testing (API 20 NE; BioMerieux, Marcy-l’Etoile, France) and by use of mass spectrometry (MALDI-TOF Biotyper; Bruker Daltonics, Bremen, Germany).
At the German reference centre for Gram-negative pathogens (Bochum, Germany), the eight isolates were typed by pulsed-field gel electrophoresis (PFGE), as described by Johnson et al. [4]. The patient’s two post-mortem lung isolates showed a PFGE band pattern indistinguishable from each other and were considered genetically indistinguishable according to the criteria by Tenover et al. [5]. From the six water isolates, four isolates (three from the hot tub and one from the shower) yielded PFGE patterns clearly distinguishable from those of the patient’s isolates and considered to be unrelated according to the criteria by Tenover et al. [5] The two remaining isolates (both from the tub) showed PFGE patterns highly similar to the lung isolates (Fig. 1). One water isolate differed from the patient’s isolates by an additional band explainable by a single insertion; the other differed by two additional bands, which could be explained either by a single insertion containing a SpeI restriction site or by two insertions. Both isolates can be regarded as being closely related based on the criteria of Tenover et al. [5]. Similar PFGE band patterns were not found among 60 P. aeruginosa isolates (49 clinical isolates, 11 environmental isolates) investigated in the laboratory performing the PFGE.
Fig. 1.
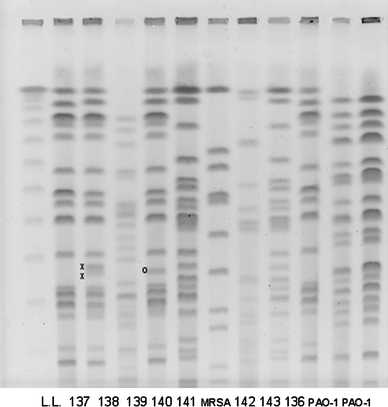
Pulsed-field gel electrophoresis patterns of Pseudomonas aeruginosa: Lanes: 136, 137 lung isolates, 138–143 water isolates. x The two additional bands (lane 138), o the one additional band (lane 140). MRSA (methicillin-resistant Staphylococcus aureus), PAO1 (Pseudomonas aeruginosa PAO1 strain) Internal controls
Natural diversity of PFGE patterns
In order to assess the epidemiological relevance of the minor differences observed among the PFGE patterns of P. aeruginosa from the two patient isolates and these two tub isolates, we prospectively collected 78 clinical isolates (from June 20 to July 10, 2010, provided by 11 hospital laboratories from 5 different provinces) to compare with the eight case-related isolates (two lung isolates, six water isolates) and two epidemiologically unrelated water isolates. The clinical isolates originated from wound swabs (n = 34), tracheal secretions (n = 14), ear swabs (n = 8), urine (n = 7), blood cultures (n = 4), sputum (n = 4), eye swabs (n = 2), tongue swab (n = 1), stool specimen (n = 1), drain (n = 1) and a percutaneous endoscopic gastrostomy (PEG) tube (n = 1); for one clinical isolate no specific information was available (n = 1).
The Austrian Agency for Health and Food Safety typed the 88 isolates by PFGE pattern analysis, as described above, by amplified fragment length polymorphism (AFLP) analysis and by multi-locus sequence typing (MLST). Genomic bacterial DNA (gDNA) for the AFLP and MLST analysis was extracted with the Quick Extract Bacterial DNA Extraction kit according to the manufacturer’s instructions (Epicentre Biotechnologies, Madison, WI). The AFLP analysis was performed using an AFLP Core Reagent kit (Life Technologies, Carlsbad, CA) for gDNA restriction, adaptor ligation and prePCR according to the manufacturer’s protocol [6]. MLST analysis was performed on all 88 isolates as described by Mansfeld et al. [7]. The sequences obtained were submitted to the P. aeruginosa PubMLST database (http://pubmlst.org/paeruginosa) [8]. Novel alleles and sequence types (STs) were submitted for allele and ST and clonal complex (CC) designations.
The 88 P. aeruginosa isolates were attributable to 56 sequence types as determined by MLST, to 80 PFGE types and to 74 AFLP types. Nine new alleles and 22 new STs, previously not available in the P. aeruginosa MLST database, were found [8]. Twelve STs comprised at least two different isolates. Twenty-two STs were assignable to ST groups within the MLST database using eBURST v3 (http://eburst.mlst.net) cluster analysis. The remaining 34 STs represented singletons.
The two lung isolates #74 and #75, the two hot tub water isolates #76 and #78 and an epidemiologically unrelated clinical isolate derived from tracheal secretions of a patient from the province Upper Austria (#27) belonged to ST-313 and could clearly be differentiated from the remaining 83 isolates (Fig. 2).
Fig. 2.

PFGE patterns (left column), amplified fragment length polymorphism patterns (AFLP, middle column) and multi-locus sequence typing (right column) of P. aeruginosa: isolate #27 from an epidemiologically unrelated patient, lung isolates #74 and #75 and water isolates #76 and #78. ST Sequence type
The AFLP pattern analysis of these five isolates revealed three different patterns (Fig. 2). One band of the epidemiologically unrelated isolate #27 had a lower molecular weight than the respective band of the two lung isolates #74 and #75 and the water isolate #78. The water isolate #76 lacked this band completely. The AFLP patterns of these five isolates were clearly different from those of the remaining 83 isolates, similar to the PFGE patterns being clearly different from those of the 83 isolates. PFGE pattern analysis revealed three different patterns (Fig. 2). The epidemiologically unrelated isolate #27 lacked one band present in the two lung isolates. One band of the water isolate #76 had a higher molecular weight than that of the respective band of the two lung isolates. The PFGE pattern of water isolate #78 was indistinguishable from that of the epidemiologically unrelated isolate #27. According to the criteria of Tenover et al. [5], the lung isolates and the water isolates from the tub can therefore to be considered as genetically closely related and as standing in an epidemiological context.
Discussion
Community-acquired P. aeruginosa infections are rare and tend to be mild and superficial. Examples include otitis externa, varicose ulcers, and folliculitis associated with jacuzzis [9]. There are only a few published reports of severe P. aeruginosa infections occurring in previously healthy persons without underlying diseases [2, 10–15]. However, community-acquired pneumonia due to P. aeruginosa in previously healthy individuals is associated with high fatality (over 30%) [12]. In the English literature from 1966 to 2000, there are 11 publications on 11 cases of community-acquired P. aeruginosa pneumonia in previously healthy persons, with a total of four fatalities [12]. The disease was associated with exposure to contaminated water aerosols in at least two of the 11 cases published: Alan et al. [13] reported on a case of community-acquired P. aeruginosa pneumonia associated with the use of a home humidifier, and Rose et al. [10] reported on P. aeruginosa pneumonia occurring following a single extended (90 min) exposure to contaminated water aerosols in a private home whirlpool. In 2003, Crnich et al. [2] reported on another case of community-acquired hot tub-associated necrotizing pneumonia in a previously healthy 40-year-old with a smoking history.
The patient described in our report most likely acquired P. aeruginosa from the contaminated water in the hotel’s hot tub. PFGE, AFLP and MLST analysis allowed the two lung isolates and the whirlpool bathtub isolates to be allocated into one cluster. The fact that the PFGE patterns of the lung isolates and the water isolates did not show 100% homology must not be misinterpreted as proof of non-clonality. P. aeruginosa is known to be highly mutational and, therefore, molecular typing methods are prone to over-discriminate. Smith et al. [16] have shown that DNA sequence mutations occur frequently during a patient’s infection. Most of these mutations are single base-pair changes, which can result in a different restriction pattern based on PFGE and AFLP analysis [17].
The increasing popularity of hot tubs in hotels and private homes demands increased awareness about the potential health risks associated with deficient hygienic maintenance. The occurrence of P. aeruginosa pneumonia in the community should always prompt proper environmental investigations in order to elucidate possible sources of infection. Using PFGE, a case of P. aeruginosa urosepsis and prostatitis in a previously healthy 38-year-old was recently linked to contaminated water in the patient’s hot tub; this underlines the considerable potential of today’s molecular subtyping methods as a tool to elucidate sources of infection [18].
The detection of 37,000 CFU of P. aeruginosa in a hot tub indicates massive biofilm formation in the bath circulation and severe deficiencies in hygienic maintenance. P. aeruginosa is able to multiply in biofilms that form on the surfaces of pipes filled with stagnant water, and it can grow at temperatures up to 42°C [1, 18]. There are a number of regulations governing the microbiological quality of water in hot tubs in commercial premises, such as wellness hotels or health spas; however, in Austria this has been regulated by law only since July 2009 [19]. The microbiological requirements are based on the Austrian standard ÖNORM M 6222-1, which stipulates “Requirements for the characteristics of bath water in hot tubs: operations, maintenance and inspection” [20]. This standard requires that the hot tub water circuit system be disinfected during or after each filling to prevent the formation of biofilms. According to this regulation, there must be no E. coli, P. aeruginosa and Legionella spp. in a 100 ml sample of water (taken after 5 min of running idle).
Acknowledgments
We gratefully acknowledge the support received from Sören Gaterman (Bochum, Germany), Hannes Pohla (Salzburg, Austria) and Thomas Holzmann (Regensburg, Germany) in this investigation. We are also indebted to our colleagues who provided clinical P. aeruginosa isolates for comparison.
Conflict of interest
The authors declare that they have no competing interests.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
References
- 1.Pier GB, Ramphal R. Pseudomonas aeruginosa. In: Mandell GL, Bennett JE, Dolin R, editors. Principles and practice of infectious diseases. 7. Philadelphia: Churchill Livingstone Elsevier; 2010. pp. 2835–2860. [Google Scholar]
- 2.Crnich CJ, Gordon B, Andes D. Hot tub-associated necrotizing pneumonia due to Pseudomonas aeruginosa. Clin Infect Dis. 2003;36:55–57. doi: 10.1086/345851. [DOI] [PubMed] [Google Scholar]
- 3.Clinical and Laboratory Standards Institute. Performance standards for antimicrobial disk susceptibility testing. Approved standard M100-S14, 15th edn. Clinical and Laboratory Standards Institute, Wayne, Pa. 2005.
- 4.Johnson JK, Arduino SM, Stine OC, Johnson JA, Harris AD. Multilocus sequence typing compared to pulsed-field gel electrophoresis for molecular typing of Pseudomonas aeruginosa. J Clin Microbiol. 2007;45:3707–3712. doi: 10.1128/JCM.00560-07. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Tenover FC, Arbeit RD, Goering RV, Mickelsen PA, Murray BE, Persing DH, Swaminathan B. Interpreting chromosomal DNA restriction patterns produced by pulsed-field gel electrophoresis: criteria for bacterial strain typing. J Clin Microbiol. 1995;33:2233–2339. doi: 10.1128/jcm.33.9.2233-2239.1995. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Vos P, Hogers R, Bleeker M, Reijans M, van de Lee T, Hornes M, Frijters A, Pot J, Peleman J, Kuiper M, Zabeau M. AFLP: a new technique for DNA fingerprinting. Nucleic Acids Res. 1995;23:4407–4414. doi: 10.1093/nar/23.21.4407. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Van Mansfeld R, Willems R, Brimicombe R, Heijerman H, van Berkhout FT, Wolfs T, van der Ent C, Bonten M. Pseudomonas aeruginosa genotype prevalence in Dutch cystic fibrosis patients and age dependency of colonization by various P. aeruginosa sequence types. J Clin Microbiol. 2009;47:4096–4101. doi: 10.1128/JCM.01462-09. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Jolley KA, Chan M-S, Maiden MCJ. mlstdbNet––distributed multi-locus sequence typing (MLST) databases. BMC Bioinformatics. 2004;5:86–93. doi: 10.1186/1471-2105-5-86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Török ME, Cooke FJ, Moran E. Oxford Handbook of Infectious Diseases and Microbiology. Oxford: Oxford University Press; 2009. pp. 341–342. [Google Scholar]
- 10.Rose HD, Franson TR, Sheth NK, Chusid MJ, Macher AM, Zeirdt CH. Pseudomonas pneumonia associated with use of a home whirlpool spa. JAMA. 1983;250:2027–2029. doi: 10.1001/jama.250.15.2027. [DOI] [PubMed] [Google Scholar]
- 11.Henderson A, Kelly W, Wright M. Fulminant primary Pseudomonas aeruginosa pneumonia and septicaemia in previously well adults. Intensive Care Med. 1992;18:430–432. doi: 10.1007/BF01694348. [DOI] [PubMed] [Google Scholar]
- 12.Hatchette TF, Gupta R, Marrie TJ. Pseudomonas aeruginosa-community-acquired pneumonia in previously healthy adults: case report and review of the literature. Clin Infect Dis. 2000;31:1349–1356. doi: 10.1086/317486. [DOI] [PubMed] [Google Scholar]
- 13.Alan AH, Goodmann L, Stuart L. Community-acquired Pseudomonas aeruginosa pneumonia associated with the use of a home humidifier. West J Med. 1984;141:521–523. [PMC free article] [PubMed] [Google Scholar]
- 14.Berrouane YF, McNutt LA, Buschelman BJ, Rhomberg PR, Sanford MD, Hollis RJ, Pfaller MA, Herwaldt LA. Outbreak of severe Pseudomonas aeruginosa infections caused by a contaminated drain in a whirlpool bathtub. Clin Infect Dis. 2000;31:1331–1337. doi: 10.1086/317501. [DOI] [PubMed] [Google Scholar]
- 15.Fishman H, Eaton B, Lipson A, Delaney MD. Primary Pseudomonas pneumonia in a previously healthy man. South Med J. 1983;76(2):260–262. doi: 10.1097/00007611-198302000-00033. [DOI] [PubMed] [Google Scholar]
- 16.Smith EE, Buckley DG, Wu Z, Saenphimmachak C, Hoffman LR, D’Argenio DA, Miller SI, Ramsey BW, Speert DP, Moskowitz SM, Burns JL, Kaul R, Olson MV. Genetic adaptation by Pseudomonas aeruginosa to the airways of cystic fibrosis patients. Proc Natl Acad Sci USA. 2006;103:8487–8492. doi: 10.1073/pnas.0602138103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Nguyen D, Singh PK. Evolving stealth: genetic adaptation of Pseudomonas aeruginosa during cystic fibrosis infections. Proc Natl Acad Sci USA. 2006;103:8305–8306. doi: 10.1073/pnas.0602526103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Dulabon LM, LaSpina M, Riddell SW, Kiska DL, Cynamon M. Pseudomonas aeruginosa acute prostatitis and urosepsis after sexual relations in a hot tub. J Clin Microbiol. 2009;47:1607–1608. doi: 10.1128/JCM.02376-08. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Austrian Federal Ministry of Health. Bundesgesetz, mit dem das Bäderhygienegesetz geändert wird. Bundesgesetzblatt I Nr. 64/2009. 2009. Available at: http://www.ris.bka.gv.at/Dokumente/BgblAuth/BGBLA_2009_I_64/BGBLA_2009_I_64.pdf.
- 20.Austrian Standards Institute (ASI). Requirements for the characteristics of bath water in whirl tubs: operations, maintenance and inspection. Document ÖNORM M 6222-1. ASI, Vienna, Austria. 2008.