

A 35-year-old man presented to the emergency department with acute-onset nausea, vomiting, diminution of vision and altered sensorium. His family gave history of ingestion of locally made alcohol the previous day. On investigating, the patient had metabolic acidosis. Non-contrast CT head done 6 hours after admission revealed bilateral symmetrical hypodensities in putamen [Figure 1]. MRI was done 4 days after CT scan. Bilateral putamen were swollen and showed hyperintensities on T2W weighted and Fluid attenuated inversion recovery [FLAIR] imaging [Figure 2]. Corresponding lesions were hypointense on T1W images and showed restriction on diffusion imaging [Figure 3]. Small hyperintense foci were also seen in bilateral frontal lobes. Diagnosis of putamen necrosis secondary to methanol ingestion was made.
Figure 1.
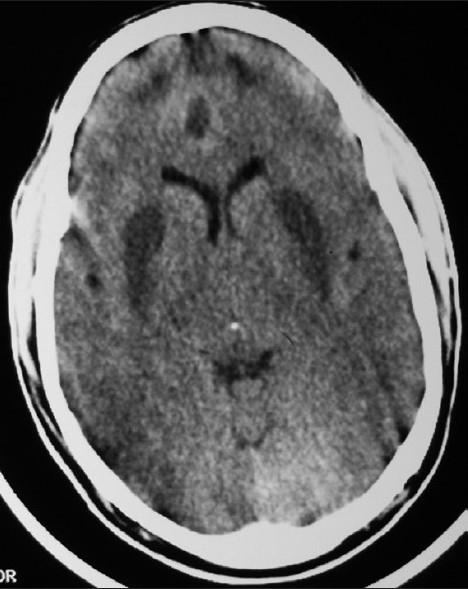
Non-contrast CT (NCCT) head shows bilateral symmetrical hypodensities in the putamen and frontal lobes
Figure 2.
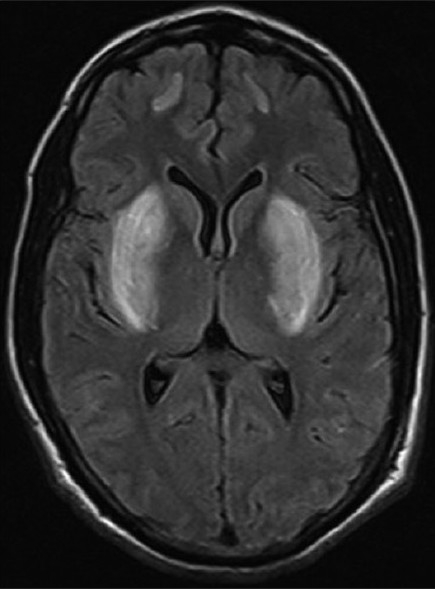
Axial FLAIR image shows bilateral symmetrical putaminal hyperintensities. Also note hyperintense signal involving bilateral frontal lobes
Figure 3.
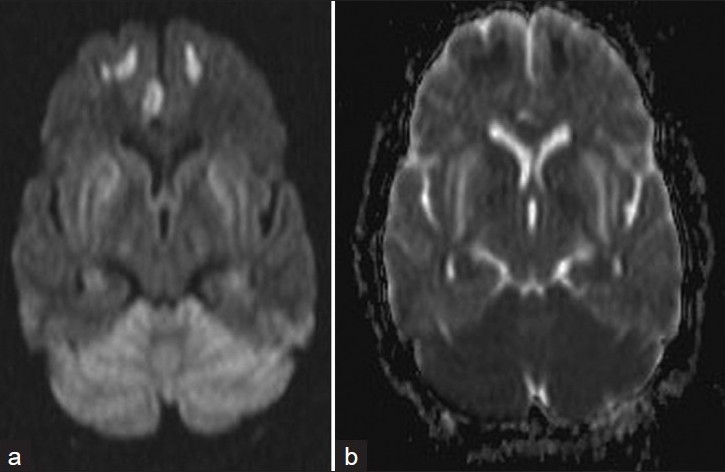
(a) Diffusion weighted images (DWI) and (b) Apparent diffusion coefficient (ADC) images show restriction of the diffusion
Methanol poisoning is an uncommon but potent central nervous system toxin that presents as accidental or suicidal ingestion. Early symptoms of methanol poisoning, except for visual disturbances, are nonspecific and include nausea, vomiting and abdominal pain.[1] Late manifestations are due to acidosis secondary to the accumulation of formic acid and lactic acid (methanol metabolites). The terminal event is often respiratory arrest, and the fatal period is from 6 to 36 hours.[2]
Neuroimaging is characteristic and diagnostic.[3–5] Bilateral necrosis of the basal ganglia is accepted as the most characteristic radiological feature of methanol poisoning. Other brain lesions occasionally described include edema, necrosis of subcortical white and gray matter, cerebellar cortical lesions, subarachnoid hemorrhage, bilateral intracerebral hemorrhage, bilateral tegmental necrosis and diffuse cerebral edema.[3] Carbon monoxide and cyanide intoxications or diffuse hypoxia can result in similar radiological findings and should be considered as differential diagnoses. Putaminal changes may also be seen in Wilson's disease, Leigh disease, Kearns-Sayre syndrome, hypoxic-ischemic injury, trichloroethane poisoning.[4,5] Present case showed the classical clinical and imaging findings in the acute setting.
It has been postulated that the putaminal necrosis results from decreased blood flow through the basal veins of Rosenthal secondary to hypotension. It may also occur as a direct toxic effect of formic acid, with higher concentrations of formic acid accumulating in the putamen than in other areas of the brain, or due to varying sensitivity of striatal neurons to toxic metabolites of methanol.[2]
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Blanco M, Casado R, Vázquez F, Pumar JM. CT and MR imaging findings in methanol intoxication. AJNR Am J Neuroradiol. 2006;27:452–4. [PMC free article] [PubMed] [Google Scholar]
- 2.Liesivuori J, Savolainen H. Methanol and formic acid toxicity: Biochemical mechanism (review) Pharmacol Toxicol. 1991;69:157–63. doi: 10.1111/j.1600-0773.1991.tb01290.x. [DOI] [PubMed] [Google Scholar]
- 3.Sefidbakht S, Rasekhi AR, Kamali K, Borhani Haghighi A, Salooti A, Meshksar A, et al. Methanol poisoning: Acute MR and CT findings in nine patients. Neuroradiology. 2007;49:427–35. doi: 10.1007/s00234-007-0210-8. [DOI] [PubMed] [Google Scholar]
- 4.Taheri MS, Moghaddam HH, Moharamzad Y, Dadgari S, Nahvi V. The value of brain CT findings in acute methanol toxicity. Eur J Radiol. 2010;73:211–4. doi: 10.1016/j.ejrad.2008.11.006. [DOI] [PubMed] [Google Scholar]
- 5.Bessell-Browne RJ, Bynevelt M. Two cases of methanol poisoning: CT and MRI features. Australas Radiol. 2007;51:175–8. doi: 10.1111/j.1440-1673.2007.01691.x. [DOI] [PubMed] [Google Scholar]