

Abstract
Hepatitis C virus (HCV) infection is relatively common among patients with end-stage kidney disease (ESKD) on dialysis and kidney transplant recipients. HCV infection in hemodialysis patients is associated with an increased mortality due to liver cirrhosis and hepatocellular carcinoma. The severity of hepatitis C-related liver disease in kidney transplant candidates may predict patient and graft survival after transplant. Liver biopsy remains the gold standard in the assessment of liver fibrosis in this setting. Kidney transplantation, not haemodialysis, seems to be the best treatment for HCV+ve patients with ESKD. Transplantation of kidneys from HCV+ve donors restricted to HCV+ve recipients is safe and associated with a reduction in the waiting time. Simultaneous kidney/liver transplantation (SKL) should be considered for kidney transplant candidates with HCV-related decompensated cirrhosis. Treatment of HCV is more complex in hemodialysis patients, whereas treatment of HCV recurrence in SLK recipients appears effective and safe.
1. Introduction
Hepatitis C is one of the commonest chronic viral infections world-wide and has major healthcare and health economic implications [1] (Figure 1). However, with recent advances in treatment, clearance of the virus is achieved in selected cases and a reduction in the rate of progression of liver disease and its complications occurs in others. Kidney disease is a major public health problem; over 10% of the adult population has chronic kidney disease (CKD) [2], and up to 350 pmp/yr of the adult population develop ESKD and require treatment with renal replacement therapy (RRT) by dialysis or transplantation. The prevalence of HCV infection in people with ESKD is very high, and when present has implications both for dialysis patients and for kidney transplant (KT) recipients [3, 4].
Figure 1.
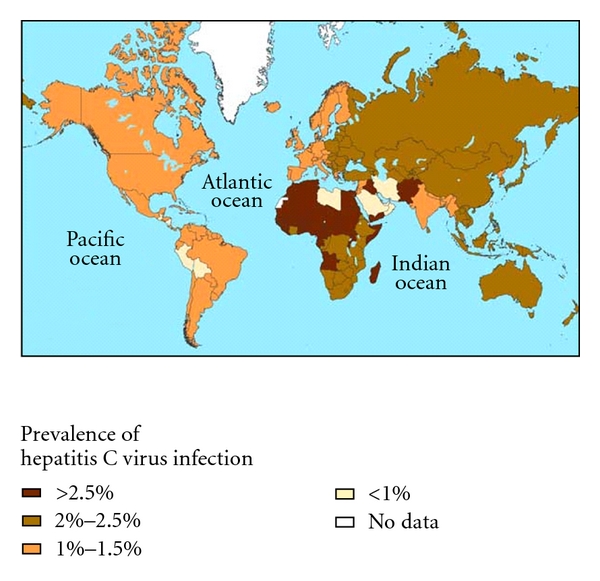
Prevalence of Hepatitis C Infection. Data source: World Health Organization. (Modified from [5].)
HCV infection is challenging both in dialysis patients and KT recipients, but there are differences between these two groups in terms of the effect of HCV infection on long-term survival, the natural history of the disease, and differential benefits and risks associated with available treatments both of the HCV and the renal failure. As kidney transplantation is the treatment of choice for many people with ESKD, the clinical assessment and the management of HCV infection are important clinical considerations in this setting.
In this paper, we report the current status of HCV infection and kidney transplantation. After a brief presentation of the natural history of hepatitis C virus infection in immunocompetent host, we assess: (i) HCV infection in end-stage kidney disease (ii) the impact of HCV on clinical outcomes (iii) the assessment of the disease and (iv) the disease management of HCV+ve kidney transplant recipients.
2. Natural History of Hepatitis C Virus (HCV) Infection
The worldwide burden of chronic hepatitis C (CHC) infection is enormous. In 1999, the World Health Organization estimated that the worldwide prevalence of CHC ranges from 0.1% to more than 12%. This equates to approximately 170 million chronic carriers worldwide with an incidence of 3 to 4 million new cases annually [6].
After initial exposure, HCV RNA can be detected in blood within 1 to 3 weeks. Acute infection is usually asymptomatic; it can be severe but rarely fulminant. In general, 60 to 85% of HCV-infected persons develop chronic infection, defined as the continued presence of HCV RNA for 6 months or longer after the estimated onset [7].
The spectrum of the disease ranges from mild to severe chronic hepatitis, cirrhosis, and hepatocellular carcinoma. The disease is complex, and predictions about long-term prognosis for individual patients remain difficult. Hepatitis C can be extremely slow to progress and usually does so without liver-specific symptoms or physical signs during the first decade of infection. Estimates of the proportion of chronically infected persons who develop cirrhosis 20 years after initial infection vary from 10 to 15% [7]. When liver cirrhosis is established, the transition to decompensated cirrhosis occurs when complications secondary to liver failure arise, such as jaundice, variceal hemorrhage, ascites, and encephalopathy. Decompensated cirrhosis is associated with increased risk of mortality and necessitates liver transplantation.
Identifying the group of patients at greatest risk of fibrosis progression remains a primary challenge for clinicians. Older age at time of infection, duration of infection, degree of liver inflammation at first biopsy, and cofactors such as alcohol abuse and coinfection with human immunodeficiency virus (HIV) or hepatitis B virus (HBV) all appear to be predictors of a poorer prognosis.
The most reliable tools for examining the natural history of hepatitis C are those which examine a change in the histopathological status. Although this necessitates repeated liver biopsies, it does enable the physician, within the space of a few years, to examine possible disease progression or lack of it. The typical histological features of chronic hepatitis C are variable degrees of hepatocellular necrosis and inflammation, referred to as the activity or grade of disease, and fibrosis, referred to as stage of disease.
While the activity of the liver disease can fluctuate, fibrosis is believed to be progressive and largely irreversible. Importantly, it is the progression of fibrosis that ultimately leads to architectural distortion of the liver and cirrhosis. For these reasons, the rate of progression of fibrosis is the defining feature of the natural history of chronic hepatitis C.
Several systems for scoring liver fibrosis have been proposed, each based on visual assessment of collagen staining of liver biopsy samples, and the more frequently used systems are the histology activity index (HAI: Knodell score) [8, 9] and the Metavir system [10].
In 2001, Poynard reported that the median estimated duration of infection for progression to cirrhosis was 30 years, ranging from 13 years in men who drank and were infected after the age of 40 to 42 years in women who did not drink alcohol and were infected before the age of 40 [11]. This average rate of progression of fibrosis is consistent with those reported in more recent studies [12–14]. It should be highlighted, however, that these studies were performed in referral centers, and the patients who were studied may not have been representative of the average patient with chronic hepatitis C.
3. HCV Infection in End-Stage Kidney Disease (ESKD): Prevalence and Impact on Survival
Hepatitis C virus (HCV) infection is very common in patients with ESKD [15]. The reported prevalence in hemodialysis (HD) patients is variable, but is considerably greater than in the general population. There are some indications that the overall prevalence of HCV infection in dialysis patients is falling, as reported by data from the USA, Western Europe, and Australia and New Zealand [3, 16–19].
Information on the incidence and prevalence of HCV infection in patients on long-term dialysis in developing countries is limited, but single-center surveys show that these rates are high [20–22]. This probably reflects nosocomial transmission of HCV in the HD environment, incomplete anti-HCV screening of blood and blood products, and a higher prevalence of HCV in the general population in developing countries.
Irrespective of the baseline prevalence in the general population, the key underlying determinants of an increased relative risk of HCV infection in dialysis patients are age, overall exposure to blood products, and the duration of dialysis treatment [15–17]. Therefore, the widespread use of erythropoeisis-stimulating agents (ESAs) with a consequent decrease in blood transfusions and progressive improvements in infection control on dialysis units are likely major contributors to a decreasing prevalence of HCV infections in HD patients in the developed world.
In those patients who undergo renal transplantation, in developed countries, the reported prevalence of HCV infection is usually higher than that seen in HD patients, ranging from 11% to 49% [23–30].
Where there are differences reported in HCV infection prevalence between dialysis patients and KT recipients, the reasons may include the length of time on dialysis before transplantation, the duration of the dialysis that the transplant recipient received, and a history of and/or the number of blood transfusions. As transplant recipients usually survive longer than patients who remain on dialysis, a higher proportion of transplant recipients may have been exposed as a consequence of receiving blood products or dialysis in a period of less rigorous infection control.
HCV infection has been independently associated with an increased mortality in maintenance HD patients. The DOPPS (Dialysis Outcomes and Practice Patterns) study, conducted over three continents, showed an independent association between positive anti-HCV antibody status and mortality in dialysis patients [4]. These results have been confirmed in other studies [31–33].
Scott et al. (the ANZDATA registry study) [3] reported similar survival at 5 years (48% versus 47%) and 10 years (22% and 20%) for HCVAb+ve and HCVAb−ve patients, however, when the differential age distribution and other patient characteristics were incorporated, the adjusted hazard ratio (aHR) for mortality was increased in the HCVAb+ve population Table 1.
Table 1.
Summary Estimates for Adjusted Relative Risk of Mortality among HCV+ve Dialysis Patients.
4. Outcome of Renal Transplantation in HCV+ Patients
Kidney transplantation (KT) is associated with improved long-term survival in the ESRD population [37], and whilst there is evidence in some studies of a detrimental impact of HCV infection on the outcome of KT, the survival of HCV infected recipients is excellent when considered against that those of HCV infected patients who remain on dialysis [38, 39].
Initial studies focused on short-term outcomes and showed similar patient and graft survival in HCV+ and HCV− recipients at 5 years [27, 40–42], and a low prevalence of cirrhosis HCV-related even after 10 years post-KT [43]. Similar findings were reported by Einollahi et al. in 2002, who showed no differences in terms of survival between HCV+ve and HCV−ve recipients at 7 years post-KT [44].
These findings could reflect the comparatively short period of followup as well as the low numbers of patients as some studies have indicated that the difference in survival was significant only in the second decade after transplantation [45].
These single studies were pooled by Fabrizi et al. in a meta-analysis [46], which showed that positive anti-HCV antibody status was an independent and significant risk factor for death and graft failure after renal transplantation; the summary estimate for the relative risk was 1.79 (95% CI, 1.57; 2.03) and 1.56 (95% CI, 1.35; 1.80), respectively (Table 2).
Table 2.
Death rate in HCV+ve versus HCV−ve patients after Kidney Transplantation.
| Year of publication | Followup after KT in months (mean)* | HCV-positive Death | HCV-negative Death | P-value | |
|---|---|---|---|---|---|
| Pereira et al. [23] | 1995 | 68/70 | 11/29 (38%) | 26/72 (36%) | n.s. |
| Pereira et al. [47] | 1995 | 68/83 | 9/22 (41%) | 16/78 (20.5%) | n.s. |
| Legendre et al. [48] | 1998 | 79/81 | 15/112 (13.4%) | 19/387 (5%) | .01 |
| Gentil et al. [49] | 1999 | 62/57 | 13/85 (15.3%) | 11/235 (4.7%) | .003 |
| Lee et al. [50] | 2001 | 72 | 31/151 (20.5%) | 46/326 (14%) | n.s. |
| Breitenfeldt et al. [51] | 2002 | 110.4 | 38/130 (29%) | 164/797 (20.6%) | .001 |
| Einollahi et al. [44] | 2003 | n.a. | 2/41 (5%) | 34/868 (4%) | .74 |
| Bruchfeld et al. [52] | 2004 | 130 | 29/51 (57%) | 170/520 (32.7%) | .001 |
| Scott et al. [3] | 2010 | 62.4 | 32/140 (23%) | 743/7432 (10%) | .0001 |
*Data are given for anti-HCV+ve/anti-HCV−ve patients when appropriate.
n.a.: not available; n.s.: not statistically significant.
In their recent study, Scott and colleagues [3] evidenced a prevalence of HCV infection among kidney transplant recipients of 1.8%, and found that patient survival among HCVAb+ve and HCVAb−ve groups was 77% versus 90% and 50% versus 79% at 5 and 10 years, respectively, with an adjusted HR for patient death of 2.38 (95%CI, 1.69–3.37).The most common causes of death among the HCVAb+ve kidney recipients were cardiovascular disease (aHR = 2.74), malignancy (aHR = 2.52), and hepatic failure (aHR = 22.1).
Despite the negative impact of HCV infection on long-term survival after KT, three retrospective studies [34, 39, 53] of HCV-infected patients have demonstrated that survival is improved with transplantation compared to the remaining wait-listed on dialysis in HCV-infected patients with kidney failure. There are no published studies demonstrating a worse outcome with transplantation compared to dialysis for these patients. Therefore, it is recommended that HCV infection should not be considered a contraindication to KT [54].
While mortality is the most significant end-point in the natural history of HCV after KT, other outcomes have also been assessed in HCV-infected KT recipients with variable conclusions. In a case-control, retrospective survey, Zylberberg et al. [55] found that the yearly progression rate of hepatic inflammation and fibrosis was significantly higher in the KT recipients as compared with the immunocompetent group. In contrast, Alric et al. [56] found that the progression of liver fibrosis per year was significantly lower for KT recipients than for matched patients with HCV and normal renal function. Reasons for the differences are not clear.
4.1. De Novo Glomerulonephritis and Chronic Allograft Nephropathy after Kidney Transplant in HCV+ve Recipient
In addition to an increased disease burden due to liver disease and an association with all-cause and cardiovascular disease mortality, HCV infection in kidney transplant recipients has been implicated in the pathogenesis of acute glomerulopathy [57], de novo immune complex glomerulonephritis in the allograft [58–60], and, in some reports, a higher rate of chronic allograft nephropathy (CAN) [61].
HCV infection is one of the most important factors predisposing to the development of glomerulonephritis (GN) in the native kidney and in the renal allograft [62] and the high prevalence of HCV infection in renal allograft recipients places this group at high risk of immune-mediated glomerular diseases. In de novo membranoproliferative glomerulonephritis (MPGN) and de novo membranous glomerulopathy (MGN), with or without mixed cryoglobulinemia, are the most most frequent glomerular lesion associated with chronic HCV infection in renal allografts [58, 60, 63].
In 2001, Cruzado et al. [64] reported a prevalence of de novo MPGN and MGN in HCV+ve kidney recipients of 45.4% and 18.2%, respectively, versus a lower rate in HCV−ve recipients of 5.7% and 7.7%, respectively. These data have been confirmed in 2006 by Ozdemir et al. [59] who reported a prevalence of de novo GN in HCV-infected recipients of 34%, compared to 6.6% in HCV−ve recipients. In both studies, this higher prevalence of autoimmune GN was associated with a poor graft outcome, even worse than de novo GN in HCV−ve.
HCV infection has also been associated with CAN. This was first suggested in 2005 by Mahmoud who reported a higher rate of CAN in patients HCV+ve who had not received interferon therapy before KT, compared with a population of HCV+ve patients who received IFN for the treatment of HCV infection (with a 100% of biochemical response and 55% of clearance of the virus), after controlling for other biases that may contribute to the development of CAN [61]. Recently, the analysis of the ANZDATA has shown an increased rates of graft failure due to chronic allograft nephropathy (aHR = 1.87) in HCV+ve recipients compared to HCV−ve patients [3]; also, the analysis of 4304 renal transplant recipients (with 587 of them HCV+ve) in the period 1990–2002, performed by the Spanish Chronic Allograft Nephropathy Study Group [65], evidenced HCV infection was associated with early greater rates of proteinuria, lower renal function, chronic rejection, de novo GN, graft loss, and lower survival, compared with HCV−ve recipients.
The pathogenesis of CAN could be explained by a multitude of alloantigen-dependent and -independent factors which have been extensively reviewed [66–68].
It has been proposed that a higher incidence of acute rejection due to higher viral-induced immune reactivity according to previous studies [27] and a chronic suboptimal immunosuppression might be a possible explanation for the relationship between HCV infection and CAN. However, this association has not been confirmed in other studies [69].
HCV infection has also been associated with the development of early graft dysfunction due to acute glomerular lesions, such as acute transplant glomerulopathy and de novo renal thrombotic microangiopathy [57, 70]. Hepatitis C infection has also been linked to an increased incidence of posttransplant diabetes mellitus (PTDM) [71], which is an important determinant of worse outcome following transplantation.
4.2. HCV Replication and Immunosuppression Regimen after Kidney Transplant
Levels of viremia after transplantation are higher compared to pretransplantation values [72]. The marked increase in serum HCV-RNA levels, which usually develops within the first months after renal and liver transplantation, has been closely associated with the immunosuppressive therapy, and a more aggressive immunosuppression enhances HCV replication [73], although the relationship between posttransplantation viral kinetics and severity of recurrence of HCV remains unclear.
Pelletier in 2000 found no correlation between HCV-RNA blood levels and the intrahepatic viral replication rate in the posttransplant period [74], suggesting that the elevated levels of serum HCV-RNA typically observed posttransplantation are not a result of increased replication but rather of decreased clearance in the setting of immune suppression [75].
Di Martino et al. [76] evidenced a progression to chronic active hepatitis after liver transplantation, despite a reduction in immunosuppression and a decrease of intrahepatic HCV-RNA levels, suggesting an immune-mediated injury behind the liver damage, although there are reports of an association between high levels of viral replication and a rapid progressive histologic course suggesting a cytopathic mechanism of HCV-induced allograft injury [77–80]. High levels of viremia have been described in the setting of fibrosing cholestatic hepatitis (FCH) after liver transplantation [81], suggesting that during the early phase of recurrent hepatitis C or in the setting of this particular syndrome, liver damage may be due to the direct cytopathic effect of HCV. Fibrosing cholestatic hepatitis has been sporadically described in kidney transplant recipients with a severe, and often fatal, course [82–85].
At the present time, there are relatively few studies that examine the impact of immunosuppression on HCV-related outcomes in kidney transplant patients, and it is not clear whether the impact of immunosuppression on outcomes in liver transplant patients with HCV infection can be extrapolated to HCV-infected kidney transplant recipients. Therefore, all currently available maintenance immunosuppressive therapies can be used in kidney transplant recipients with HCV infection [54].
Cyclosporin, but not tacrolimus may inhibit HCV viral replication, although whether this has any clinical consequences is not validated in kidney transplant patients. However, a recent report of 71 HCV+ve KT recipients [86] showed, during long-term immunosuppression, cyclosporine when compared with tacrolimus, resulted in no significant differences in viral replication and development of liver fibrosis. However, the function of the renal graft was significantly better preserved in patients receiving tacrolimus.
Mycophenolate mofetil (MMF) has shown to have an inhibitory effect on viral replication in the nontransplant setting [87] and there is no convincing evidence of a specific deleterious effect on either graft or patient outcomes in kidney transplant recipients with HCV infection [88, 89].
Among antibody therapies commonly used for induction or for treating acute rejection, unfavorable outcomes have been frequently reported in the literature concerning liver transplant patients with HCV infection. In contrast, recent registry data of 3708 patients from the United States indicate that antibody induction with the use of a biological agent, either depleting (OKT3, ATGAM, or rabbit thymoglobulin) or nondepleting antibodies (IL-2 R blocking antibodies), did not negatively affect patient survival in HCV-infected kidney transplant recipients [90].
Regarding the use of sirolimus in HCV-infected kidney transplant recipients, there are only limited data.
5. Assessment of Liver Fibrosis in HCV+ Renal Transplant Candidates
There is evidence that the severity of hepatitis C-related liver disease may predict worse patient and graft survival [91, 92] after KT. The most accurate method to assess liver inflammation and fibrosis is with liver histology, using the Knodell score [8]. Single-center retrospective cross-sectional studies have reported that up to 25% of HCV-infected patients being evaluated for kidney transplantation have bridging fibrosis or cirrhosis on biopsy [93–98]. Some investigators have suggested that presence of advanced fibrosis (bridging fibrosis or cirrhosis) should preclude kidney transplantation [99, 100]. However, we feel that currently there are insufficient data to support such a recommendation.
Recently, the accuracy of liver biopsy in staging liver disease has been a focus of discussion. Because a biopsy represents 1/50,000 of the liver, the heterogeneity of liver fibrosis in HCV infection and the inadequacy of liver sample size can cause considerable bias in the assessment of liver histology [100–102]. Also, liver biopsy is associated with clinical risks.
Currently, a variety of noninvasive tests may be used to estimate liver fibrosis in HCV patients with normal renal function, using either individual markers (such as procollagen) or a panel of tests, such as the Enhanced Liver Fibrosis (ELF) that includes hyaluronic acid, tissue inhibitor of matrix metalloproteinases-1, aminoterminal propeptide of procollagen type III (which are involved in the synthesis and degradation of extracellular matrix) [103], and present the advantage of providing frequent fibrosis evaluation. However, few data are available regarding the utility of those tests in ESRD patients with HCV chronic infection (Table 3).
Table 3.
Predictive value of serological markers for advanced liver fibrosis in HCV+ patients with end-stage renal disease.
| Components of the test | Cutoffs | Authors | Sample Size | AUROC | PPV | NPV | |
|---|---|---|---|---|---|---|---|
| APRI | AST-to-Platelets-Ratio | <0.4 = no advanced fibrosis >0.9 = advanced fibrosis |
Schiavon et al. [103] | 203 | 0.8 | 66% | 93% |
| Liu et al. [104] | 279 | 0.83 | 85% | 82% | |||
| Schiavon et al. [105] | 185 | 0.78 | 66% | 93% | |||
| Fibrotest | α2 macroglobulin, haptoglobin, γ-glutamyl transpeptidase, total bilirubin and apolipoprotein A1 levels | <0.2 = no advanced fibrosis >0.6 = advanced fibrosis |
Varaut et al. [106] | 50 | 0.47 | 71% | 77% |
| Canabakan et al. [107] | 33 | 0.46 | 20% | 45% | |||
| Hyaluronic Acid | Unbranched, high-molecular weight polysaccharide that is widely distributed in the extracellular spaces | <64 = no advanced fibrosis >205 = advanced fibrosis |
Schiavon et al.[105] | 185 | 0.65 | 42% | 86% |
| YKL-40 | Glycoprotein with function in the remodelling of the extracellular matrix or in tissue inflammation | <290 = no advanced fibrosis >520 = advanced fibrosis |
Schiavon et al. [105] | 185 | 0.6 | 35% | 84% |
The AST/ALT ratio was studied as a noninvasive marker of liver fibrosis in 49 ESRD patients with HCV infection. Despite the significant differences in AST/ALT ratio found between different fibrosis stages, the usefulness of this index may be limited by the absence of adjusted cutoffs in ESRD patients where lower aminotransferase activity is expected. The lack of association between AST/ALT ratio and the degree of liver fibrosis has been also confirmed in a more recent study [103, 108].
The FibroTest, a composite marker of fibrosis, has been evaluated in both HD patients and KT recipients with HCV infection, but its reliability in this setting is controversial [106, 107].
APRI (AST-to-platelets ration index) with adjusted cutoffs has been proposed as a valid alternative to liver biopsy in a significant proportion of HCV+ HD patients [103, 104] although further large studies are needed to confirm these findings.
Others markers of liver fibrosis have also been evaluated in patients with chronic hepatitis C, including YKL-40 and hyaluronic acid (HA), but the performance of these tests was lower than that observed for others noninvasive markers previously evaluated such as APRI [105].
Transient elastography (TE, FibroScan) is a novel noninvasive technique that has been validated in patients with chronic hepatitis C for the assessment of hepatic fibrosis, by measuring liver stiffness. Although it has not been validated yet in CKD patients with HCV infection, it may represent a new and noninvasive tool to assess the stage of liver disease in this setting.
In conclusion, liver biopsy represents the gold-standard in the assessment of liver fibrosis in HCV+ patients with ESKD and might be considered part of the pretransplant evaluation for HCV+ patients; despite the increased role of noninvasive tests for the evaluation of liver fibrosis in HCV-infected patients with CKD, this requires further study.
5.1. Kidney or Liver and Kidney Transplantation?
Should patients found to have advanced fibrosis or cirrhosis be excluded from kidney transplantation alone? This is a key question as the mortality in HCV+ patients with advanced kidney disease is more commonly related to other comorbidities than liver disease both pre- and posttransplantation [39, 109]. The data in this area are conflicting.
The presence of compensated liver cirrhosis before kidney transplantation has the potential to increase the risk of recipient mortality in terms of operative procedure because of marginal posttransplant reserve and nutritional state, and increased susceptibility to post-transplant infectious and metabolic complications, as well as evolution to decompensated liver disease and the subsequent need for a liver transplant.
There are no data available to determine whether patients with early cirrhosis on liver biopsy but well-compensated clinical disease do better if they are transplanted or remain on dialysis.
In 2006, Campbell et al. [109] evaluated the association between advanced liver fibrosis and survival among HCV+ patients evaluated for KT.
Among 108 HCV+ patients, eighteen (6%) had advanced fibrosis (bridging fibrosis or cirrhosis) before KT. Fifty-eight patients subsequently underwent KT, and 10 of these had advanced fibrosis. Rates of transplantation were similar between those with advanced fibrosis (56%) and those without (53%; P = .1). Survival was similar in those with and without advanced fibrosis both among all patients (P = .92) and among those patients who underwent kidney transplantation (P = .83); nonliver disease comorbidities seemed to be the most important outcome determinants in this population.
In 2007, Maluf et al. [38], analyzing forty-three HCV+ KT recipients, identified Knodell score >6 in the pre-KT biopsies (without mentioning if it was prevalently related to inflammation or fibrosis) as a predictor of mortality after KT in HCV+ve patients and, therefore, raised concerns about the benefits of KTx in this group of patients, although prospective studies are necessary to confirm these findings.
There are very limited outcome data regarding transplantation of a kidney alone in HCV-infected recipients with pre-existing compensated cirrhosis of the liver; therefore, the KDIGO (Kidney Disease: Improving Global Outcomes) clinical guidelines 2008 recommends that HCV-infected kidney transplant candidates with compensated liver cirrhosis on biopsy only be considered for kidney transplantation under investigational protocol. HCV-infected patients with evidence of decompensated liver disease should be evaluated for simultaneous kidney liver transplantation [54].
6. Use of Kidney Allografts from Anti-HCV+ Donors
Shortly after the introduction of the first-generation anti-HCV tests, studies conducted at the New England Organ Bank unequivocally demonstrated that HCV could be transmitted by organ transplantation [110–112]. This may occur as a new infection in a previously uninfected recipient or superinfection with a different genotype in an HCV-infected recipient [113] Studies conducted in the 1980–1990s evidenced as, among recipients of organs from anti-HCV+ve donors, 35% (range 0–55%) developed posttransplant liver disease, 50% (14–100%) became anti-HCV+ve after transplantation, and 73% (14–96%) developed HCV viremia [111, 112]. The wide variations in the rate of transmission of HCV infection by anti-HCV+ve donors reported by different centers could be due to several factors, such as failure to test recipients at some centers, different prevalence of HCV infection among donors, and differences in organ preservation; the use of pulsatile pump perfusion may reduce the viral load in the donor kidney and seems to have the potential to reduce viral transmission from HCV-infected organs [114]. The extrapolated prevalence of anti-HCV among cadaver organs by ELISA-2 was calculated to be 4.2% and that of HCV-RNA to be 2.4% [112]. This seems to be higher than the prevalence of anti-HCV among healthy blood donors, and it could reflect the higher prevalence of risk factors, among cadaver organ donors, associated with the spread of viral infections, such as unsuspected intravenous drug use or sexual promiscuity.
The high prevalence of HCV among dialysis patients awaiting KT and the shortage of cadaveric kidneys led some groups to evaluate efficacy and safety of using kidneys from HCV+ donors in recipients infected with HCV [115, 116].
A large registry analysis in 2002 demonstrated that use of grafts from HCV+ donors was associated with an increased mortality, regardless of the anti-HCV antibody status of the recipient [117]. However, the use of kidneys from anti-HCV+ deceased donors in HCV+ recipients has been associated with superior patient survival compared with dialysis [118]. Also, Maluf et al. [119], using the Organ Procurement and Transplantation Network (OPTN) database, reported a shortened waiting time of nearly 300 days for HCV+ve recipients received a graft from HCV+ donors compared with HCV−ve recipients, though this was balanced by a significantly decreased patient and graft survival. It is unknown whether the survival reduction was due to other donor factors, a direct effect of the virus on the kidney itself, or related to superinfection with competing viral strains.
A larger analysis of the same OPTN database recently performed by Northup et al. [120], including 19 496 HCV+ve recipients and 934 HCV+ve donors, showed that the adjusted hazard ratio for death was similar for HCV+ recipient/HCV− donor compared with HCV+ recipient/HCV+ donor (1.176 versus 1.165, P = .91); the worst survival was in the HCV− recipient/HCV+ donor group (55.1%).
Use of organs from HCV+ donors has been associated with severe acute hepatitis in HCV-ve recipients (fulminant or fibrosing cholestatic hepatitis), perhaps related to acute infection under maximal immunosuppression [121–123], increased prevalence of chronic liver disease, and worse survival [35, 124–126]; therefore, transplantation of kidneys from HCV+ donors should be restricted to recipients who have a HCV viremia at the time of transplant.
The potential risks of superinfection with an HCV donor genotype different from that of the recipient is unknown. Genotype 1 is the most common genotype of hepatitis C virus in the western countries in both patient with and without ESRD, and it is known to be less responsive to the antiviral therapy with Peg-interferon plus Ribavirin. Genotype superinfection through transplantation has been reported in a few cases, and an increase in transaminase levels was observed [127–130]. Some authors argued that genotyping should be routine, and that HCV genotype 1 kidneys should not be used in patients with other genotypes. However, data do not exist for this strategy beyond anecdotal reports, recommendations, and case reports.
In conclusion, these data provide strong evidence that access to this “extra” pool of organs may confer a waiting time advantage in the HCV-positive population, but the conflicting data on graft and patient survival in this group requires further thought.
7. Therapy of Chronic Hepatitis C in the Chronic Kidney Disease Population
In those without kidney disease, the current standard of care for the treatment of HCV infection is with pegylated interferon and ribavirin. The response is dependent on many factors, including HCV genotype, HCV viral load, age and gender, degree of liver impairment, and duration of therapy. Treatment is limited by many factors, especially toxicity. New agents, such as protease inhibitors, are in clinical development and early studies suggest that these will revolutionize the treatment of HCV infection. Thus, for some patients with histologically early liver disease and little inflammatory activity, delay of therapy may be appropriate.
Despite the increased prevalence of HCV infection in CKD patients compared to that of the general population, the indications for treatment and optimal antiviral regimens in terms of safety and efficacy in CKD are not well defined. Also, all major RCTs for the treatment of HCV infection have specifically excluded patients with abnormal kidney function. A variety of IFN-based regimens with differing treatment durations have been used in CKD, which makes comparison among studies more difficult. The KDIGO Clinical Practice Guidelines 2008 on “Treatment of HCV infection in patients with CKD” were based on the best available information from the CKD population together with data from the general population, where extrapolation was considered to be appropriate.
The decision to treat HCV infection in the CKD patient should be based on liver histology, age, comorbidities, ability to tolerate therapy, probability of achieve a sustained viral response (SVR), life expectancy, and candidacy for kidney transplantation [54].
Potential benefits of successful therapy include slowing the progression of liver disease and reducing the risk of posttransplant complications associated with HCV. However, given the generally indolent progression of HCV, treatment is not recommended for the patient with less than a 5-year estimated survival due to comorbidities such as cardiovascular disease. In some patients, such as in the pretransplant patient or in the patients with HCV-associated GN with or without cryoglobulinemia, there are good data to support treatment. For patients with HCV infection and CKD Stages 1–4, it might be reasonable to adapt the recommendations for treatment that apply to the general population, as there are no studies available that target this specific population [54]. Considering that HCV infection after kidney transplantation is implicated in the pathogenesis of acute glomerulopathy, de novo graft HCV-associated GN, diabetes mellitus, and the higher incidence of CAN, the strength of the recommendation to treat HCV+ve kidney transplant candidate is greater than in the general HCV+ve population on HD; moreover, in this setting antiviral therapy is recommended even for those with a pattern of histologic injury that does not meet the recommended degree of fibrosis to qualify for therapy in the general population (that is, Metavir score <2 and Ishak score <3). In patients with well-compensated cirrhosis, the decision of whether to treat is difficult, and the benefit of treatment in this setting is difficult to measure.
Conventional IFN monotherapy in dialysis patients with chronic hepatitis C is associated with dismal results [61, 131–136]. Two separate meta-analyses analyzing HCV+ patients on hemodialysis showed SVR rates of 33% to 37% with standard IFN-alpha with drop-out rates of 17% to 30% [137, 138].
The combination of Pegylated IFN (PEG-IFN) and ribavirin (RBV) in chronic HCV patients with normal kidney function gives reported SVR rates of 54% to 61% [139].
Few, studies have evaluated combined therapy in HD patients and the quality of this evidence is very low [140–147]. Patients with renal dysfunction are particularly vulnerable to the tolerability issues associated with therapy with PEG-IFN α plus ribavirin. The elimination rate of ribavirin in patients with impaired renal function is reduced, and only a small fraction of the drug is eliminated by hemodialysis. In patients with creatinine clearance between 10–30 mL/minute and 30–60 mL/minute, the AUC for ribavirin is threefold and twofold greater, respectively, than for patients with CrCl > 90 mL/minute. As a result of this increase in drug exposure and the accompanying elevated risk for drug-related toxicity, for example, severe hemolytic anemia, ribavirin is contraindicated in patients with CrCl < 50 mL/minute [148–150].
The use of PEG-IFN monotherapy in patients with ESRD, compared with traditional IFN, is more convenient with once a week dosing, but only small studies have been published to date [36, 151–160].
There is no significant difference in apparent body clearance of PEG-IFN α-2a between patients with normal kidney function and those with significant reductions in kidney function (creatinine clearance >100 mL/min versus 20–40 mL/min (CKD 3b/4)) [161]. However, with ESKD patients receiving HD, the pharmacokinetics of pegylated interferon α-2a may vary reflecting differences in dialyzer permeability and pore size [162]. Recently Fabrizi et al. [163] attempted a systematic review of the literature with a meta-analysis of clinical trials performed to assess efficacy and safety of PEG-IFN monotherapy in CKD patients with chronic hepatitis C. They analyzed 16 clinical trials (5 controlled studies) with a total of 254 patients. The results showed that SVR was achieved by around one-third of patients on HD, the same response seen with standard IFN monotherapy. However, the viral response to monotherapy with standard or pegylated IFN in maintenance HD patients remains higher than that observed in patients with chronic hepatitis C virus and normal kidney function (7–29%) who received standard IFN monotherapy [164]. There may be several reasons for this including: low HCV viral load in HD patients [165] reduced clearance of IFN in HD patients [166] and the observation that HCV-related chronic hepatitis in HD patients is usually milder [167]. The data reported in this meta-analysis are limited by heterogeneity between studies and the small numbers in each study population. Furthermore, the applicability of these results to clinical practice is uncertain because patients included in these studies were on the waiting list for renal transplantation and were younger and probably healthier than the general dialysis population.
More encouraging results regarding the effectiveness of PEG-IFN come from the recent single-center report by Werner et al. [168] who showed a SVR of 45% among a population of 22 naïve HCV patients on HD listed for KT, but confirmation with larger samples is required (Table 4).
Table 4.
Clinical trials of monotherapy with conventional IFN or pegylated IFN in hemodialysis patients with chronic hepatitis C.
| Period | Patients number | Antiviral Agent | Doses of IFN or Peg-IFN | SVR | |
|---|---|---|---|---|---|
| Degos et al. [132] | 2001 | 37 | IFN α | 3 MU three times weekly | 19% |
| Mukherjee et al. [152] | 2003 | 9 | Peg-IFN-α2b | 1 mcg/kg/week | 22% |
| Ozdemir et al. [133] | 2004 | 20 | IFN α | 3–6 MU three times weekly | 40% |
| Rivera et al. [134] | 2005 | 27 | IFN α (n = 20) Peg-IFN-α2a (n = 7) |
3 MU three times weekly 135 mcg/week |
40% |
| Mahmoud et al. [61] | 2005 | 18 | IFN α | 3 MU three times weekly | 44% |
| Grgurevic et al. [135] | 2006 | 15 | IFN α | 3 × 3 MU/week (n = 8) 3 × 5 MU/week for 3 months, then 1 × 5 MU/week for another 3 months (n = 7) |
40% |
| Rocha et al. [136] | 2006 | 46 | IFN α | 3 MU three times weekly | 22% |
| Sporea et al. [153] | 2006 | 10 | Peg-IFN-α2a | 180 mcg/week | 30% |
| Russo et al. [151] | 2006 | 16 | Peg-IFN-α2b | 1 mcg/kg/week (n = 9), 0.5 mcg/kg/week (n = 7) | 12.5% |
| Covic et al. [154] | 2006 | 78 | Peg-IFN-α2a | 135 mcg/week | 14% |
| Espinosa et al. [36] | 2007 | 16 | Peg-IFN-α2a (n = 7) Peg-IFN-α2b (n = 9) |
1.5 mcg/week (n = 9), 135 mcg/kg/week (n = 7) |
25% |
| Casanovas-Taltavull et al. [155] | 2007 | 12 | Peg-IFN-α2a | 135 mcg/week | 25% |
| Ucmak et al. [156] | 2008 | 12 | Peg-IFN-α2a | 135 mcg/week | 50% |
| Sikole et al. [157] | 2008 | 14 | Peg-IFN-α2a | 135 mcg/week | 41% |
| Liu et al. [158] | 2008 | 25 | Peg-IFN-α2a | 135 mcg/week | 48% |
| Ayaz et al. [159] | 2008 | 22 | Peg-IFN-α2a | 135 mcg/week | 50% |
| Akhan et al. [160] | 2008 | 12 | Peg-IFN-α2a | 135 mcg/week | 50% |
| Werner et al. [168] | 2010 | 22 | Peg-IFN-α2a (n = 9) Peg-IFN-α2b (n = 13) |
180 mcg/week 1.5 mcg/kg/week 1 mcg/kg/week (1 patient) |
45% |
IFN: interferon; MU: million units; Peg-IFN: pegylated interferon; SVR: sustained virological response.
Interferon therapy pretransplant has been associated to a reduced incidence of post-transplant de novo or recurrent glomerulonephritis. Cruzado et al. in 2003 [169] found that of 15 HCV+ KT recipients who received prerenal transplantation interferon, 10 (67%) became negative at the time of renal transplantation, and only one of 15 (6.7%) developed de novo glomerulonephritis (this patient was HCV RNA+ at transplantation). Among untreated controls, 12 out of 60 (19%) developed de novo glomerulonephritis post-KT, all 12 had detectable HCV RNA at transplantation.
Pretransplant antiviral therapy of HCV may also reduce the incidence of post-transplant diabetes mellitus (PTDM) in allograft recipients. In a controlled trial, Gursoy et al.[170] observed that the frequency of PTDM was higher in the group of HCV+ recipients who had not received IFN than in those who had been treated with IFN before transplantation, 25% (10/40) versus 7.1% (1/14), P = .009.
8. Therapy of Chronic HCV Infection in Kidney Transplant Recipients
The efficacy and safety of IFN-based therapy of hepatitis C after KT is unsatisfactory [144, 171–174]. The potential benefits need to be weighed against the risk of allograft rejection.
The administration of IFN after kidney transplantation can be deleterious to the allograft and should generally be avoided in kidney transplant recipients unless there is indication of worsening hepatic injury on biopsy or clinically decompensating liver disease. Reported rates of kidney graft dysfunction after IFN treatment range from 9 to 100%, with most episodes occurring between 0.3 and 8 months after initiation of therapy. Most kidney graft dysfunction was related to increased rates of acute rejection, which is frequently steroid resistant and irreversible and could lead to graft loss [54].
Apart from the antiviral effects mediated through the Jak-Stat signaling pathway, IFN is a potent immunomodulator affecting both the innate and the adaptive immune system [175–181].
The association between ACR and antiviral therapy was initially described in renal transplant recipients and was subsequently reported in liver transplant patients [182, 183]. Interferon alpha (IFNα) activates a large number of interferon stimulated genes (ISGs), which combined with the upregulation of MHC antigen expression results in increased antigen presentation, T-cell activation, and dominance of a Th1 response including release of TNFα, IL2, IL12, IFNγ, FasL, perforin, and GrzB activities, and decrease on IL10 and T-reg activity, collectively leading to tissue damage and inflammation. Also, ribavirin potentiates ISGs expression skewing toward TH response. IFNα also enhances recruitment and activity of other nonspecific cell types such as natural killer (NK) cells, macrophages, neutophiles, and monocytes.
While expansions of T-cell clones directed to viral antigens contribute to viral load reduction and clearance, expansions of T-cell clones to alloantigens may trigger immune-related disorders including acute cellular rejection and chronic ductopenic rejection as well as de novo autoimmune hepatitis.
ACR is often associated with concomitant low or negative serum HCV RNA. It has been suggested that HCV clearance during IFN-based therapy improves hepatic microsomal function, which in turn leads to lower immunosuppressant levels in blood putting patients at higher risk of development of ACR.
The American Association for the Study of the Liver Disease (AASLD) specifically recommends that kidney transplantation is a contraindication to IFN therapy for HCV infection. However, controlled and cohort (prospective or retrospective) studies have addressed this issue in kidney transplant recipients.
A meta-analysis of clinical trials of IFN-based therapy (interferon alone or with ribavirin) in KT recipients with chronic hepatitis C showed that the summary estimate for SVR rate was 18.0% (95% CI, 7.0–29%) with a drop-out rate of 35% (95% CI, 20–50%) [174]. The most frequent side-effect requiring discontinuation was acute rejection refractory to corticosteroid therapy. Combined antiviral therapy (interferon plus ribavirin) has been evaluated in a few studies [172, 173]. Shu et al. [173] in 2004 reported an SVR of 27% (3/11) and a drop-out rate of 27% (3/11) due to graft dysfunction (n = 1) and urosepsis (n = 2) during antiviral therapy with very low dose IFN-α (1 MU s.c. three times weekly) for 48 weeks.
Thus, antiviral therapy with IFN, as state in KDIGO clinical practice guidelines 2008, should only be considered in patients with fibrosing cholestatic hepatitis or life-threatening vasculitis in whom the risk of not treating justifies the possible loss of the allograft [54].
Alternative regimens based on amantadine, RBV monotherapy, or their combination have been proposed, but no proof of their efficacy has been provided [184–187], and therefore they are not recommended.
9. Combined Kidney-Liver Transplantion in Patients with Hepatitis C
As cirrhosis and the development of liver cell cancer constitute an important risk factor for death and renal dysfunction after KT alone, combined kidney/liver transplantation should be considered for KT candidates with cirrhosis.
Since the adoption of the Model for End-Stage Liver Disease (MELD) score for allocating organs in the US in 2002, there has been a significant increase in simultaneous liver kidney (SLK) transplantation [188]. However, data are controversial and do not identify which patient should be offered SLK transplantation [189–194].
In 2008 an American consensus conference [195] convened to establish guidelines for evaluation, listing and transplantation of patients with end-stage liver disease (ESLD) and renal failure. The consensus agreed that the following conditions represent clear indications for listing for SKL:
End-stage renal disease with cirrhosis and symptomatic portal hypertension or hepatic vein wedge pressure gradient ≥10 mm Hg.
Liver failure and CKD with GFR ≤30 mL/min.
AKI or hepatorenal syndrome with serum creatinine ≥2.0 mg/dL and dialysis ≥8 weeks.
Liver failure and CKD with a renal biopsy demonstrating >30% glomerulosclerosis or 30% fibrosis.
There are many data supporting the effectiveness of SKL. One year patient survival seems to be better than liver transplantation alone (LTA) [190, 196]. Some evidence suggests the kidney allograft lasts longer in liver transplant recipients from the same donor [197, 198]. Moreover, dialysis seems to be tolerated poorly in liver transplant recipients compared with matched kidney failure only dialysis patients [199].
However, if patients with cirrhosis receive a liver and kidney transplant, this may disadvantage those who require a kidney alone. Many recent studies have reported a lower survival of renal allografts in SLK compared to KTA recipients without liver disease [189, 197, 200].
As HCV-related cirrhosis is the leading indication for liver transplantation in western countries [201] and because HCV is associated with increased morbidity and mortality among both liver and kidney transplant recipients [202–207], there is a clear need to obtain data on the natural history and management of recurrent hepatitis C in the SKL setting.
In 2009, Del Pozo [208] compared outcomes among HCV+ and HCV− recipients of SLK with HCV+ recipients of isolated liver transplant, but did not find any significant difference in terms of 1-, 2-, and 5-years survival (P = .6). They found that HCV+ patients undergoing SKL were significantly older than HCV− patients (61 versus 51 years, P = .01). Diabetes after SLK was significantly more prevalent in the HCV+ group (78% versus 28%, P = .01). There were no significant differences between HCV+ and HCV− SKL recipients in terms of kidney graft function and kidney and liver rejection.
Van Wagner and colleagues [209], in the largest study reported to date, analyzed the outcome of patients with HCV infection undergoing SLK transplant, compared to that of HCV+ patient underwent LTA.
Despite many limitations, such as the retrospective nature of the studies, the heterogeneity of the indication for SKL, the lack of a control group of HCV-SLK recipients, and the choice of a control group of LTA patients with a lower median MELD score lower (17.4 versus 38, LTA, and SLKT, resp.), reflecting less advanced liver disease.
The 1-, 3-, and 5-year overall survival rates for the SLK group were 73.7%, 61.8%, and 68.1%, and in the LTA group the rates were 91.9%, 78.8%, and 73.2%, respectively. However, once adjusted for age, gender, and MELD, there were no statistical differences (P = .298). Also, there was no difference in liver graft survival between SLK and LTA groups.
There were more early posttransplant infection episodes in the SLK (56.3%) compared with LTA (21.6%) (P = .001) and there was a trend towards increased early mortality in the SLK group (P = .08), as reported in others studies [197, 200, 210–212].
There was no difference in the time to HCV recurrence, the proportion with ≥stage 2 fibrosis, renal function, and graft function between the groups. This study does not report posttransplant diabetes.
Ten of the 17 SLK recipients with HCV recurrence underwent antiviral therapy with pegylated IFN and RBV. Of these 10 SKL patients, two achieved SVR and 5 discontinued therapy; of the 14 liver only recipients, 5 achieved SVR and seven discontinued therapy. There were no episodes of liver or kidney rejection while on treatment in the SKL group, while one episode of liver rejection was documented in the LTA group. The authors speculated that the simultaneous transplantation of kidney and liver may protect the kidney graft against acute rejection induced by PEG-IFN alpha treatment; this is in keeping with evidence that the liver transplant provides some level of immunologic protection to the kidney allograft [197, 200].
Similar findings were reported in two case reports [213, 214] and in a small case series by Schmitz et al. [215], who showed, among 6 recipients of combined kidney-liver transplant (4 simultaneous, 2 consecutive), one episode of liver rejection after antiviral treatment with PEG-IFN alfa2b, but no episodes of kidney rejection were reported; the rate of SVR was 50% (3/6).
Based on these data, antiviral treatment for HCV recurrence in SLK recipients appears safe, but additional prospective studies with larger patient populations are needed to further validate the feasibility of such antiviral treatment.
10. Conclusion
The prevalence of hepatitis C in patients with chronic kidney disease (CKD) on hemodialysis (HD) is higher than that in the general population. Hepatitis C reduces survival both in dialysis patients and renal transplant recipients. Liver biopsy performed before KT is an important tool to determine the severity of liver disease in HCV+ patients and may help to assess the prognosis and the management of the patients both before and after transplantation. Transplantation of kidneys from HCV+ donors restricted to HCV+ recipients may confer an advantage in terms of waiting time in this population although the results on outcome seem to be controversial. Monotherapy with conventional IFN or Pegylated-IFN for chronic hepatitis C seems to be effective in patients on haemodialysis. Data available about combination therapy with pegylated interferon plus ribavirin are limited. While IFN treatment in HCV+ kidney transplant candidates is recommended, treatment post-KT should be restricted to patients in whom the risk of not treating justifies the possible loss of the allograft (such as fibrosing cholestatic hepatitis). Otherwise, it is contraindicated, because of the high risk of rejection and consequent graft loss. Simultaneous kidney/liver transplantation should be considered for renal transplant candidates with decompensated cirrhosis.
Treatment of HCV recurrence in SLK recipients appears effective and safe, although further studies are needed to validate this data.
References
- 1.Lauer GM, Walker BD. Hepatitis C virus infection. New England Journal of Medicine. 2001;345(1):41–52. doi: 10.1056/NEJM200107053450107. [DOI] [PubMed] [Google Scholar]
- 2.Wen CP, Cheng TY, Tsai MK, et al. All-cause mortality attributable to chronic kidney disease: a prospective cohort study based on 462 293 adults in Taiwan. The Lancet. 2008;371(9631):2173–2182. doi: 10.1016/S0140-6736(08)60952-6. [DOI] [PubMed] [Google Scholar]
- 3.Scott DR, Wong JK, Spicer TS, et al. Adverse impact of hepatitis C virus infection on renal replacement therapy and renal transplant patients in Australia and New Zealand. Transplantation. 2010;90(11):1165–1171. doi: 10.1097/TP.0b013e3181f92548. [DOI] [PubMed] [Google Scholar]
- 4.Goodkin DA, Bragg-Gresham JL, Koenig K, et al. Association of comorbid conditions and mortality in hemodialysis patients in Europe, Japan, and the United States: the dialysis outcomes and practice patterns study (DOPPS) Journal of the American Society of Nephrology. 2003;14(12):3270–3277. doi: 10.1097/01.asn.0000100127.54107.57. [DOI] [PubMed] [Google Scholar]
- 5.Perz JF, Farrington LA, Pecoraro C. Estimated global prevalence of hepatitis C virus infection. In: Proceedings of the 42nd Annual Meeting of the Infectious Diseases Society of America; September-October 2004; Boston, Mass, USA. [Google Scholar]
- 6.Anonymous. Global surveillance and control of hepatitis C. Journal of Viral Hepatitis. 1999;6(1):35–47. [PubMed] [Google Scholar]
- 7.NIH consensus statement on management of hepatitis C: 2002. NIH Consens State Sci Statements. 2002;19(3):1–46. [PubMed] [Google Scholar]
- 8.Knodell RG, Ishak KG, Black WC, et al. Formulation and application of a numeral scoring system for assessing histological activity in asymptomatic chronic active hepatitis. Hepatology. 1981;1:431–435. doi: 10.1002/hep.1840010511. [DOI] [PubMed] [Google Scholar]
- 9.Ishak K, Baptista A, Bianchi L, et al. Histological grading and staging of chronic hepatitis. Journal of Hepatology. 1995;22(6):696–699. doi: 10.1016/0168-8278(95)80226-6. [DOI] [PubMed] [Google Scholar]
- 10.Bedossa P, Poynard T. An algorithm for the grading of activity in chronic hepatitis C. Hepatology. 1996;24(2):289–293. doi: 10.1002/hep.510240201. [DOI] [PubMed] [Google Scholar]
- 11.Poynard T, Ratziu V, Charlotte F, Goodman Z, McHutchison J, Albrecht J. Rates and risk factors of liver fibrosis progression in patients with chronic hepatitis C. Journal of Hepatology. 2001;34(5):730–739. doi: 10.1016/s0168-8278(00)00097-0. [DOI] [PubMed] [Google Scholar]
- 12.Marcellin P, Akremi R, Cazals D, et al. Genotype 1 is associated with a slower progression of fibrosis in untreated patients with mild chronic hepatitis C. Journal of Hepatology. 2001;34(supplement 1):p. 159. [Google Scholar]
- 13.Ghany MG, Kleiner DE, Alter HJ, et al. Progression of fibrosis in early stages of chronic hepatitis C. Hepatology. 2000;32:p. 496A. [Google Scholar]
- 14.Alberti A, et al. Outcome of initially mild chronic hepatitis C. Hepatology. 2001;34:p. 225A. [Google Scholar]
- 15.Pereira BJG, Levey AS. Hepatitis C virus infection in dialysis and renal transplantation. Kidney International. 1997;51(4):981–999. doi: 10.1038/ki.1997.139. [DOI] [PubMed] [Google Scholar]
- 16.Finelli L, Miller JT, Tokars JI, Arduino MJ. National surveillance of dialysis-associated diseases in the United States, 2002. Seminars in Dialysis. 2005;18(1):52–61. doi: 10.1111/j.1525-139X.2005.18108.x. [DOI] [PubMed] [Google Scholar]
- 17.Fissell RB, Bragg-Gresham JI, Woods JD, et al. Patterns of hepatitis C prevalence and seroconversion in hemodialysis units from three continents: the DOOPS. Kidney International. 2004;65(6):2335–2342. doi: 10.1111/j.1523-1755.2004.00649.x. [DOI] [PubMed] [Google Scholar]
- 18.Jadoul M, Poignet JL, Geddes C, et al. The changing epidemiology of hepatitis C virus infection in haemodialysis: European multicentre study. Nephrology Dialysis Transplantation. 2004;19(4):904–909. doi: 10.1093/ndt/gfh012. [DOI] [PubMed] [Google Scholar]
- 19.Fabrizi F, Poordad FF, Martin P. Hepatitis C infection and the patient with end-stage renal disease. Hepatology. 2002;36(1):3–10. doi: 10.1053/jhep.2002.34613. [DOI] [PubMed] [Google Scholar]
- 20.Covic A, Iancu L, Apetrei C, et al. Hepatitis virus infection in haemodialysis patients from Moldavia. Nephrology Dialysis Transplantation. 1999;14(1):40–45. doi: 10.1093/ndt/14.1.40. [DOI] [PubMed] [Google Scholar]
- 21.Saxena AK, Panhotra BR. The impact of nurse understaffing on the transmission of hepatitis C virus in a hospital-based hemodialysis unit. Medical Principles and Practice. 2004;13(3):129–135. doi: 10.1159/000076951. [DOI] [PubMed] [Google Scholar]
- 22.Hmajed F, Mamou MB, Saune-Sandres K, et al. Hepatitis C virus infection among dialysis patients in Tunisia: incidence and molecular evidence for nosocomial transmission. Journal of Medical Virology. 2006;78(2):185–191. doi: 10.1002/jmv.20526. [DOI] [PubMed] [Google Scholar]
- 23.Periera BJG, Wright TL, Schmid CH, Levey AS. The impact of pretransplantation hepatitis C infection on the outcome of renal transplantation. Transplantation. 1995;60(8):799–805. [PubMed] [Google Scholar]
- 24.Stempel CA, Lake J, Kuo G, Vincenti F. Hepatitis C—its prevalence in end-stage renal failure patients and clinical course after kidney transplantation. Transplantation. 1993;55(2):273–276. doi: 10.1097/00007890-199302000-00008. [DOI] [PubMed] [Google Scholar]
- 25.Huang CC, Liaw YF, Lai MK, Chu SH, Chuang CK, Huang JY. The clinical outcome of hepatitis C virus antibody-positive renal allograft recipients. Transplantation. 1992;53(4):763–765. doi: 10.1097/00007890-199204000-00011. [DOI] [PubMed] [Google Scholar]
- 26.Ponz E, Campistol JM, Barrera JM, et al. Hepatitis C virus antibodies in patients on hemodialysis and after kidney transplantation. Transplantation Proceedings. 1991;23(1):1371–1372. [PubMed] [Google Scholar]
- 27.Roth D, Zucker K, Cirocco R, et al. The impact of hepatitis C virus infection on renal allograft recipients. Kidney International. 1994;45(1):238–244. doi: 10.1038/ki.1994.29. [DOI] [PubMed] [Google Scholar]
- 28.Roth D. Hepatitis C virus: the nephrologist's view. American Journal of Kidney Diseases. 1995;25(1):3–16. doi: 10.1016/0272-6386(95)90617-7. [DOI] [PubMed] [Google Scholar]
- 29.Ynares C, Johnson HK, Kerlin T, Crowe D, MacDonell R, Richie R. Impact of pretransplant hepatitis C antibody status upon long-term patient and renal allograft survival-A 5- and 10-year follow-up. Transplantation Proceedings. 1993;25(1):1466–1468. [PubMed] [Google Scholar]
- 30.Fritsche C, Brandes JC, Delaney SR, et al. Hepatitis C is a poor prognostic indicator in black kidney transplant recipients. Transplantation. 1993;55(6):1283–1287. doi: 10.1097/00007890-199306000-00014. [DOI] [PubMed] [Google Scholar]
- 31.Fabrizi F, Martin P, Dixit V, Bunnapradist S, Dulai G. Meta-analysis: effect of hepatitis C virus infection on mortality in dialysis. Alimentary Pharmacology and Therapeutics. 2004;20(11-12):1271–1277. doi: 10.1111/j.1365-2036.2004.02290.x. [DOI] [PubMed] [Google Scholar]
- 32.The current state of chronic dialysis treatment in Japan (as of December 31, 2000) Therapeutic Apheresis and Dialysis. 2003;7(1):3–35. [PubMed] [Google Scholar]
- 33.Fabrizi F, Takkouche B, Lunghi G, Dixit V, Messa P, Martin P. The impact of hepatitis C virus infection on survival in dialysis patients: meta-analysis of observational studies. Journal of Viral Hepatitis. 2007;14(10):697–703. doi: 10.1111/j.1365-2893.2007.00868.x. [DOI] [PubMed] [Google Scholar]
- 34.Pereira BJ, Natov SN, Bouthot BA, et al. Effect of hepatitis C infection and renal transplantation on survival in end-stage renal disease. Kidney International. 1998;53(5):1374–1381. doi: 10.1046/j.1523-1755.1998.00883.x. [DOI] [PubMed] [Google Scholar]
- 35.Meyers CM, Seeff L, Stehman-Breen CO, Hoofnagle JH. Hepatitis C and renal disease: an update. American Journal of Kidney Diseases. 2003;42(4):631–657. doi: 10.1016/s0272-6386(03)00828-x. [DOI] [PubMed] [Google Scholar]
- 36.Espinosa M, Arenas MD, Aumente MD, et al. Anemia associated with pegylated interferon-alpha2a and alpha2b therapy in hemodialysis patients. Clinical Nephrology. 2007;6:366–373. doi: 10.5414/cnp67366. [DOI] [PubMed] [Google Scholar]
- 37.Port F, Wolfe R, Mauger E, et al. Comparison of survival probabilities for dialysis patients versus cadaveric renal transplant recipients. Journal of the American Medical Association. 1993;270:p. 1339. [PubMed] [Google Scholar]
- 38.Maluf DG, Fisher RA, King AL, et al. Hepatitis C virus infection and kidney transplantation: predictors of patient and graft survival. Transplantation. 2007;83(7):853–857. doi: 10.1097/01.tp.0000259725.96694.0a. [DOI] [PubMed] [Google Scholar]
- 39.Bloom RD, Sayer G, Fa K, Constantinescu S, Abt P, Reddy KR. Outcome of hepatitis C virus-infected kidney transplant candidates who remain on the waiting list. American Journal of Transplantation. 2005;5(1):139–144. doi: 10.1111/j.1600-6143.2004.00652.x. [DOI] [PubMed] [Google Scholar]
- 40.Morales JM. Hepatitis C and renal transplantation: outcome of patients. Nephrology Dialysis Transplantation. 1995;10(supplement 1):125–128. doi: 10.1093/ndt/10.supp6.125. [DOI] [PubMed] [Google Scholar]
- 41.Goffin E, Pirson Y, van Ypersele de Strihou C. Implications of chronic hepatitis B or hepatitis C infection for renal transplant candidates. Nephrology Dialysis Transplantation. 1995;10(supplement 6):88–92. doi: 10.1093/ndt/10.supp6.88. [DOI] [PubMed] [Google Scholar]
- 42.Kliem V, van den Hoff U, Brunkhorst R, et al. The longterm course of hepatitis C after kidney transplantation. Transplantation. 1996;62:1417–1421. doi: 10.1097/00007890-199611270-00007. [DOI] [PubMed] [Google Scholar]
- 43.Rostaing L, Rumeau JL, Cisterne J, Izopet J, Chabannier MH, Durand D. Liver histology in renal transplant patients after more than 10 years of hepatitis C virus infection. Transplantation Proceedings. 1996;28(5):2836–2837. [PubMed] [Google Scholar]
- 44.Einollahi B, Hajarizadeh B, Bakhtiari S, et al. Pretransplant hepatitis C virus infection and its effect on the post-transplant course of living renal allograft recipients. Journal of Gastroenterology and Hepatology. 2003;18(7):836–840. doi: 10.1046/j.1440-1746.2003.03063.x. [DOI] [PubMed] [Google Scholar]
- 45.Hanafusa T, Ichikawa Y, Kishikawa H, et al. Retrospective study on the impact of hepatitis C virus infection on kidney transplant patients over 20 years. Transplantation. 1998;66(4):471–476. doi: 10.1097/00007890-199808270-00010. [DOI] [PubMed] [Google Scholar]
- 46.Fabrizi F, Martin P, Dixit V, Bunnapradist S, Dulai G. Hepatitis C virus antibody status and survival after renal transplantation: meta-analysis of observational studies. American Journal of Transplantation. 2005;5(6):1452–1461. doi: 10.1111/j.1600-6143.2005.00864.x. [DOI] [PubMed] [Google Scholar]
- 47.Pereira BJG, Wright T, Schmid CH, Levey AS. A controlled study of hepatitis C transmission by organ transplantation. The Lancet. 1995;345(8948):484–487. doi: 10.1016/s0140-6736(95)90583-9. [DOI] [PubMed] [Google Scholar]
- 48.Legendre CH, Garrigue V, Le Bihan C, et al. Harmful long-term impact of hepatitis C virus infection in kidney transplant recipients. Transplantation. 1998;65(5):667–670. doi: 10.1097/00007890-199803150-00011. [DOI] [PubMed] [Google Scholar]
- 49.Gentil MA, Rocha JL, Algarra GR, et al. Impaired kidney transplant survival in patients with antibodies to hepatitis C virus. Nephrology Dialysis Transplantation. 1999;14(10):2455–2460. doi: 10.1093/ndt/14.10.2455. [DOI] [PubMed] [Google Scholar]
- 50.Lee WC, Shu KH, Cheng CH, Wu MJ, Chen CH, Lian JD. Longterm impact of hepatitis B, C virus infection on renal transplantation. American Journal of Nephrology. 2001;21(4):300–306. doi: 10.1159/000046265. [DOI] [PubMed] [Google Scholar]
- 51.Breitenfeldt MK, Rasenack J, Berthold H, et al. Impact of hepatitis B and C on graft loss and mortality of patients after kidney transplantation. Clinical Transplantation. 2002;16(2):130–136. doi: 10.1034/j.1399-0012.2002.1o034.x. [DOI] [PubMed] [Google Scholar]
- 52.Bruchfeld A, Wilczek H, Elinder CG. Hepatitis C infection, time in renal-replacement therapy, and outcome after kidney transplantation. Transplantation. 2004;78(5):745–750. doi: 10.1097/01.tp.0000131948.29742.24. [DOI] [PubMed] [Google Scholar]
- 53.Knoll GA, Tankersley MR, Lee JY, Julian BA, Curtis JJ. The impact of renal transplantation on survival in hepatitis C-positive end-stage renal disease patients. American Journal of Kidney Diseases. 1997;29(4):608–614. doi: 10.1016/s0272-6386(97)90345-0. [DOI] [PubMed] [Google Scholar]
- 54.Kidney disease: improving global outcomes (KDIGO) Kidney International. 2008;(109):S1–S99. doi: 10.1038/ki.2008.81. [DOI] [PubMed] [Google Scholar]
- 55.Zylberberg H, Nalpas B, Carnot F, et al. Severe evolution of chronic hepatitis C in renal transplantation: a case control study. Nephrology Dialysis Transplantation. 2002;17(1):129–133. doi: 10.1093/ndt/17.1.129. [DOI] [PubMed] [Google Scholar]
- 56.Alric L, DiMartino V, Selves J, et al. Long-term impact of renal transplantation on liver fibrosis during hepatitis C virus infection. Gastroenterology. 2002;123(5):1494–1499. doi: 10.1053/gast.2002.36610. [DOI] [PubMed] [Google Scholar]
- 57.Cosio G, Sedmak DD, Henry ML, et al. The high prevalence of severe early posttransplant renal allograft pathology inhepatitis C positive recipients. Transplantation. 1996;62(8):1054–1059. doi: 10.1097/00007890-199610270-00004. [DOI] [PubMed] [Google Scholar]
- 58.Roth D, Cirocco R, Zucker K, et al. De novo membranoproliferative glomerulonephritis in hepatitis C virus infected renal allograft recipients. Transplantation. 1995;59(12):1676–1682. doi: 10.1097/00007890-199506270-00006. [DOI] [PubMed] [Google Scholar]
- 59.Ozdemir BH, Ozdemir FN, Sezer S, Colak T, Haberal M. De novo glomerulonephritis in renal allografts with hepatitis C virus infection. Transplantation Proceedings. 2006;38(2):492–495. doi: 10.1016/j.transproceed.2005.12.109. [DOI] [PubMed] [Google Scholar]
- 60.Morales JM, Pascual-Capdevila J, Campistol JM, et al. Membranous glomerulonephritis associated with hepatitis C virus infection in renal transplant patients. Transplantation. 1997;63(11):1634–1639. doi: 10.1097/00007890-199706150-00017. [DOI] [PubMed] [Google Scholar]
- 61.Mahmoud IM, Sobh MA, El-Habashi AF, et al. Interferon therapy in hemodialysis patients with chronic hepatitis C: study of tolerance, efficacy and post-transplantation course. Nephron Clinical Practice. 2005;100(4):c133–c139. doi: 10.1159/000085442. [DOI] [PubMed] [Google Scholar]
- 62.Cruzado JM, Torras J, Gil-Vernet S, et al. Glomerulonephritis associated with hepatitis C virus infection after renal transplantation. Nephrology Dialysis Transplantation. 2000;15(supplement 8):65–67. doi: 10.1093/ndt/15.suppl_8.65. [DOI] [PubMed] [Google Scholar]
- 63.Cruzado JM, Gil-Vernet S, Ercilla G, et al. Hepatitis C virus-associated membranoproliferative glomerulonephritis in renal allografts. Journal of the American Society of Nephrology. 1996;7(11):2469–2475. doi: 10.1681/ASN.V7112469. [DOI] [PubMed] [Google Scholar]
- 64.Cruzado JM, Carrera M, Torras J, Grinyó JM. Hepatitis C virus infection and de novo glomerular lesions in renal allografts. American Journal of Transplantation. 2001;1(2):171–178. [PubMed] [Google Scholar]
- 65.Morales JM, Marcén R, Andres A, et al. Renal transplantation in patients with hepatitis C virus antibody. A long national experience. NDT Plus. 2010;3(supplement 2):ii41–ii46. doi: 10.1093/ndtplus/sfq070. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Paul LC. Chronic renal transplant loss. Kidney International. 1995;47(6):1491–1499. doi: 10.1038/ki.1995.211. [DOI] [PubMed] [Google Scholar]
- 67.Bia MJ. Nonimmunologic causes of late renal graft loss. Kidney International. 1995;47:1470–1480. doi: 10.1038/ki.1995.206. [DOI] [PubMed] [Google Scholar]
- 68.Koskinen P, Lemstrom K, Hayry P. Chronic rejection. Current Opinion in Nephrology and Hypertension. 1996;5:269–279. doi: 10.1097/00041552-199605000-00013. [DOI] [PubMed] [Google Scholar]
- 69.Sabry A. Proteinuria among renal transplant patients and its relation to hepatitis c virus and graft outcome: a single center experience. Experimental and Clinical Transplantation. 2010;8(2):91–97. [PubMed] [Google Scholar]
- 70.Baid S, Pascual M, Williams WW, et al. Renal thrombotic microangiopathy associated with anticardiolipin antibodies in hepatitis C virus-infected renal allograft recipients. Transplantation. 1995;59:p. 1676. doi: 10.1681/ASN.V101146. [DOI] [PubMed] [Google Scholar]
- 71.Abbott KC, Lentine KL, Bucci JR, et al. Impact of diabetes and hepatitis after kidney transplantation on patients who are affected by hepatitis C virus. Journal of the American Society of Nephrology. 2004;15(12):3166–3174. doi: 10.1097/01.ASN.0000145439.48387.BF. [DOI] [PubMed] [Google Scholar]
- 72.Chazouilleres O, Kim M, Combs C, et al. Quantitation of hepatitis C virus RNA in liver transplant recipients. Gastroenterology. 1994;106(4):994–999. doi: 10.1016/0016-5085(94)90759-5. [DOI] [PubMed] [Google Scholar]
- 73.Berenguer M. Management of hepatitis C virus in the transplant patient. Clinics in Liver Disease. 2007;11(2):355–376. doi: 10.1016/j.cld.2007.04.010. [DOI] [PubMed] [Google Scholar]
- 74.Pelletier SJ, Raymond DP, Crabtree TD, et al. Hepatitis C-induced hepatic allograft injury is associated with a pre-transplantation elevated viral replication rate. Hepatology. 2000;32(2):418–426. doi: 10.1053/jhep.2000.9408. [DOI] [PubMed] [Google Scholar]
- 75.Berenguer M, Lopez-Labrador FX, Greenberg HB, Wright TL. Hepatitis C virus and the host: an imbalance induced by immunosuppression. Hepatology. 2000;32(2):433–435. doi: 10.1053/jhep.2000.16184. [DOI] [PubMed] [Google Scholar]
- 76.Di Martino V, Saurini F, Samuel D, et al. Long-term longitudinal study of intrahepatic hepatitis C virus replication after liver transplantation. Hepatology. 1997;26(5):1343–1350. doi: 10.1053/jhep.1997.v26.pm0009362382. [DOI] [PubMed] [Google Scholar]
- 77.Sreekumar R, Gonzalez-Koch A, Maor-Kendler Y, et al. Early identification of recipients with progressive histologic recurrence of hepatitis C after liver transplantation. Hepatology. 2000;32(5):1125–1130. doi: 10.1053/jhep.2000.19340. [DOI] [PubMed] [Google Scholar]
- 78.Papatheodoridis GV, Barton SG, Andrew D, et al. Longitudinal variation in hepatitis C virus (HCV) viraemia and early course of HCV infection after liver transplantation for HCV cirrhosis: the role of different immunosuppressive regimens. Gut. 1999;45(3):427–434. doi: 10.1136/gut.45.3.427. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Neumann AU, Lam NP, Dahari H, et al. Hepatitis C viral dynamics in vivo and the antiviral efficacy of interferon-α therapy. Science. 1998;282(5386):103–107. doi: 10.1126/science.282.5386.103. [DOI] [PubMed] [Google Scholar]
- 80.Gretch D, Bacchi C, Corey L, et al. Persistent hepatitis C virus infection after liver transplantation: clinical and virological features. Hepatology. 1995;22(1):1–9. [PubMed] [Google Scholar]
- 81.Doughty AL, Spencer JD, Cossart YE, McCaughan GW. Cholestatic hepatitis after liver transplantation is associated with persistently high serum hepatitis C virus RNA levels. Liver Transplantation and Surgery. 1998;4(1):15–21. doi: 10.1002/lt.500040102. [DOI] [PubMed] [Google Scholar]
- 82.Hooda AK, Puri P, Narula AS, Raychaudhury N, Varghese SJ, Basu A. Hepatitis C virus-related fibrosing cholestatic hepatitis in a renal transplant recipient. Indian Journal of Gastroenterology. 2006;25(6):308–309. [PubMed] [Google Scholar]
- 83.Delladetsima JK, Boletis JN, Makris F, Psichogiou M, Kostakis A, Hatzakis A. Fibrosing cholestatic hepatitis in renal transplant recipients with hepatitis C virus infection. Liver Transplantation and Surgery. 1999;5(4):294–300. doi: 10.1002/lt.500050417. [DOI] [PubMed] [Google Scholar]
- 84.De Bustillo EM, Ibarrola C, Colina F, et al. Fibrosing cholestatic hepatitis in hepatitis C virus-infected renal transplant recipients. Journal of the American Society of Nephrology. 1998;9(6):1109–1113. doi: 10.1681/ASN.V961109. [DOI] [PubMed] [Google Scholar]
- 85.Toth CM, Pascual M, Chung RT, et al. Hepatitis C virus- associated fibrosing cholestatic hepatitis after renal transplantation: response to interferon-alpha therapy. Transplantation. 1998;66(9):1254–1258. doi: 10.1097/00007890-199811150-00023. [DOI] [PubMed] [Google Scholar]
- 86.Kahraman A, Witzke O, Scherag A, et al. Impact of immunosuppressive therapy on hepatitis C infection after renal transplantation. Clinical Nephrology. 2011;75(1):16–25. [PubMed] [Google Scholar]
- 87.Zekry A, Gleeson M, Guney S, McCaughan GW. A prospective cross-over study comparing the effect of mycophenolate versus azathioprine on allograft function and viral load in liver transplant recipients with recurrent chronic HCV infection. Liver Transplantation. 2004;10(1):52–57. doi: 10.1002/lt.20000. [DOI] [PubMed] [Google Scholar]
- 88.Abbott KC, Bucci JR, Matsumoto CS, et al. Hepatitis C and renal transplantation in the era of modern immunosuppression. Journal of the American Society of Nephrology. 2003;14(11):2908–2918. doi: 10.1097/01.asn.0000090743.43034.72. [DOI] [PubMed] [Google Scholar]
- 89.Akalin E, Murphy B, Sehgal V, Ames S, Daly L, Bromberg JS. Rapid steroid withdrawal in hepatitis C virus-positive kidney transplant recipients. Clinical Transplantation. 2004;18(4):384–389. doi: 10.1111/j.1399-0012.2004.00177.x. [DOI] [PubMed] [Google Scholar]
- 90.Luan FL, Schaubel DE, Zhang H, et al. Impact of immunosuppressive regimen on survival of kidney transplant recipients with hepatitis C. Transplantation. 2008;85(11):1601–1606. doi: 10.1097/TP.0b013e3181722f3a. [DOI] [PubMed] [Google Scholar]
- 91.Bestard O, Cruzado JM, Torras J, et al. Long-term effect of hepatitis C virus chronic infection on patient and renal graft survival. Transplantation Proceedings. 2005;37(9):3774–3777. doi: 10.1016/j.transproceed.2005.09.170. [DOI] [PubMed] [Google Scholar]
- 92.Fabrizi F, Lunghi G, Colucci P, Finazzi S, Ponticelli C, Locatelli F. Reduced aminotransferace activity in patients with chronic renal failure not requiring dialysis: impact on the evaluation of viral hepatitis. American Journal of Kidney Diseases. 2001;28:1009–1015. doi: 10.1053/ajkd.2001.28590. [DOI] [PubMed] [Google Scholar]
- 93.Martin P, Carter D, Fabrizi F, et al. Histopathological features of hepatitis C in renal transplant candidates. Transplantation. 2000;69(7):1479–1484. doi: 10.1097/00007890-200004150-00045. [DOI] [PubMed] [Google Scholar]
- 94.Caramelo C, Ortiz A, Aguilera B, et al. Liver disease patterns in hemodialysis patients with antibodies to hepatitis C virus. American Journal of Kidney Diseases. 1993;22(6):822–828. doi: 10.1016/s0272-6386(12)70341-4. [DOI] [PubMed] [Google Scholar]
- 95.Cotler SJ, Diaz G, Gundlapalli S, et al. Characteristics of hepatitis C in renal transplant candidates. Journal of Clinical Gastroenterology. 2002;35(2):191–195. doi: 10.1097/00004836-200208000-00013. [DOI] [PubMed] [Google Scholar]
- 96.Glicklich D, Thung SN, Kapoian T, Tellis V, Reinus JF. Comparison of clinical features and liver histology in hepatitis C-positive dialysis patients and renal transplant recipients. American Journal of Gastroenterology. 1999;94(1):159–163. doi: 10.1111/j.1572-0241.1999.00788.x. [DOI] [PubMed] [Google Scholar]
- 97.Pol S, Romeo R, Zins B, et al. Hepatitis C virus RNA in anti-HCV positive hemodialyzed patients: significance and therapeutic implications. Kidney International. 1993;44(5):1097–1100. doi: 10.1038/ki.1993.354. [DOI] [PubMed] [Google Scholar]
- 98.Sterling RK, Sanyal AJ, Luketic VA, et al. Chronic hepatitis C infection in patients with end stage renal disease: characterization of liver histology and viral load in patients awaiting renal transplantation. American Journal of Gastroenterology. 1999;94(12):3576–3582. doi: 10.1111/j.1572-0241.1999.01649.x. [DOI] [PubMed] [Google Scholar]
- 99.Kasiske BL, Cangro CB, Hariharan S, et al. The evaluation of renal transplant candidates: clinical practice guidelines. American Journal of Transplantation. 2001;1(supplement 2):5–95. [PubMed] [Google Scholar]
- 100.Regev A, Berho M, Jeffers LJ, et al. Sampling error and intraobserver variation in liver biopsy in patients with chronic HCV infection. American Journal of Gastroenterology. 2002;97(10):2614–2618. doi: 10.1111/j.1572-0241.2002.06038.x. [DOI] [PubMed] [Google Scholar]
- 101.Siddique I, El-Naga H, Madda JP, Memon A, Hasan F. Sampling variability on percutaneous liver biopsy in patients with chronic hepatitis C virus infection. Scandinavian Journal of Gastroenterology. 2003;38(4):427–432. doi: 10.1080/00365520310000825. [DOI] [PubMed] [Google Scholar]
- 102.Scheuer PJ. Liver biopsy size matters in chronic hepatitis: bigger is better. Hepatology. 2003;38(6):1356–1358. doi: 10.1016/j.hep.2003.10.010. [DOI] [PubMed] [Google Scholar]
- 103.Schiavon LL, Schiavon JL, Filho RJ, et al. Simple blood tests as noninvasive markers of liver fibrosis in hemodialysis patients with chronic hepatitis C virus infection. Hepatology. 2007;46(2):307–314. doi: 10.1002/hep.21681. [DOI] [PubMed] [Google Scholar]
- 104.Liu CH, Liang CC, Liu CJ, et al. The ratio of aminotransferase to platelets is a useful index for predicting hepatic fibrosis in hemodialysis patients with chronic hepatitis C. Kidney International. 2010;78(1):103–109. doi: 10.1038/ki.2010.74. [DOI] [PubMed] [Google Scholar]
- 105.Schiavon LL, Narciso-Schiavon JL, Carvalho Filho RJ, et al. Serum levels of YKL-40 and hyaluronic acid as noninvasive markers of liver fibrosis in haemodialysis patients with chronic hepatitis C virus infection. Journal of Viral Hepatitis. 2008;15(9):666–674. doi: 10.1111/j.1365-2893.2008.00992.x. [DOI] [PubMed] [Google Scholar]
- 106.Varaut A, Fontaine H, Serpaggi J, et al. Diagnostic accuracy of the fibrotest in hemodialysis and renal transplant patients with chronic hepatitis C virus. Transplantation. 2005;80(11):1550–1555. doi: 10.1097/01.tp.0000183399.85804.02. [DOI] [PubMed] [Google Scholar]
- 107.Canbakan M, Senturk H, et al. Validation of biochemical markers for the prediction of liver fibrosis and necroinflammatory activity in hemodialysis patients with chronic hepatitis C. Nephron Clinical Practice. 2011;117(3):c289–c295. doi: 10.1159/000320751. [DOI] [PubMed] [Google Scholar]
- 108.Unstundag Y, Bilezikci B, Boyacioglu S, Kayata M, Ödemir N. The utility of AST/ALT ratio as a non-invasive demonstration of the degree of liver fibrosis in chronic HCV patients on long-term haemodialysis. Nephrology Dialysis Transplantation. 2000;15(10):1716–1717. doi: 10.1093/ndt/15.10.1716. [DOI] [PubMed] [Google Scholar]
- 109.Campbell MS, Constantinescu S, Furth EE, Reddy KR, Bloom RD. Effects of hepatitis C-induced liver fibrosis on survival in kidney transplant candidates. Digestive Diseases and Sciences. 2007;52(10):2501–2507. doi: 10.1007/s10620-006-9716-x. [DOI] [PubMed] [Google Scholar]
- 110.Pereira BJ, Milford EL, Kirkman RL, Levey AS. Transmission of hepatitis C virus by organ transplantation. New England Journal of Medicine. 1991;325(7):454–460. doi: 10.1056/NEJM199108153250702. [DOI] [PubMed] [Google Scholar]
- 111.Natov SN. Transmission of viral hepatitis by kidney transplantation: donor evaluation and transplant policies (part 1: hepatitis B virus) Transplant Infectious Disease. 2002;4(3):124–131. doi: 10.1034/j.1399-3062.2002.t01-1-01002.x. [DOI] [PubMed] [Google Scholar]
- 112.Pereira BJ, Wright TL, Schmid CH, et al. Screening and confirmatory testing of cadaver organ donors for hepatitis C virus infection: a U.S. national collaborative study. Kidney International. 1994;46(3):886–892. doi: 10.1038/ki.1994.346. [DOI] [PubMed] [Google Scholar]
- 113.Widell A, Mansson S, Persson NH, Thysell H, Hermodsson S, Blohme I. Hepatitis C superinfection in hepatitis C virus (HCV)-infected patients transplanted with an HCV-infected kidney. Transplantation. 1995;60(7):642–647. doi: 10.1097/00007890-199510150-00004. [DOI] [PubMed] [Google Scholar]
- 114.Zucker K, Cirocco R, Roth D, et al. Depletion of hepatitis C virus from procured kidneys using pulsatile perfusion preservation. Transplantation. 1994;57(6):832–840. doi: 10.1097/00007890-199403270-00011. [DOI] [PubMed] [Google Scholar]
- 115.Morales M, Campistol JM, Castellano G, et al. Transplantation of kidneys from donors with hepatitis C antibody into recipients with pre-transplantation anti-HCV. Kidney International. 1995;47(1):236–240. doi: 10.1038/ki.1995.29. [DOI] [PubMed] [Google Scholar]
- 116.Ali MK, Light JA, Baryte DY, et al. Donor hepatitis virus status does not adversely short-term outcomes in HCV positive recipients in renal transplantation. Transplantation. 1998;66:1694–1697. doi: 10.1097/00007890-199812270-00021. [DOI] [PubMed] [Google Scholar]
- 117.Bucci JR, Matsumoto CS, Swanson SJ, Agodoa LY, Holtzmuller KC, Abbott KC. Donor hepatitis C seropositivity: clinical correlates and effect on early graft and patient survival in adult cadaveric kidney transplantation. Journal of the American Society of Nephrology. 2002;13(12):2974–2982. doi: 10.1097/01.asn.0000034944.90425.75. [DOI] [PubMed] [Google Scholar]
- 118.Abbott KC, Lentine KL, Bucci JR, Agodoa LY, Peters TG, Schnitzler MA. The impact of transplantation with deceased donor hepatitis C-positive kidneys on survival in wait-listed long-term dialysis patients. American Journal of Transplantation. 2004;4(12):2032–2037. doi: 10.1046/j.1600-6143.2004.00606.x. [DOI] [PubMed] [Google Scholar]
- 119.Maluf DG, Archer KJ, Mas VR. Kidney grafts from HCV-positive donors: advantages and disadvantages. Transplantation Proceedings. 2010;42(7):2436–2446. doi: 10.1016/j.transproceed.2010.04.056. [DOI] [PubMed] [Google Scholar]
- 120.Northup PG, Argo CK, Nguyen DT, et al. Liver allografts from hepatitis c positive donors can offer good outcomes in hepatitis C positive recipients: a us national transplant registry analysis. Transplant International. 2010;23(10):1038–1044. doi: 10.1111/j.1432-2277.2010.01092.x. [DOI] [PubMed] [Google Scholar]
- 121.Delladetsima I, Psichogiou M, Sypsa V, et al. The course of hepatitis C virus infection in pretransplantation anti-hepatitis C virus-negative renal transplant recipients: a retrospective follow-up study. American Journal of Kidney Diseases. 2006;47(2):309–316. doi: 10.1053/j.ajkd.2005.11.008. [DOI] [PubMed] [Google Scholar]
- 122.Chan TM, Wu PC, Lok AS, Lai CL, Cheng IK. Clinicopathological features of hepatitis C virus antibody negative fatal chronic hepatitis C after renal transplantation. Nephron. 1995;71(2):213–217. doi: 10.1159/000188715. [DOI] [PubMed] [Google Scholar]
- 123.Dussol B, Brunet P, Cantaloube JF, Schleinitz N, Biagnini P, Berland Y. Hepatitis C virus infection contracted just before kidney transplantation. Nephron. 1995;71(2):p. 229. doi: 10.1159/000188719. [DOI] [PubMed] [Google Scholar]
- 124.Mendez R, El-Shahawy M, Obispo E, Aswad S, Mendex RG. Four years follow-up of hepatitis C positive kidney into hepatitis C negative recipients-prospective study. Journal of the American Society of Nephrology. 1995;6:p. 1105. [Google Scholar]
- 125.Pirsch JD, Heisey D, et al. Transplantation of Hepatitis C kidneys: defining the risk. In: Proceedings of the 14th Annual Meeting of the Society of Transplan Physicians; May 1995; Chicago, Illl, USA. [Google Scholar]
- 126.Fabrizi F, Martin P, Ponticelli C. Hepatitis C virus infection and renal transplantation. American Journal of Kidney Diseases. 2001;38(5):919–934. doi: 10.1053/ajkd.2001.28576. [DOI] [PubMed] [Google Scholar]
- 127.Widell A, Mansson S, Persson NH, Thysell H, Hermodsson S, Blohme I. Hepatitis C superinfection in hepatitis C virus -infected patients transplanted with an HCV-infected kidney. Transplantation. 1995;60(7):642–647. doi: 10.1097/00007890-199510150-00004. [DOI] [PubMed] [Google Scholar]
- 128.Schussler T, Staffeld-Coit C, Eason J, Nair S. Severe hepatitis C infection in a renal transplant recipient following hepatitis C genotype mismatch transplant. American Journal of Transplantation. 2004;4(8):1375–1378. doi: 10.1111/j.1600-6143.2004.00504.x. [DOI] [PubMed] [Google Scholar]
- 129.Colleoni N, Bucci R, Ribero M, et al. Hepatitis C virus genotype in anti-HCV-positive haemodialysis patients. Nephrology Dialysis Transplantation. 1996;11:2258–2264. doi: 10.1093/oxfordjournals.ndt.a027145. [DOI] [PubMed] [Google Scholar]
- 130.Rostaing L, Izopet J, Cisterne JM, et al. Impact of hepatitis C virus duration and hepatitis C virus genotypes on renal transplant patients: correlation with clinicopathological features. Transplantation. 1998;65(7):930–936. doi: 10.1097/00007890-199804150-00012. [DOI] [PubMed] [Google Scholar]
- 131.Russo MW, Goldsweig CD, Lacobson M, Brown RS. Interferon monotherapy for dialysis patients with chronic hepatitis C: an analysis of the literature on efficacy and safety. American Journal of Gastroenterology. 2003;98(7):1610–1615. doi: 10.1111/j.1572-0241.2003.07526.x. [DOI] [PubMed] [Google Scholar]
- 132.Degos F, Pol S, Chaix ML, et al. The tolerance and efficacy of interferon-α in haemodialysis patients with HCV infection: a multicentre, prospective study. Nephrology Dialysis Transplantation. 2001;16(5):1017–1023. doi: 10.1093/ndt/16.5.1017. [DOI] [PubMed] [Google Scholar]
- 133.Ozdemir FN, Akcay A, Sezer S, et al. A six-year follow-up after interferon-α monotherapy for chronic hepatitis C infection in hemodialysis patients. Renal Failure. 2004;26:583–588. doi: 10.1081/jdi-200031725. [DOI] [PubMed] [Google Scholar]
- 134.Rivera M, Gentil MA, Sayago M, et al. Treatment of hepatitis C virus with interferon in hemodialysis patients awaiting kidney transplant. Transplantation Proceedings. 2005;37(3):1424–1425. doi: 10.1016/j.transproceed.2005.02.054. [DOI] [PubMed] [Google Scholar]
- 135.Grgurevic I, Vince A, Buljevac M, et al. Efficacy of interferon-α in the treatment of chronic hepatitis C in dialysis patients: two therapeutic protocols compared. Nephron Clinical Practice. 2006;103(1):c8–c11. doi: 10.1159/000090505. [DOI] [PubMed] [Google Scholar]
- 136.Rocha CM, Perez RM, Ferreira AP, et al. Efficacy and tolerance of interferon-α in the treatment of chronic hepatitis C in end-stage renal disease patients on hemodialysis. Liver International. 2006;26(3):305–310. doi: 10.1111/j.1478-3231.2005.01225.x. [DOI] [PubMed] [Google Scholar]
- 137.Fabrizi F, Dulai G, Dixit V, Bunnapradist S, Martin P. Meta-analysis: interferon for the treatment of chronic hepatitis C in dialysis patients. Alimentary Pharmacology and Therapeutics. 2003;18(11-12):1071–1081. doi: 10.1046/j.1365-2036.2003.01780.x. [DOI] [PubMed] [Google Scholar]
- 138.Fabrizi F, Dixit V, Messa P, Martin P. Interferon monotherapy of chronic hepatitis C in dialysis patients: meta-analysis of clinical trials. Journal of Viral Hepatitis. 2008;15(2):79–88. doi: 10.1111/j.1365-2893.2007.00907.x. [DOI] [PubMed] [Google Scholar]
- 139.Hoofnagle JH, Seeff LB. Peginterferon and ribavirin for chronic hepatitis C. New England Journal of Medicine. 2006;355(23):2444–2451. doi: 10.1056/NEJMct061675. [DOI] [PubMed] [Google Scholar]
- 140.Tan AC, Brouwer JT, Glue P, van Leusen R, Kauffmann RH, Schalm SW. Safety of interferon and ribavirin therapy in hemodialysis patients with chronic hepatitis C: results of a pilot study. Nephrology Dialysis Transplantation. 2001;16:193–195. doi: 10.1093/ndt/16.1.193. [DOI] [PubMed] [Google Scholar]
- 141.Mousa DH, Abdalla AH, Al-Shoail A, Al-Sulaiman H, Al-Hawas FA, Al-Khader A. Alpha-interferon with ribavirin in the treatment of hemodialysis patients with hepatitis C. Transplantation Proceedings. 2004;36(6):1831–1834. doi: 10.1016/j.transproceed.2004.07.025. [DOI] [PubMed] [Google Scholar]
- 142.Bruchfeld A, Lindahl K, Reichard O, Carlsson T, Schvarcz R. Pegylated interferon and ribavirin treatment for hepatitis C in hemodialysed patients. Journal of Viral Hepatitis. 2006;13:316–321. doi: 10.1111/j.1365-2893.2005.00680.x. [DOI] [PubMed] [Google Scholar]
- 143.Rendina M, Castellaneta NM, Castellaneta A, et al. The treatment of chronic hepatitis C with peginterferon alpha2a (40 kDa) plus ribavirin in hemodialysed patients awaiting renal transplant. Journal of Hepatology. 2007;46:764–768. doi: 10.1016/j.jhep.2006.12.016. [DOI] [PubMed] [Google Scholar]
- 144.Schmitz V, Kiessling A, Bahra M, et al. Peginterferon alfa-2b plus ribavirin for the treatment of hepatitis C recurrence following combined liver and kidney transplantation. Annals of Transplantation. 2007;12(3):22–27. [PubMed] [Google Scholar]
- 145.Carriero D, Fabrizi F, Uriel AJ, Park J, Martin P, Dieterich DT. Treatment of dialysis patients with chronic hepatitis C using pegylated interferon and low-dose ribavirin. International Journal of Artificial Organs. 2008;31(4):295–302. doi: 10.1177/039139880803100404. [DOI] [PubMed] [Google Scholar]
- 146.van Leusen R, Adang RP, de Vries RA, et al. Pegylated interferon alfa-2a (40 kD) and ribavirin in haemodialysis patients with chronic hepatitis C. Nephrology Dialysis Transplantation. 2008;23(2):721–725. doi: 10.1093/ndt/gfm724. [DOI] [PubMed] [Google Scholar]
- 147.Hakim W, Sheikh S, Inayat I, et al. HCV response in patients with end stage renal disease treated with combination pegylated interferon alpha-2a and ribavirin. Journal of Clinical Gastroenterology. 2009;43:477–481. doi: 10.1097/MCG.0b013e318180803a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 148.Rebetol. Capusules and Oral Solution. Kenilworth, NJ, USA: Schering; 2004. [Google Scholar]
- 149.Strader DB, Wright T, Thomas DL, Seeff LB. Diagnosis, management, and treatment of hepatitis C. Hepatology. 2004;39(4):1147–1171. doi: 10.1002/hep.20119. [DOI] [PubMed] [Google Scholar]
- 150.Dienstag JL, McHutchison JG. American gastroenterological association technical review on the management of hepatitis C. Gastroenterology. 2006;130(1):231–264. doi: 10.1053/j.gastro.2005.11.010. [DOI] [PubMed] [Google Scholar]
- 151.Russo MW, Ghalib R, Sigal S, et al. Randomized trial of pegylated interferon alpha-2b monotherapy in haemodialysis patients with chronic hepatitis C. Nephrology Dialysis Transplantation. 2006;21(2):437–443. doi: 10.1093/ndt/gfi231. [DOI] [PubMed] [Google Scholar]
- 152.Mukherjee S, Gilroy RK, McCashland TM, Schafer DF. Pegylated interferon for recurrent hepatitis C in liver transplant recipients with renal failure: a prospective cohort study. Transplantation Proceedings. 2003;35(4):1478–1479. doi: 10.1016/s0041-1345(03)00446-9. [DOI] [PubMed] [Google Scholar]
- 153.Sporea I, Popescu A, Sirli R, et al. Pegylated interferon alpha2a treatment for chronic hepatitis C in patients on chronic hemodialysis. World Journal of Gastroenterology. 2006;12:4191–4194. doi: 10.3748/wjg.v12.i26.4191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 154.Covic A, Maftei ID, Mardare NGI, et al. Analysis of safety and efficacy of pegylated-interferon alpha-2a in hepatitis C virus positive hemodialysis patients: results from a large, multicenter audit. Journal of Nephrology. 2006;19(6):794–801. [PubMed] [Google Scholar]
- 155.Casanovas-Taltavull T, Baliellas C, Llobet M, et al. Preliminary results of treatmentwith pegylated interferon alpha2a for chronic hepatitis C virus in kidney transplant candidates on hemodialysis. Transplantation Proceedings. 2007;39(7):2125–2127. doi: 10.1016/j.transproceed.2007.07.013. [DOI] [PubMed] [Google Scholar]
- 156.Ucmak H, Kokoglu OF, Hosoglu S, et al. Long-term efficacy of pegylated interferon alpha-2a in HCV-positive hemodialysis patients. Renal Failure. 2008;30(2):227–232. doi: 10.1080/08860220701813368. [DOI] [PubMed] [Google Scholar]
- 157.Sikole A, Dzekova P, Selja N, et al. Treatment of hepatitis C in haemodialysis patients with pegylated interferon alpha2a as monotherapy. Renal Failure. 2008;29:961–966. doi: 10.1080/08860220701641579. [DOI] [PubMed] [Google Scholar]
- 158.Liu CH, Liang CC, Lin JW, et al. Pegylated interferon alfa-2a versus standard interferon alfa-2a for treatment naive dialysis patients with chronic hepatitis C: a randomized study. Gut. 2008;57(4):525–530. doi: 10.1136/gut.2007.133884. [DOI] [PubMed] [Google Scholar]
- 159.Ayaz C, Celen MK, Yuce UN, Geyik MF. Efficacy and safety of pegylated-interferon alpha-2a in hemodialysis patients with chronic hepatitis C. World Journal of Gastroenterology. 2008;14(2):255–259. doi: 10.3748/wjg.14.255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 160.Akhan SC, Kalender B, Ruzgar M. The response to pegylated interferon alpha 2a in haemodialysis patients with hepatitis C virus infection. Infection. 2008;36(4):341–344. doi: 10.1007/s15010-008-7134-z. [DOI] [PubMed] [Google Scholar]
- 161.Martin P, Mitra S, Farrington K, Martin NE, Modi MW. Pegylated (40 KD) interferon alfa-2a (Pegasys) is unaffected by renal impairment. Hepatology. 2000;32:p. 370A. [Google Scholar]
- 162.Barril G, Quiroga JA, Sanz P, Rodriguez-Salvanes F, Selgas R, Carreno V. Pegylated interferon-alpha2a kinetics during experimental hemodialysis: impact of permeability and pore size of dialysers. Alimentary Pharmacology and Therapeutics. 2004;20(1):37–44. doi: 10.1111/j.1365-2036.2004.02014.x. [DOI] [PubMed] [Google Scholar]
- 163.Fabrizi F, Dixit V, Messa P, Martin P. Pegylated interferon monotherapy of chronic hepatitis C in dialysis patients: meta-analysis of clinical trials. Journal of Medical Virology. 2010;82(5):768–775. doi: 10.1002/jmv.21542. [DOI] [PubMed] [Google Scholar]
- 164.McHutchison JG, Gordon SC, Schiff ER, et al. Interferon alfa-2b alone or in combination with ribavirin as initial treatment for chronic hepatitis C. New England Journal of Medicine. 1998;339(21):1485–1492. doi: 10.1056/NEJM199811193392101. [DOI] [PubMed] [Google Scholar]
- 165.Fabrizi F, Martin P, Dixit V, et al. Quantitative assessment of HCV load in chronic hemodialysis patients: a cross-sectional survey. Nephron. 1998;80(4):428–433. doi: 10.1159/000045215. [DOI] [PubMed] [Google Scholar]
- 166.Rostaing L, Chatelut E, Payen JL, et al. Pharmacokinetics of alphaIFN-2b in chronic hepatitis C virus patients undergoing chronic hemodialysis or with normal renal function: clinical implications. Journal of the American Society of Nephrology. 1998;9(12):2344–2348. doi: 10.1681/ASN.V9122344. [DOI] [PubMed] [Google Scholar]
- 167.Martin P, Carter D, Fabrizi F, et al. Histopathological features of hepatitis C in renal transplant candidates. Transplantation. 2000;69(7):1479–1484. doi: 10.1097/00007890-200004150-00045. [DOI] [PubMed] [Google Scholar]
- 168.Werner T, Aqel B, Balan V, et al. Treatment of hepatitis C in renal transplantation candidates: a single-center experience. Transplantation. 2010;90:407–411. doi: 10.1097/TP.0b013e3181e72837. [DOI] [PubMed] [Google Scholar]
- 169.Cruzado M, Casanovas-Taltavull T, Torras J, Baliellas C, Gil-Vernet S, Grinyo JM. Pretransplant interferon prevents hepatitis C virus-associated glomerulonephritis in renal allografts by HCV RNA clearance. American Journal of Transplantation. 2003;3(3):357–360. doi: 10.1034/j.1600-6143.2003.00057.x. [DOI] [PubMed] [Google Scholar]
- 170.Gursoy M, Guvener N, Koksal R, et al. Impact of HCV infection on development of posttransplantation diabetes mellitus in renal allograft recipients. Transplantation Proceedings. 2006;32(3):561–562. doi: 10.1016/s0041-1345(00)00890-3. [DOI] [PubMed] [Google Scholar]
- 171.Rostaing L, Izopet J, Baron E, Duffaut M, Puel J, Durand D. Treatment of chronic hepatitis C with recombinant alpha in kidney transplant recipients. Transplantation. 1995;59(10):1426–1431. doi: 10.1097/00007890-199505270-00012. [DOI] [PubMed] [Google Scholar]
- 172.Tang S, Cheng IK, Leung VK, et al. Successful treatment of hepatitis C after kidney transplantation with combined interferon alpha 2b and ribavirin. Journal of Hepatology. 2003;39(5):875–878. doi: 10.1016/s0168-8278(03)00358-1. [DOI] [PubMed] [Google Scholar]
- 173.Shu KH, Lan JL, Wu MJ, et al. Ultralow-dose alpha-interferon plus ribavirin for the treatment of active hepatitis C in renal transplant recipients. Transplantation. 2004;77(12):1894–1905. doi: 10.1097/01.tp.0000131151.07818.d7. [DOI] [PubMed] [Google Scholar]
- 174.Fabrizi F, Lunghi G, Dixit V, Martin P. Meta-analysis: antiviral therapy of hepatitis C virus-related liver disease in renal transplant patients. Alimentary Pharmacology and Therapeutics. 2006;24(10):1413–1422. doi: 10.1111/j.1365-2036.2006.03151.x. [DOI] [PubMed] [Google Scholar]
- 175.Shindo M, Di Bisceglie AM, Hoofnagle JH. Acute exacerbation of liver disease during interferon alfa therapy for chronic hepatitis C. Gastroenterology. 1992;102(4):1406–1408. [PubMed] [Google Scholar]
- 176.Kisseleva T, Bhattacharya S, Braunstein J, Schindler CW. Signaling through the JAK/STAT pathway, recent advances and future challenges. Gene. 2002;285(1-2):1–24. doi: 10.1016/s0378-1119(02)00398-0. [DOI] [PubMed] [Google Scholar]
- 177.Feld JJ, Hoofnagle JH. Mechanism of action of interferon and ribavirin in treatment of hepatitis C. Nature. 2005;436(7053):967–972. doi: 10.1038/nature04082. [DOI] [PubMed] [Google Scholar]
- 178.Fitzgerald-Bocarsly P, Feng D. The role of type I interferon production by dendritic cells in host defense. Biochimie. 2007;89(6-7):843–855. doi: 10.1016/j.biochi.2007.04.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 179.Papo T, Piette JC, Du LT, Godeau P. Interferon-alpha and autoimmunity. Annales de Medecine Interne (Paris) 1993;144(5):357–366. [PubMed] [Google Scholar]
- 180.Todros L, Saracco G, Durazzo M, et al. Efficacy and safety of interferon alfa therapy in chronic hepatitis C with autoantibodies to liver-kidney microsomes. Hepatology. 1995;22(5):1374–1378. [PubMed] [Google Scholar]
- 181.Garcia-Buey L, Garcia-Monzon C, Rodriguez S, et al. Latent autoimmune hepatitis triggered during interferon therapy in patients with chronic hepatitis C. Gastroenterology. 1995;108(6):1770–1777. doi: 10.1016/0016-5085(95)90139-6. [DOI] [PubMed] [Google Scholar]
- 182.Magnone M, Holley JL, Shapiro R, et al. Interferon-alpha-induced acute renal allograft rejection. Transplantation. 1995;59(7):1068–1070. doi: 10.1097/00007890-199504150-00030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 183.Rostaing L, Modesto A, Baron E, Cisterne JM, Chabannier MH, Durand D. Acute renal failure in kidney transplant patients treated with interferon alpha 2b for chronic hepatitis C. Nephron. 1996;74(3):512–516. doi: 10.1159/000189444. [DOI] [PubMed] [Google Scholar]
- 184.Kamar N, Rostaing L, Sandres-Saune K, Ribes D, Durand D, Izopet J. Amantadine therapy in renal transplant patients with hepatitis C virus infection. Journal of Clinical Virology. 2004;30(1):110–114. doi: 10.1016/j.jcv.2003.10.001. [DOI] [PubMed] [Google Scholar]
- 185.Fontaine H, Vallet-Pichard A, Equi-Andrade C, et al. Histopathological efficacy of ribavirin monotherapy in kidney allograft recipients with chronic hepatitis C. Transplantation. 2004;78(6):853–857. doi: 10.1097/01.tp.0000128911.87538.aa. [DOI] [PubMed] [Google Scholar]
- 186.Kamar N, Sandres-Saune K, Selves J, et al. Long-term ribavirin therapy in hepatitis C virus-positive renal transplant patients: effects on renal function and liver histology. American Journal of Kidney Diseases. 2003;42(1):184–192. doi: 10.1016/s0272-6386(03)00422-0. [DOI] [PubMed] [Google Scholar]
- 187.Calanca LN, Fehr T, Jochum W, et al. Combination therapy with ribavirin and amantadine in renal transplant patients with chronic hepatitis C virus infection is not superior to ribavirin alone. Journal of Clinical Virology. 2007;39(1):54–58. doi: 10.1016/j.jcv.2007.02.006. [DOI] [PubMed] [Google Scholar]
- 188.Davis CL, Feng S, Sung R, et al. Simultaneous liver-kidney transplantation: evaluation to decision making. American Journal of Transplantation. 2007;7(7):1702–1709. doi: 10.1111/j.1600-6143.2007.01856.x. [DOI] [PubMed] [Google Scholar]
- 189.Locke JE, Warren DS, Singer AL, et al. Declining outcomes in simultaneous liver-kidney transplantation in the MELD era: ineffective usage of renal allografts. Transplantation. 2008;85(7):935–942. doi: 10.1097/TP.0b013e318168476d. [DOI] [PubMed] [Google Scholar]
- 190.Gonwa TA, McBride MA, Anderson K, Mai ML, Wadei H, Ahsan N. Continued influence of preoperative renal function on outcome of orthotopic liver transplant (OLTX) in the US: where will MELD lead us? American Journal of Transplantation. 2006;6(11):2651–2659. doi: 10.1111/j.1600-6143.2006.01526.x. [DOI] [PubMed] [Google Scholar]
- 191.Campbell MS, Kotlyar DS, Brensinger CM, et al. Renal function after orthotopic liver transplantation is predicted by duration of pretransplantation creatinine elevation. Liver Transplantation. 2005;11(9):1048–1055. doi: 10.1002/lt.20445. [DOI] [PubMed] [Google Scholar]
- 192.Cohen AJ, Stegall MD, Rosen CB, et al. Chronic renal dysfunction late after liver transplantation. Liver Transplantation. 2002;8(10):916–921. doi: 10.1053/jlts.2002.35668. [DOI] [PubMed] [Google Scholar]
- 193.Marik PE, Wood K, Starzl TE. The course of type 1 hepato-renal syndrome post liver transplantation. Nephrology Dialysis Transplantation. 2006;21(2):478–482. doi: 10.1093/ndt/gfi212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 194.Pawarode A, Fine DM, Thuluvath PJ. Independent risk factors and natural history of renal dysfunction in liver transplant recipients. Liver Transplantation. 2003;9(7):741–747. doi: 10.1053/jlts.2003.50113. [DOI] [PubMed] [Google Scholar]
- 195.Eason JD, Gonwa TA, Davis CL, Sung RS, Gerber D, Bloom RD. Proceedings of consensus conference on simultaneous liver kidney transplantation (SLK) American Journal of Transplantation. 2008;8(11):2243–2251. doi: 10.1111/j.1600-6143.2008.02416.x. [DOI] [PubMed] [Google Scholar]
- 196.Schmitt TM, Kumer SC, Al-Osaimi A, et al. Combined liver-kidney and liver transplantation in patients with renal failure outcomes in the MELD era. Transplant International. 2009;22(9):876–883. doi: 10.1111/j.1432-2277.2009.00887.x. [DOI] [PubMed] [Google Scholar]
- 197.Fong TL, Bunnapradist S, Jordan SC, et al. Analysis of the united network for organ sharing database comparing renal allografts and patient survival in combined liver-kidney transplantation with the contralateral allografts in kidney alone or kidney-pancreas transplantation. Transplantation. 2003;76(2):348–353. doi: 10.1097/01.TP.0000071204.03720.BB. [DOI] [PubMed] [Google Scholar]
- 198.Simpson N, Cho YW, Cicciarelli JC, et al. Comparison of renal allograft outcomes in combined liver-kidney transplantation versus subsequent kidney transplantation in liver transplant recipients: analysis of UNOS database. Transplantation. 2006;82(10):1298–1303. doi: 10.1097/01.tp.0000241104.58576.e6. [DOI] [PubMed] [Google Scholar]
- 199.Al Riyami D, Alam A, Badovinac K, Ivis F, Trpeski L, Cantarovich M. Decreased survival in liver transplant patients requiring chronic dialysis: a Canadian experience. Transplantation. 2008;85(9):1277–1280. doi: 10.1097/TP.0b013e31816c4e6b. [DOI] [PubMed] [Google Scholar]
- 200.Ruiz R, Kunitake H, Wilkinson AH. Longterm analysis of combined liver—kidney transplantation at a single center. Archives of Surgery. 2006;141(8):735–741. doi: 10.1001/archsurg.141.8.735. [DOI] [PubMed] [Google Scholar]
- 201.Thompson JA, Lake JR. Review of hepatitis C in liver transplantation. Transplantation Updates. 2008;2:3–12. [Google Scholar]
- 202.Pascual M, Thadhani R, Chung RT, et al. Nephrotic syndrome after liver transplantation in a patient with hepatitis C virus-associated glomerulonephritis. Transplantation. 1997;64(7):1073–1076. doi: 10.1097/00007890-199710150-00022. [DOI] [PubMed] [Google Scholar]
- 203.Kamar N, Izopet J, Alric L, et al. Hepatitis C virus related kidney disease: an overview. Clinical Nephrology. 2008;69(3):149–160. doi: 10.5414/cnp69149. [DOI] [PubMed] [Google Scholar]
- 204.Abrahamian GA, Cosimi AB, Farrell ML, et al. Prevalence of hepatitis C virus-associated mixed cryoglobulinemia after liver transplantation. Liver Transplantation. 2000;6(2):185–190. doi: 10.1002/lt.500060224. [DOI] [PubMed] [Google Scholar]
- 205.Kendrick EA, McVicar JP, Kowdley KV, et al. Renal disease in hepatitis C-positive liver transplant recipients. Transplantation. 1997;63(9):1287–1293. doi: 10.1097/00007890-199705150-00016. [DOI] [PubMed] [Google Scholar]
- 206.Ghafari A, Sanadgol H. Impact of hepatitis B and hepatitis C virus infections on patients and allograft outcomes in renal transplant recipients: a single center study. Transplantation Proceedings. 2008;40(1):196–198. doi: 10.1016/j.transproceed.2007.12.006. [DOI] [PubMed] [Google Scholar]
- 207.Savas N, Ocal S, Colak T, Karakayali H, Yilmaz U, Haberal M. Clinical course of hepatitis C virus infection in renal transplant recipients. Transplantation Proceedings. 2007;39(4):984–986. doi: 10.1016/j.transproceed.2007.02.047. [DOI] [PubMed] [Google Scholar]
- 208.Del Pozo AC, Martìn JDR, Rodriguez-Laiz G, et al. Outcome of combined liver and kidney transplantation inhepatitis C: a single-center long-term follow-up experience. Transplantation Proceedings. 2009;41(5):1713–1716. doi: 10.1016/j.transproceed.2009.02.103. [DOI] [PubMed] [Google Scholar]
- 209.van Wagner LB, Baker T, Ahya SN, Norvell JP, Wang E, Levitsky J. Outcomes of patients with hepatitis C undergoing simultaneous liver-kidney transplantation. Journal of Hepatology. 2009;51(5):874–880. doi: 10.1016/j.jhep.2009.05.025. [DOI] [PubMed] [Google Scholar]
- 210.Port FK, Bragg-Gresham JL, Metzger RA, et al. Donor characteristics associated with reduced graft survival: an approach to expanding the pool of kidney donors. Transplantation. 2002;74(9):1281–1286. doi: 10.1097/00007890-200211150-00014. [DOI] [PubMed] [Google Scholar]
- 211.Durlik M, Gaciong Z, Rowinska D, et al. Long-term results of treatment of chronic hepatitis B, C and D with interferon-alpha in renal allograft recipients. Transplant International. 1998;11(supplement 1):S135–S139. doi: 10.1007/s001470050445. [DOI] [PubMed] [Google Scholar]
- 212.Calne RY, Davis DR, Hadjiyannakis E, et al. Immunosuppressive effects of soluble cell membrane fractions, donor blood and serum on renal allograft survival. Nature. 1970;227(5261):903–906. doi: 10.1038/227903a0. [DOI] [PubMed] [Google Scholar]
- 213.Montalbano M, Pasulo L, Sonzogni A, Remuzzi G, Colledan M, Strazzabosco M. Treatment with pegylated interferon and ribavirin for hepatitis C virus-associated severe cryoglobulinemia in a liver/kidney transplant recipient. Journal of Clinical Gastroenterology. 2007;41(2):216–220. doi: 10.1097/01.mcg.0000225569.04773.8b. [DOI] [PubMed] [Google Scholar]
- 214.Mukherjee S, Ariyarantha K. Successful hepatitis C eradication with preservation of renal functionin a liver/kidney recipient using pegylated interferon and ribavirin. Transplantation. 2007;84(10):1374–1375. doi: 10.1097/01.tp.0000289996.37615.7d. [DOI] [PubMed] [Google Scholar]
- 215.Schmitz V, Kiessling A, Bahra M, et al. Peginterferon alfa-2b plus ribavirin for the treatment of hepatitis C recurrence following combined liver and kidney transplantation. Annals of Transplantation. 2007;12(3):22–27. [PubMed] [Google Scholar]