

Abstract
Consideration of specific pediatric aspects is essential to achieve adequate peritoneal dialysis (PD) treatment in children. These are first of all the rapid growth, in particular during infancy and puberty, which must be accompanied by a positive calcium balance, and the age dependent changes in body composition. The high total body water content and the high ultrafiltration rates required in anuric infants for adequate nutrition predispose to overshooting convective sodium losses and severe hypotension. Tissue fragility and rapid increases in intraabdominal fat mass predispose to hernia and dialysate leaks. Peritoneal equilibration tests should repeatedly been performed to optimize individual dwell time. Intraperitoneal pressure measurements give an objective measure of intraperitoneal filling, which allow for an optimized dwell volume, that is, increased dialysis efficiency without increasing the risk of hernias, leaks, and retrofiltration. We present the concept of adapted PD, that is, the combination of short dwells with low fill volume to promote ultrafiltration and long dwells with a high fill volume to improve purification within one PD session. The use of PD solutions with low glucose degradation product content is recommended in children, but unfortunately still not feasible in many countries.
1. Introduction
Peritoneal dialysis (PD) is increasingly applied around the globe; newborns and even preterm children with a body weight of as little as 1500 g are meanwhile included in the chronic PD program. Whereas initial prognosis is often determined by acute comorbidities, such as neonatal complications and diseases associated with hereditary syndromes, long-term outcome is essentially determined by adequate control of uremia-related sequelae, mainly bone mineral disease and cardiovasculopathy [1]. Dietary and life style changes are difficult to procure. Individually tailored, optimized PD regimes, considering specific pediatric aspects, are therefore essential to achieve an improved long-term outcome of patients with pediatric onset of dialysis.
2. Specific Pediatric Aspects
A salient feature of children is the rapid somatic and psychomotor development in the first years of life and during puberty. Growth rate reaches 20 cm during the first and 15 cm during the second year of life. Body length is doubled within four years. This requires careful and repeated adaptation of the PD regime to body size and of protein, energy, and mineral supply. Total body calcium content is 25 g in newborns and increases to 1 kg until adulthood. Insufficient calcium supply and hyperparathyroidism interfere with the growth plate mineralization process and potentially result in epiphyseal slipping and severe deformities. Thus, despite all concerns regarding cardiovascular calcifications, a positive calcium balance is mandatory in growing children. Energy supply should be 100% of the dietary reference intake adapted to age, body mass index (BMI) and physical activity, protein intake 100% (adapted to ideal body weight), and an additional compensation for dialytic protein and amino acid losses [2].
Body composition also differs considerably in children as compared to adults. Water content is 75% in newborns, 60% in adolescents, and only 50% in elderly man. 40% of CKD5d children have hypodysplastic kidneys associated with polyuria. Dehydration is more likely to occur, especially in association with gastroenteritis. On the other hand, infants with little urine output need much higher ultrafiltration (UF) rate per square meter body surface area (BSA) as compared to adults to achieve adequate nutrition. Adequate nutrition is essential for normal physical and psychomotor development. In such children UF-related convective solute transport is considerable. While calcium may be supplied in sufficient amounts with calcium containing phosphate binders and high calcium dialysate concentrations, additional oral sodium chloride supply is often required to prevent a reduced body sodium content, hypotension, and associated neurological sequelae.
Successful insertion of a Tenckhoff catheter in newborns and infants is challenging, since the catheter is relatively larger and the peritoneal wall is thin and fragile. This readily explains the markedly increased risk of hernia and leakage in this age group [3, 4]. Moreover, rapid changes in body mass index and intraperitoneal fat mass and thus in intraperitoneal pressure occur during infancy [5] and further promote dialysis leak development.
In face of the good long-term prognosis of pediatric CKD5d patients as compared to adults [1, 6] with survival far into adulthood and the need of renal replacement therapy for many decades, the option to choose PD later in life should be maintained as long as possible. Prevention of peritoneal infections and inflammation and optimized PD biocompatibility are of particular importance to preserve long-term peritoneal membrane function.
3. Initiation of PD
To allow for sufficient healing of the PD catheter into the abdominal wall, early catheter implantation is advised. If possible, initiation of PD should be withheld for one to two weeks. Prophylactic herniotomy is often performed in newborns, omentectomy in most of the children to prevent catheter obstruction. Based on the clinical observation that catheter obstructions develop quite frequently even with curled catheters, the omentum should be removed as much as it is accessible during the insertion procedure. Preoperative treatment of constipation and adequate postoperative analgesia mitigate intraabdominal pressure peaks [7]. To safely increase the dwell volume postoperatively, intraperitoneal pressure (IPP) measurements should be performed [7]. An initial Peritoneal Equilibration Test (PET) is required to determine the optimal dwell time. In case these tests cannot be performed, PD should be started with 10 mL/kg body weight for 5–7 days after catheter insertion. The dwell volume should subsequently be increased to about 1100 mL/m² BSA within one week in children above 1 year and to 600 to a maximum of 800 mL in children below 1 year of age. BMI, organomegaly, and malnutrition increase the risk of hernia and leakage.
4. Defining Dwell Time According to PET
The PET is a standardized measure of the transperitoneal solute transport rates and ultrafiltration. It is performed with 1100 mL/m2 BSA of PD fluid containing 2.5% glucose [8]. A short PET of 2 hours yields similar results as a 4-hour PET in children [9]. The biocompatibility of PD fluids does not impact on PET findings to a major extend [10, 11]. PET performed with 4.2% of glucose gives a more accurate estimate of UF and of sodium sieving. Sodium sieving is a measure of AQP-1 function and thus glucose driven free water transport, which mainly occurs during the early phase of a dwell [12].
The peritoneal permeability of the patient, as assessed by a PET, should impact on dialysis prescription, especially on dwell duration. A low transporter status in the PET indicates low purification rates and potential difficulties to achieve creatinine clearance (CrCl) and Kt/V targets but good ultrafiltration even with long dwell times. In these children, the number of cycles can be low whereas total daily dialysis duration should be long to achieve sufficient clearance rates. An additional long exchange may be required, for example, during day time in cycling PD patients with a high solute and toxin load.
High and especially very high solute transport rates in the PET imply good purification, which however is associated with rapid glucose absorption and thus dissipation of the osmotic gradient required for ultrafiltration. Short dwell times and increased peritoneal glucose exposure are usually required to achieve sufficient water removal. In particular anuric patients with rapid solute transport need a high dialysate glucose concentration and frequent exchanges. The high peritoneal glucose exposure induces progressive peritoneal neoangiogenesis and thus further acceleration of glucose uptake. A vicious circle ultimately results in ultrafiltration failure [13]. Icodextrin should be considered to halt peritoneal membrane degradation [14]. Of note, frequent short dwells with a high glucose concentration result in a high amount of free water transport, which predominantly reduces water overload but only to a smaller extent salt excess. An increase in dwell time and of total dialysis time per day may be required to normalize blood pressure.
In adults a higher transport status has been associated with a worse survival [15]. In children higher peritoneal transport kinetics have been associated with higher CrP and lower serum albumin levels [16] and with reduced longitudinal growth [17]. Patients presenting with a high transporter status at PD onset appear to be less suited for chronic PD [15, 18–20], this however has not been confirmed consistently [21, 22] and may rather be a reflection of comorbidity than a problem with PD per se [23–25].
5. Intraperitoneal Pressure: A Measure of Optimized Dwell Volume
Since body size changes rapidly in children, frequent adaptation of dwell volume is required. This can best be performed by determination of the intraperitoneal pressure. IPP gives an objective measure of the individual intraperitoneal filling and thus allows for an optimization of the individual dwell volume. The measurement is easy to perform, which provided a sufficient cooperation of the child [7, 27]. IPP increases with BMI and organ size [7] (Figure 1). The latter is especially relevant in children with organomegaly, for example, in children with autosomal recessive kidney disease. Likewise, abdominal pain and constipation increase IPP [7]. Pitfalls of the measurements include inadequate pressure transmission, which can be evaluated from the respiration-dependent oscillations of the fluid level, and a filled bladder. Biocompatible PD solutions reduce IPP by 15–20% [28]. Abdominal pain is not reported below 12 cm H2O. IPP is usually acceptable up to 13-14 cm H2O, which corresponds to a mean fill volume of 1400 mL/m² (Figure 2). In children below 2 years of age IPP should not be above 8–10 cm H2O, that is, in most cases fill volume not above 800 mL/m² [29]. Otherwise the risk of hernia and leakage increases considerably in infants.
Figure 1.
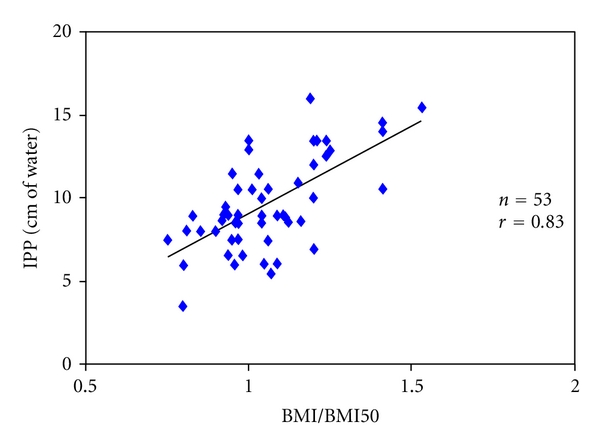
IPP is an individual patient characteristic, determined by BMI and dwell volume. The intraperitoneal pressure (IPP, y-axis) is positively correlated with the normalized body mass index (x-axis) within the general population. This correlation is even stronger than the correlation between dwell volume to IPP [5].
Figure 2.

Intraperitoneal pressure (mean/SD) according to dwell volume in children on PD above two years of age [7, 26]. In infants IPP should be below 8–10 cm, in children below 13-14 cm H2O. The red arrows give an example of how dwell volumes can be increased in patients with low IPP.
Of note, there are no clinical trials systematically evaluating the validity of IPP measurements. Extended clinical experience in pediatric dialysis centres, however, suggests that IPP is a suitable measure of abdominal filling and thus of the ratio of the wetted and functionally active peritoneal surface area to the anatomical surface area.
According to computed tomography analyses [30], the peritoneal surface area that is in contact with the dialysate is only 30 to 60% of the anatomic area. A larger fraction of the membrane can be recruited for exchange in the supine as compared to the upright position (which argues in favor of APD during the night) and with larger fill volumes. In fact, optimisation of the individual dwell volume may substantially increase the delivered dialysis dose. In the majority of children with an average fill volume of 800–1000 mL/m² BSA, an increase in fill volume of 30–50% is feasible (Figure 2). Such increases in fill volume should improve purification, for example, of phosphate and thus yield far reaching beneficial effects. Dialytic phosphate removal is highly correlated with total PD fluid turnover [31] and thus the cumulative phosphate load, a major cause of cardiovascular calcifications [1].
Calculations of the total pore area over diffusion distance (A0/ΔX) based on the three pore model of peritoneal transport in relation to the dwell volume support this notion.
Augmentation of the dwell volume from 800 to 1400 mL/m² increases A0/ΔX and thus the peritoneal surface recruited for purification by 20% [29, 32]. Still, smaller fill volumes must be prescribed in infants, at initiation of dialysis, in patients with history of leaks or hernia, and in patients reporting discomfort.
Other potential beneficial aspects of repeated IPP measurements are the reduction in back filtration, which should improve the ultrafiltration rates per gram of glucose infused, and a lower incidence of hernia and dialysate leaks. These observations, however, await scientific reconfirmation in clinical trials. In adults IPP levels above 14 cm have been shown to increase the risk of peritonitis [33].
Since the peritoneal membrane, that is, the anatomic peritoneal surface area, is proportional to BSA and not to body weight, scaling the dwell volume must be performed according to BSA. Scaling according to body weight resulted in an inappropriately low dwell volume especially in infants and young children and thus in the false perception of a peritoneal membrane inherent hyperpermeability in this age group in the past [34, 35]. On the other hand, keeping the fill volume below the limits of IPP of 8–10 cm H2O (800 mL/m²) as suggested for the children below 2 years of age results in a functional hyperpermeability as compared to older children [34]. To achieve sufficient ultrafiltration in neonates and infants, more frequent and shorter dwells must be applied to compensate for the functional hyperpermeability with faster glucose absorption [35].
6. The Concept of Adapted PD (APD)
APD is classically prescribed as repeated exchanges, each of them having the same duration and fill volume [36]. As given above, modification of the dwell time impacts on dialysis efficiency, both in terms of UF and purification. The Accelerated Peritoneal Examination (APEX) time defined by the crossing point of the urea and glucose equilibration curves obtained from a standardized PET has been proposed to be the optimal dwell time in terms of UF capacity [37, 38] (Figure 3). Likewise, modification of the dwell volume impacts on peritoneal surface area recruitment and thus ultrafiltration and purification capacity. A large intraperitoneal fill volume should favor convective and diffusive toxin removal. A very large fill volume with a too high intraperitoneal pressure, however, may result in back filtration and reduced net ultrafiltration [7]. Conversely, a smaller fill volume should favor UF, due to the lower intraperitoneal pressure [29, 38]. We propose to apply these principles by sequential exchanges with short and longer dwell-time and small and larger fill volumes as the concept of APD (Figure 4). The short exchanges with a smaller fill volume and a lower IPP to maximize UF should be based on the individual APEX time, the long dwells being three to four times the APEX time [38], and a higher fill volume with a still tolerable IPP to promote toxin clearance. IPP should not exceed 18 cm H2O; close follow-up is required in children with IPP above 13 cm H2O. This concept of individually assigned PD prescription based on the individual clinical tolerance and on IPP has been shown to allow for improved dialysis efficiency both in terms of blood purification and in terms of water and sodium removal and thus blood pressure control in children [39] and adults [40]. Of note, enhanced dialysis efficiency is achieved with the same total amount of dialysate delivered and within the same total daily dialysis time as compared to a conventional PD session.
Figure 3.

Illustration of APEX time, the crossing point of dialytic urea appearance, and glucose disappearance curve. APEX time indicates the optimal dwell time for ultrafiltration (normal range: 18 to 71 minutes).
Figure 4.

Example of an adapted PD session. Short dwells of 45 minutes of dwell time (i.e., individual APEX time) with a small fill volume (800 mL/m2) favoring ultrafiltration by a high osmotic gradient at a low IPP are followed by long dwells (150 minutes; 3-4 times the APEX time) with a large fill volume (1500 mL/m2), to promote uremic toxin removal.
7. Fluid Homeostasis
Structural and functional abnormalities of the heart are highly prevalent among paediatric PD patients, with oligoanuria and hypertension being independent predictors [16]. To achieve adequate sodium, volume and blood pressure control, repeated determinations of body weight, blood pressure, nutritional sodium supply and serum electrolyte concentrations, and eventually urine- and effluent electrolyte concentrations are required. Single-frequency bioimpedance analysis indicates intraindividual changes in hydration status [41, 42]. Margins of error, however, are large when total body water is predicted and the method is not yet broadly applied. Multiple-frequency bioimpedance analysis seems to be a promising method [43], but it is not yet sufficiently evaluated in children.
While infants with residual renal function may require additional sodium and water supply, dietary restriction of sodium and water intake is needed in many of the older children. The latter, however, is difficult to implement in the daily life. PD-associated water and sodium removal therefore plays a key role in maintaining euvolemia and normal body sodium content. In mice 50% of total UF occurs via aquaporin 1 (AQP-1) [44]. In humans treated with short dwells free water transport via AQP-1 is high, while water and convective solute removal via small pores predominates with long dwells. In adults 100 mmol of sodium are removed per litre of ultrafiltrate with a long, 4-hour dwell. About 80 mmol of sodium are removed per litre of ultrafiltrate during APD [45]. In children UF-associated sodium losses may even be high due to the relative lower fill volume per BSA and the associated functional hyperpermeability. Further sodium removal can be achieved with an additional day time exchange, in particular when icodextrin solutions are used [46].
All PD fluids currently available have a sodium concentration of 132–134 mmol/L. Reducing dialysate sodium concentration from 115 to 126 mmol/L and increasing glucose concentrations to up to 2.5% to maintain dialysate osmolality substantially increase sodium removal. Pioneering studies in adults have demonstrated promising effects on blood pressure and fluid status [47, 48]. These PD solutions, however, have not yet been admitted to the market and have not yet been investigated in children.
Insufficient, membrane-related ultrafiltration may have the following causes:
limited availability of membrane surface due to postoperative and post-infectious adhesions as well as fibrotic and sclerotic transformation of the membrane increasing the interstitial space,
high lymphatic and extra lymphatic absorption rates, for example, due to a high IPP,
impaired aquaporin 1 function, as suggested by the lack of sodium dipping,
increased vascular surface area due to acute and chronic hyperperfusion observed with inflammation and neoangiogenesis.
Preventive measures include atraumatic operations, postoperative addition of heparin to the dialysate [49], and above all prevention of peritonitis episodes by implementing respective standards of care and semiautomated connection devices. Impairment of aquaporin 1 function and peritoneal membrane transformation are related to PD fluid bioincompatibility and treatment time [50].
8. Improving PD Biocompatibility
PD has been performed with first generation single chamber PD solutions for several decades. They, however, contain high amounts of glucose and toxic glucose degradation products (GDPs) and expose the patient to supraphysiological lactate concentrations at an unphysiologically low pH. These PD solutions impair peritoneal mesothelial cell function and local host defence [51, 52] and lead to profound alterations of PD membrane morphology and function within few years [50, 53].
Several new PD solutions have meanwhile been introduced, which have the potential to substantially improve PD therapy in children. Separation of the glucose at a very low pH in multichamber bags markedly reduces GDP formation by 50 to more than 90% [54, 55], depending on the manufacturer. The pH of these double and triple chamber solutions is neutral to physiological pH; the buffer compound consists of lactate, bicarbonate, or a mixture of both. Numerous in vitro and animal studies demonstrate an improved biocompatibility profile [52, 56, 57]. Lactate-related in vitro toxicity improves at a physiological pH but does not normalize [58, 59]. In humans, prospective randomized trials demonstrate similar solute transport and ultrafiltration capacity with multichamber as compared to conventional PD solutions [10, 11, 60, 61]. Effluent surrogate markers of biocompatibility improve [11, 60, 62, 63]; residual renal function is better preserved, provided that it is not very low, that is, below 2 mL/minutes∗1.73 m² [64, 65]. Switch from conventional to low GDP solutions results in a peritoneal washout of AGE [66, 67] and a 15% decline in systemic AGE levels in children [68] and adults [62]. Two large-scale registries demonstrate significant improvement of patient morbidity and mortality in adults using multichamber as compared to conventional fluids [69, 70]. In face of the plethora of positive scientific evidence, multichamber PD solutions have meanwhile been advocated as standard of care in children treated in countries where these solutions are available [71]. General recommendations with regard to the choice of specific multichamber PD solutions cannot be given at present. Noteworthy, the beneficial effects associated with the introduction of new PD solutions may also be related to the simultaneous introduction of semiautomated connection devices, reducing the risk of touch contamination and thus of infectious complications. Likewise, PD surveillance has improved with cycler-based chip systems, monitoring daily PD performance in detail. The impact of these innovations, however, has not yet been analysed systematically.
Icodextrin solution is another useful option, in particular in children with sodium and water overload. The GDP content is reduced, lactate concentration is 40 mmol/L, and pH is still 5.5. The transperitoneal absorption rate is much lower than that of glucose; 40% of the icodextrin molecules are absorbed within 12-hours [72]. Icodextrin is metabolized to maltose and its derivatives; a clinical impact of maltose accumulation has not yet been discerned. Icodextrin induces iso-osmotic, colloid osmotic ultrafiltration, which is aquaporin-1 independent; that is, sodium sieving does not occur. Thus, icodextrin fluid is particularly suitable for children with impaired AQP-1 function and insufficient UF. It is administered during a single long dwell per day, that is, the day time dwell with APD. Icodextrin fluid has been reported to increase sodium removal and improve hydration status [73], blood pressure, and left ventricular mass [74], independent of the underlying transporter status [75]. Limitations regard allergic skin reactions to icodextrin and exfoliative dermatitis, observed in up to 10% of the patients. In addition, aseptic peritonitis outbreaks due to transient contamination with bacterial membrane compounds have repeatedly been noted with icodextrin [76, 77]. Due to interference with the assays, falsely increased plasma glucose determinations and falsely reduced total alpha-amylase activity may be observed with icodextrin use.
Amino acids are another osmotic alternative to glucose. Amino acid-based PD solutions contain very low amounts of GDP [78] and allow for a phosphate-free amino acid supply. Experimental studies, however, do not unequivocally support the notion of improved biocompatibility [57, 79, 80]. Solute and water transport is similar as compared to conventional, high GDP fluids [81, 82]. The limited anabolic effects of the relatively expensive solutions and the usual achievement of adequate nutrition with enteral feeding thus far have prevented wider administration of amino acid-based PD fluids in children, although the concept is intriguing. They are not yet recommended for parenteral nutrition in malnourished children [71].
In conclusion, the biocompatibility of the new generation of PD solutions is substantiated by numerous experimental and clinical studies. They provide evidence for major local and systemic benefits justifying their use in children. The associated increase in costs should be offset by reduced infectious complications [83, 84], improved long-term preservation of the PD membrane [57, 85], improved cardiovascular health [73, 85, 86], and improved long-term patient survival. Ultimate scientific evidence proving this assumption, however, is still missing. Large-scale randomized comparative trials are underway; an international pediatric peritoneal biopsy study evaluating the morphological and functional changes with standard and low GDP solutions is currently established.
9. Adequacy in Pediatric PD
Scientific data in children indicating that any of the measures of dialysis efficacy is predictive of well-being, morbidity, or mortality is absent and definition of PD adequacy is even more difficult than in adults. Adult targets of urea removal scaled to its volume of distribution (Kt/V) and clearance of creatinine have been implemented in pediatric PD. These measures, however, are a matter of debate. 2006 K/DOQI guidelines recommended a minimal total Kt/V of 1.8 [87]. To allow for sufficient dietary protein intake a Kt/V of 2.0 has been suggested for continuous ambulatory peritoneal dialysis (CAPD) patients [88]. Considering the much higher relative protein intake required in growing children per kg body weight [2], the Japanese Study Group of Pediatric PD even suggested a Kt/V of 2.5 or higher [89]. The adequate target Kt/V is yet unknown. At present a Kt/V of at least 2.1 and a total clearance of creatinine of 63 liters/week/1.73 m² are recommend in children on continuous cyclic peritoneal dialysis (CCPD). Other aspects such as the preservation of residual renal function are at least as important. This can be achieved by ACE inhibition and angiotensin receptor blockade [90], pediatric data however is scant, and a general recommendation on ACE and ARB use is not yet justified. In adults survival is closely related to residual renal function but not to Kt/V, provided that a lower limit of urea removal is maintained [91, 92]. In children growth correlates with renal but not with peritoneal solute clearance [93].
Kt/V is scaled to body weight, CrCl to BSA. Due to the relation of BW to BSA of 1 : 30 a ratio of Kt/V to CrCl of 1 : 30 has therefore been generally be recommended [36], even though small children and infants have a higher ratio of BSA to body weight. Kt/V targets are often easier to achieve than CrCl targets, in particular in anuric children, which require frequent cycles for ultrafiltration. Urea removal is more related to the number of cycles and dwell volume, CrCl more to PD duration [27]. Likewise, patients with a high peritoneal transporter status, either due to a hyperpermeable state of the peritoneum or due to a too low fill volume per BSA, have a relatively higher urea versus creatinine removal.
In view of these limitations, adequacy of pediatric PD is probably better described by the achievement of a normal water and electrolyte balance and thus normal blood pressure, by a minimal phosphate and toxin accumulation in a clinically asymptomatic child with growth and psychomotor development close to normal. This, of course, is difficult to achieve, especially in anuric children. A major step towards this goal is optimizing PD prescription by means of PET and IPP, allowing for individual adaptation of fill volume and dwell time. Too low fill volumes resulting in functional hyperpermeability and too large fill volumes resulting in back filtration, discomfort, and dialysate leaks can be avoided. Dwell time should be adapted to individual ultrafiltration and purification needs. This may be varied within one PD session. Administration of PD solutions with reduced local and systemic toxicity, consideration of the age specific needs of rapidly growing children, and continuous support of the families to reduce the burden of home dialysis therapy should further contribute to make adequate PD an achievable goal.
References
- 1.Oh J, Wunsch R, Turzer M, et al. Advanced coronary and carotid arteriopathy in young adults with childhood-onset chronic renal failure. Circulation. 2002;106(1):100–105. doi: 10.1161/01.cir.0000020222.63035.c0. [DOI] [PubMed] [Google Scholar]
- 2.KDOQI Work Group. KDOQI clinical practice guideline for nutrition in children with CKD: 2008 update. Executive summary. American Journal of Kidney Diseases. 2009;53(supplement 2):11–104. doi: 10.1053/j.ajkd.2008.11.017. [DOI] [PubMed] [Google Scholar]
- 3.Rinaldi S, Sera F, Verrina E, et al. The Italian registry of pediatric chronic peritoneal dialysis: a ten-year experience with chronic peritoneal dialysis catheters. Peritoneal Dialysis International. 1998;18(1):71–74. [PubMed] [Google Scholar]
- 4.Leblanc M, Ouimet D, Pichette V. Dialysate leaks in peritoneal dialysis. Seminars in Dialysis. 2001;14(1):50–54. doi: 10.1046/j.1525-139x.2001.00014.x. [DOI] [PubMed] [Google Scholar]
- 5.Fiscbach M, Terzic J, Provot E, et al. Intraperitoneal pressure in children: fill-volume related and impacted by body mass index. Peritoneal Dialysis International. 2003;23(4):391–394. [PubMed] [Google Scholar]
- 6.McDonald SP, Craig JC. Long-term survival of children with end-stage renal disease. New England Journal of Medicine. 2004;350(26):2654–2662. doi: 10.1056/NEJMoa031643. [DOI] [PubMed] [Google Scholar]
- 7.Fischbach M, Terzic J, Laugel V, Escande B, Dangelser C, Helmstetter A. Measurement of hydrostatic intraperitoneal pressure: a useful tool for the improvement of dialysis dose prescription. Pediatric Nephrology. 2003;18(10):976–980. doi: 10.1007/s00467-003-1199-9. [DOI] [PubMed] [Google Scholar]
- 8.Warady BA, Alexander SR, Hossli S, et al. Peritoneal membrane transport function in children receiving long-term dialysis. Journal of the American Society of Nephrology. 1996;7(11):2385–2391. doi: 10.1681/ASN.V7112385. [DOI] [PubMed] [Google Scholar]
- 9.Cano F, Sanchez L, Rebori A, et al. The short peritoneal equilibration test in pediatric peritoneal dialysis. Pediatric Nephrology. 2010;25(10):2159–2164. doi: 10.1007/s00467-010-1566-2. [DOI] [PubMed] [Google Scholar]
- 10.Schmitt CP, Haraldsson B, Doetschmann R, et al. Effects of pH-neutral, bicarbonate-buffered dialysis fluid on peritoneal transport kinetics in children. Kidney International. 2002;61(4):1527–1536. doi: 10.1046/j.1523-1755.2002.00255.x. [DOI] [PubMed] [Google Scholar]
- 11.Haas S, Schmitt CP, Arbeiter K, et al. Improved acidosis correction and recovery of mesothelial cell mass with neutral-pH bicarbonate dialysis solution among children undergoing automated peritoneal dialysis. Journal of the American Society of Nephrology. 2003;14(10):2632–2638. doi: 10.1097/01.asn.0000086475.83211.df. [DOI] [PubMed] [Google Scholar]
- 12.Pride ET, Gustafson J, Graham A, et al. Comparison of a 2.5% and a 4.25% dextrose peritoneal equilibration test. Peritoneal Dialysis International. 2002;22(3):365–370. [PubMed] [Google Scholar]
- 13.Davies SJ, Phillips L, Naish PF, Russell GI. Peritoneal glucose exposure and changes in membrane solute transport with time on peritoneal dialysis. Journal of the American Society of Nephrology. 2001;12(5):1046–1051. doi: 10.1681/ASN.V1251046. [DOI] [PubMed] [Google Scholar]
- 14.Davies SJ, Brown EA, Frandsen NE, et al. Longitudinal membrane function in functionally anuric patients treated with APD: data from EAPOS on the effects of glucose and icodextrin prescription. Kidney International. 2005;67(4):1609–1615. doi: 10.1111/j.1523-1755.2005.00243.x. [DOI] [PubMed] [Google Scholar]
- 15.Churchill DN, Thorpe KE, Nolph KD, Keshaviah PR, Oreopoulos DG, Pagé D. Increased peritoneal membrane transport is associated with decreased patient and technique survival for continuous peritoneal dialysis patients. Journal of the American Society of Nephrology. 1998;9(7):1285–1292. doi: 10.1681/ASN.V971285. [DOI] [PubMed] [Google Scholar]
- 16.Bakkaloglu SA, Saygili A, Sever L, et al. Impact of peritoneal transport characteristics on cardiac function in paediatric peritoneal dialysis patients: a Turkish Pediatric Peritoneal Dialysis Study Group (TUPEPD) report. Nephrology Dialysis Transplantation. 2010;25(7):2296–2303. doi: 10.1093/ndt/gfq027. [DOI] [PubMed] [Google Scholar]
- 17.Schaefer F, Klaus G, Mehls O. Peritoneal transport properties and dialysis dose affect growth and nutritional status in children on chronic peritoneal dialysis. Journal of the American Society of Nephrology. 1999;10(8):1786–1792. doi: 10.1681/ASN.V1081786. [DOI] [PubMed] [Google Scholar]
- 18.Wang T, Heimbürger O, Waniewski J, Bergström J, Lindholm B. Increased peritoneal permeability is associated with decreased fluid and small-solute removal and higher mortality in CAPD patients. Nephrology Dialysis Transplantation. 1998;13(5):1242–1249. doi: 10.1093/ndt/13.5.1242. [DOI] [PubMed] [Google Scholar]
- 19.Dasgupta MK, Perry D, Royer R, Fox S. Long-term survival and its relationship to membrane transport status in peritoneal dialysis. Advances in Peritoneal Dialysis. 2000;16:15–18. [PubMed] [Google Scholar]
- 20.Jager KJ, Merkus MP, Dekker FW, et al. Mortality and technique failure in patients starting chronic peritoneal dialysis: results of the Netherlands cooperative study on the adequacy of dialysis. Kidney International. 1999;55(4):1476–1485. doi: 10.1046/j.1523-1755.1999.00353.x. [DOI] [PubMed] [Google Scholar]
- 21.Brown EA, Davies SJ, Rutherford P, et al. Survival of functionally anuric patients on automated peritoneal dialysis: the European APD outcome study. Journal of the American Society of Nephrology. 2003;14(11):2948–2957. doi: 10.1097/01.asn.0000092146.67909.e2. [DOI] [PubMed] [Google Scholar]
- 22.Passadakis PS, Thodis ED, Panagoutsos SA, Selisiou CA, Pitta EM, Vargemezis VA. Outcome for continuous ambulatory peritoneal dialysis patients is not predicted by peritoneal permeability characteristics. Advances in Peritoneal Dialysis. 2000;16:2–6. [PubMed] [Google Scholar]
- 23.Balafa O, Halbesma N, Struijk DG, Dekker FW, Krediet RT. Peritoneal albumin and protein losses do not predict outcome in peritoneal dialysis patients. Clinical Journal of the American Society of Nephrology. 2011;6(3):561–566. doi: 10.2215/CJN.05540610. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Stenvinkel P, Chung SH, Heimbürger O, Lindholm B. Malnutrition, inflammation, and atherosclerosis in peritoneal dialysis patients. Peritoneal Dialysis International. 2001;21(3):S157–S162. [PubMed] [Google Scholar]
- 25.Kim SB, Chang JW, Lee SK, Park JS. Acute systemic inflammation is associated with an increase in peritoneal solute transport rate in chronic peritoneal dialysis patients. Peritoneal Dialysis International. 2004;24(6):597–600. [PubMed] [Google Scholar]
- 26.Rusthoven E, van der Vlugt ME, van Lingen-van Bueren LJ, et al. Evaluation of intraperitoneal pressure and the effect of different osmotic agents on intraperitoneal pressure in children. Peritoneal Dialysis International. 2005;25(4):352–356. [PubMed] [Google Scholar]
- 27.Fischbach M, Warady BA. Peritoneal dialysis prescription in children: bedside principles for optimal practice. Pediatric Nephrology. 2009;24(9):1633–1642. doi: 10.1007/s00467-008-0979-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Fischback M, Terzic J, Chauvé S, Laugel V, Muller A, Haraldsson B. Effect of peritoneal dialysis fluid composition on peritoneal area available for exchange in children. Nephrology Dialysis Transplantation. 2004;19(4):925–932. doi: 10.1093/ndt/gfg518. [DOI] [PubMed] [Google Scholar]
- 29.Fischbach M, Terzic J, Menouer S, Haraldsson B. Optimal volume prescription for children on peritoneal dialysis. Peritoneal Dialysis International. 2001;20(6):603–606. [PubMed] [Google Scholar]
- 30.Chagnac A, Herskovitz P, Ori Y, et al. Effect of increased dialysate volume on peritoneal surface area among peritoneal dialysis patients. Journal of the American Society of Nephrology. 2002;13(10):2554–2559. doi: 10.1097/01.asn.0000026492.83560.81. [DOI] [PubMed] [Google Scholar]
- 31.Schmitt CP, Borzych D, Nau B, Wühl E, Zurowska A, Schaefer F. Dialytic phosphate removal: a modifiable measure of dialysis efficacy in automated peritoneal dialysis. Peritoneal Dialysis International. 2009;29(4):465–471. [PubMed] [Google Scholar]
- 32.Fischbach M, Haraldsson B. Dynamic changes of the total pore area available for peritoneal exchange in children. Journal of the American Society of Nephrology. 2001;12(7):1524–1529. doi: 10.1681/ASN.V1271524. [DOI] [PubMed] [Google Scholar]
- 33.Dejardin A, Robert A, Goffin E. Intraperitoneal pressure in PD patients: relationship to intraperitoneal volume, body size and PD-related complications. Nephrology Dialysis Transplantation. 2007;22(5):1437–1444. doi: 10.1093/ndt/gfl745. [DOI] [PubMed] [Google Scholar]
- 34.Kohaut EC, Waldo FB, Benfield MR. The effect of changes in dialysate volume on glucose and urea equilibration. Peritoneal Dialysis International. 1994;14(3):236–239. [PubMed] [Google Scholar]
- 35.Fischbach M. Peritoneal dialysis prescription for neonates. Peritoneal Dialysis International. 1996;16(1):S512–S514. [PubMed] [Google Scholar]
- 36.Fischbach M, Stefanidis CJ, Watson AR. Guidelines by an ad hoc European committee on adequacy of the paediatric peritoneal dialysis prescription. Nephrology Dialysis Transplantation. 2002;17(3):380–385. doi: 10.1093/ndt/17.3.380. [DOI] [PubMed] [Google Scholar]
- 37.Fischbach M, Desprez P, Terzic J, Lahlou A, Mengus L, Geisert J. Use of intraperitoneal pressure, ultrafiltration and purification dwell times for individual peritoneal dialysis prescription in children. Clinical Nephrology. 1996;46(1):14–16. [PubMed] [Google Scholar]
- 38.Fischbach M, Lahlou A, Eyer D, Desprez P, Geisert J. Determination of individual ultrafiltration time (APEX) and purification phosphate time by peritoneal equilibration test: application to individual peritoneal dialysis modality prescription in children. Peritoneal Dialysis International. 1996;16(1):S557–S560. [PubMed] [Google Scholar]
- 39.Fischbach M, Desprez P, Donnars F, Hamel G, Geisert J. Optimization of CCPD prescription in children using peritoneal equilibration test. Advances in Peritoneal Dialysis. 1994;10:307–309. [PubMed] [Google Scholar]
- 40.Fischbach M, Issad B, Dubois V, Taamma R. The influence of varying the dwell time and fill volume on the effectiveness of automated peritoneal dialysis: a randomized controlled trial. doi: 10.3747/pdi.2010.00146. Peritoneal Dialysis International. In press. [DOI] [PubMed] [Google Scholar]
- 41.Edefonti A, Mastrangelo A, Paglialonga F. Assessment and monitoring of nutrition status in pediatric peritoneal dialysis patients. Peritoneal Dialysis International. 2009;29(2):S176–S179. [PubMed] [Google Scholar]
- 42.Wühl E, Fusch CH, Schärer K, Mehls O, Schaefer F. Assessment of total body water in paediatric patients on dialysis. Nephrology Dialysis Transplantation. 1996;11(1):75–80. [PubMed] [Google Scholar]
- 43.Demirci MS, Demirci C, Ozdogan O, et al. Relations between malnutrition-inflammation-atherosclerosis and volume status. The usefulness of bioimpedance analysis in peritoneal dialysis patients. Nephrology Dialysis Transplantation. 2011;26(5):1708–1716. doi: 10.1093/ndt/gfq588. [DOI] [PubMed] [Google Scholar]
- 44.Ni J, Verbavatz JM, Rippe A, et al. Aquaporin-1 plays an essential role in water permeability and ultrafiltration during peritoneal dialysis. Kidney International. 2006;69(9):1518–1525. doi: 10.1038/sj.ki.5000285. [DOI] [PubMed] [Google Scholar]
- 45.Rippe B, Venturoli D. Optimum electrolyte composition of a dialysis solution. Peritoneal Dialysis International. 2008;28(3):S131–S136. [PubMed] [Google Scholar]
- 46.Fourtounas C, Hardalias A, Dousdampanis P, Papachristopoulos B, Savidaki E, Vlachojannis JG. Sodium removal in peritoneal dialysis: the role of icodextrin and peritoneal dialysis modalities. Advances in Peritoneal Dialysis. 2008;24:27–31. [PubMed] [Google Scholar]
- 47.Nakayama M, Kasai K, Imai H. Novel low na peritoneal dialysis solutions designed to optimize na gap of effluent: kinetics of na and water removal. Peritoneal Dialysis International. 2009;29(5):528–535. [PubMed] [Google Scholar]
- 48.Davies S, Carlsson O, Simonsen O, et al. The effects of low-sodium peritoneal dialysis fluids on blood pressure, thirst and volume status. Nephrology Dialysis Transplantation. 2009;24(5):1609–1617. doi: 10.1093/ndt/gfn668. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Margetts P. Heparin and the peritoneal membrane. Peritoneal Dialysis International. 2009;29(1):16–19. [PubMed] [Google Scholar]
- 50.Williams JD, Craig KJ, Topley N, et al. Morphologic changes in the peritoneal membrane of patients with renal disease. Journal of the American Society of Nephrology. 2002;13(2):470–479. doi: 10.1681/ASN.V132470. [DOI] [PubMed] [Google Scholar]
- 51.Witowski J, Jörres A. Peritoneal dialysis: a biological membrane with a nonbiological fluid. Contributions to Nephrology. 2009;163:27–34. doi: 10.1159/000223777. [DOI] [PubMed] [Google Scholar]
- 52.Mortier S, Lameire NH, De Vriese AS. The effects of peritoneal dialysis solutions on peritoneal host defense. Peritoneal Dialysis International. 2004;24(2):123–138. [PubMed] [Google Scholar]
- 53.Yoshino A, Honda M, Fukuda M, et al. Changes in peritoneal equilibration test values during long-term peritoneal dialysis in peritonitis-free children. Peritoneal Dialysis International. 2001;21(2):180–185. [PubMed] [Google Scholar]
- 54.Frischmann M, Spitzer J, Fünfrocken M, et al. Development and validation of an HPLC method to quantify 3,4-dideoxyglucosone-3-ene in peritoneal dialysis fluids. Biomedical Chromatography. 2009;23(8):843–851. doi: 10.1002/bmc.1194. [DOI] [PubMed] [Google Scholar]
- 55.Erixon M, Wieslander A, Lindén T, et al. How to avoid glucose degradation products in peritoneal dialysis fluids. Peritoneal Dialysis International. 2006;26(4):490–497. [PubMed] [Google Scholar]
- 56.Topley N, Kaur D, Petersen MM, et al. Biocompatibility of bicarbonate buffered peritoneal dialysis fluids: influence on mesothelial cell and neutrophil function. Kidney International. 1996;49(5):1447–1456. doi: 10.1038/ki.1996.204. [DOI] [PubMed] [Google Scholar]
- 57.Mortier S, Faict D, Schalkwijk CG, Lameire NH, De Vriese AS. Long-term exposure to new peritoneal dialysis solutions: effects on the peritoneal membrane. Kidney International. 2004;66(3):1257–1265. doi: 10.1111/j.1523-1755.2004.00879.x. [DOI] [PubMed] [Google Scholar]
- 58.Plum J, Razeghi P, Lordnejad RM, et al. Peritoneal dialysis fluids with a physiologic pH based on either lactate or bicarbonate buffer-effects on human mesothelial cells. American Journal of Kidney Diseases. 2001;38(4):867–875. doi: 10.1053/ajkd.2001.27709. [DOI] [PubMed] [Google Scholar]
- 59.Ogata S, Mori M, Tatsukawa Y, Kiribayashi K, Yorioka N. Expression of vascular endothelial growth factor, fibroblast growth factor, and lactate dehydrogenase by human peritoneal mesothelial cells in solutions with lactate or bicarbonate or both. Advances in Peritoneal Dialysis. 2006;22:37–40. [PubMed] [Google Scholar]
- 60.Williams JD, Topley N, Craig KJ, et al. The Euro-Balance Trial: the effect of a new biocompatible peritoneal dialysis fluid (balance) on the peritoneal membrane. Kidney International. 2004;66(1):408–418. doi: 10.1111/j.1523-1755.2004.00747.x. [DOI] [PubMed] [Google Scholar]
- 61.Tranaeus A. A long-term study of a bicarbonate/lactate-based peritoneal dialysis solution—clinical benefits. Peritoneal Dialysis International. 2000;20(5):516–523. [PubMed] [Google Scholar]
- 62.Zeier M, Schwenger V, Deppisch R, et al. Glucose degradation products in PD fluids: do they disappear from the peritoneal cavity and enter the systemic circulation? Kidney International. 2003;63(1):298–305. doi: 10.1046/j.1523-1755.2003.00705.x. [DOI] [PubMed] [Google Scholar]
- 63.Rippe B, Simonsen O, Heimbürger O, et al. Long-term clinical effects of a peritoneal dialysis fluid with less glucose degradation products. Kidney International. 2001;59(1):348–357. doi: 10.1046/j.1523-1755.2001.00497.x. [DOI] [PubMed] [Google Scholar]
- 64.Kim SG, Kim S, Hwang Y-H, et al. Could solutions low in glucose degradation products preserve residual renal function in incident peritoneal dialysis patients? A 1-year multicenter prospective randomized controlled trial (Balnet study) Peritoneal Dialysis International. 2008;28:S117–S122. [PubMed] [Google Scholar]
- 65.Haag-Weber M, Krämer R, Haake R, et al. Low-GDP fluid (Gambrosol trio) attenuates decline of residual renal function in PD patients: a prospective randomized study. Nephrology Dialysis Transplantation. 2010;25(7):2288–2296. doi: 10.1093/ndt/gfq087. [DOI] [PubMed] [Google Scholar]
- 66.Ho-dac-Pannekeet MM, Weiss MF, De Waart DR, Erhard P, Hiralall JK, Krediet RT. Analysis of non enzymatic glycosylation in vivo: impact of different dialysis solutions. Peritoneal Dialysis International. 1999;19(2):S68–S74. [PubMed] [Google Scholar]
- 67.Posthuma N, Ter Wee PM, Niessen H, Donker AJM, Verbrugh HA, Schalkwijk CG. Amadori albumin and advanced glycation end-product formation in peritoneal dialysis using icodextrin. Peritoneal Dialysis International. 2001;21(1):43–51. [PubMed] [Google Scholar]
- 68.Schmitt CP, von Heyl D, Rieger S, et al. Reduced systemic advanced glycation end products in children receiving peritoneal dialysis with low glucose degradation product content. Nephrology Dialysis Transplantation. 2007;22(7):2038–2044. doi: 10.1093/ndt/gfm148. [DOI] [PubMed] [Google Scholar]
- 69.Han SH, Ahn SV, Yun JY, Tranaeus A, Han DS. Mortality and technique failure in peritoneal dialysis patients using advanced peritoneal dialysis solutions. American Journal of Kidney Diseases. 2009;54(4):711–720. doi: 10.1053/j.ajkd.2009.05.014. [DOI] [PubMed] [Google Scholar]
- 70.Lee HY, Choi HY, Park HC, et al. Changing prescribing practice in CAPD patients in Korea: increased utilization of low GDP solutions improves patient outcome. Nephrology Dialysis Transplantation. 2006;21(10):2893–2899. doi: 10.1093/ndt/gfl393. [DOI] [PubMed] [Google Scholar]
- 71.Schmitt CP, Sevcan A, Bakkaloglu SA, Günter K, Schröder C, Fischbach M. Solutions for PD in children—recommendations by the European pediatric dialysis working group. Pediatric Nephrology. 2011;26(7):1137–1147. doi: 10.1007/s00467-011-1863-4. [DOI] [PubMed] [Google Scholar]
- 72.Moberly JB, Mujais S, Gehr T, et al. Pharmacokinetics of icodextrin in peritoneal dialysis patients. Kidney International. 2002;62(81, supplement):S23–S33. doi: 10.1046/j.1523-1755.62.s81.5.x. [DOI] [PubMed] [Google Scholar]
- 73.Davies SJ, Woodrow G, Donovan K, et al. Icodextrin improves the fluid status of peritoneal dialysis patients: results of a double-blind randomized controlled trial. Journal of the American Society of Nephrology. 2003;14(9):2338–2344. doi: 10.1097/01.asn.0000083904.12234.27. [DOI] [PubMed] [Google Scholar]
- 74.Konings CJAM, Kooman JP, Schonck M, et al. Effect of icodextrin on volume status, blood pressure and echocardiographic parameters: a randomized study. Kidney International. 2003;63(4):1556–1563. doi: 10.1046/j.1523-1755.2003.00887.x. [DOI] [PubMed] [Google Scholar]
- 75.Finkelstein F, Healy H, Abu-Alfa A, et al. Superiority of icodextrin compared with 4.25% dextrose for peritoneal ultrafiltration. Journal of the American Society of Nephrology. 2005;16(2):546–554. doi: 10.1681/ASN.2004090793. [DOI] [PubMed] [Google Scholar]
- 76.Martis L, Patel M, Giertych J, et al. Aseptic peritonitis due to peptidoglycan contamination of pharmacopoeia standard dialysis solution. Lancet. 2005;365(9459):588–594. doi: 10.1016/S0140-6736(05)17908-2. [DOI] [PubMed] [Google Scholar]
- 77.Adam FU, Singan M, Ozelsancak R, Torun D, Ozdemir FN, Haberal M. Icodextrin-associated sterile peritonitis: a recent outbreak in Turkey. Peritoneal Dialysis International. 2007;27(5):598–599. [PubMed] [Google Scholar]
- 78.Schalkwijk CG, ter Wee PM, Teerlink T. Reduced 1,2-dicarbonyl compounds in bicarbonate/lactate-buffered peritoneal dialysis (PD) fluids and PD fluids based on glucose polymers or amino acids. Peritoneal Dialysis International. 2001;20(6):796–798. [PubMed] [Google Scholar]
- 79.Reimann D, Dachs D, Meye C, Gross P. Amino acid-based peritoneal dialysis solution stimulates mesothelial nitric oxide production. Peritoneal Dialysis International. 2004;24(4):378–384. [PubMed] [Google Scholar]
- 80.Tjiong HL, Zijlstra FJ, Rietveld T, et al. Peritoneal protein losses and cytokine generation in automated peritoneal dialysis with combined amino acids and glucose solutions. Mediators of Inflammation. 2007;2007 doi: 10.1155/2007/97272. Article ID 97272. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Qamar IU, Secker D, Levin L, Balfe JA, Zlotkin S, Balfe JW. Effects of amino acid dialysis compared to dextrose dialysis in children on continuous cycling peritoneal dialysis. Peritoneal Dialysis International. 1999;19(3):237–247. [PubMed] [Google Scholar]
- 82.Li FK, Chan LYY, Woo JCY, et al. A 3-year, prospective, randomized, controlled study on amino acid dialysate in patients on CAPD. American Journal of Kidney Diseases. 2003;42(1):173–183. doi: 10.1016/s0272-6386(03)00421-9. [DOI] [PubMed] [Google Scholar]
- 83.Montenegro J, Saracho R, Gallardo I, Martñnez I, Muñoz R, Quintanilla N. Use of pure bicarbonate-buffered peritoneal dialysis fluid reduces the incidence of CAPD peritonitis. Nephrology Dialysis Transplantation. 2007;22(6):1703–1708. doi: 10.1093/ndt/gfl848. [DOI] [PubMed] [Google Scholar]
- 84.Furkert JD, Zeier M, Schwenger V. Effects of Peritoneal dialysis solutions low in GDPs on peritonitis and exit-site infection rates. Peritoneal Dialysis International. 2008;28(6):637–640. [PubMed] [Google Scholar]
- 85.Bredie SJH, Bosch FH, Demacker PNM, Stalenhoef AFH, van Leusen R. Effects of peritoneal dialysis with an overnight icodextrin dwell on parameters of glucose and lipid metabolism. Peritoneal Dialysis International. 2001;21(3):275–281. [PubMed] [Google Scholar]
- 86.Babazono T, Nakamoto H, Kasai K, et al. Effects of icodextrin on glycemic and lipid profiles in diabetic patients undergoing peritoneal dialysis. American Journal of Nephrology. 2007;27(4):409–415. doi: 10.1159/000105123. [DOI] [PubMed] [Google Scholar]
- 87.Peritoneal Dialysis Adequacy Working Group. Clinical practice guidelines for peritoneal dialysis adequacy. American Journal of Kidney Disease. 2006;48(supplement 1):98–129. doi: 10.1053/j.ajkd.2006.04.006. [DOI] [PubMed] [Google Scholar]
- 88.Nolph KD, Popovich RP, Moncrief JW. Theoretical and practical implications of continuous ambulatory peritoneal dialysis. Nephron. 1978;21(3):117–122. doi: 10.1159/000181381. [DOI] [PubMed] [Google Scholar]
- 89.Honda M. Peritoneal dialysis prescription suitable for children with anuria. Peritoneal Dialysis International. 2008;28(3):S153–S158. [PubMed] [Google Scholar]
- 90.Akbari A, Knoll G, Ferguson D, McCormick B, Davis A, Biyani M. Angiotensin-converting enzyme inhibitors and angiotensin receptor blockers in peritoneal dialysis: systematic review and meta-analysis of randomized controlled trials. Peritoneal Dialysis International. 2009;29(5):554–561. [PubMed] [Google Scholar]
- 91.Amato D, Paniagua R. The ADEMEX study: afterthoughts. Peritoneal Dialysis International. 2003;23(4):313–316. [PubMed] [Google Scholar]
- 92.Bargman JM, Thorpe KE, Churchill DN. Relative contribution of residual renal function and peritoneal clearance to adequacy of dialysis: a reanalysis of the CANUSA study. Journal of the American Society of Nephrology. 2001;12(10):2158–2162. doi: 10.1681/ASN.V12102158. [DOI] [PubMed] [Google Scholar]
- 93.Chadha V, Blowey DL, Waraby BA. Is growth a valid outcome measure of dialysis clearance in children undergoing peritoneal dialysis? Peritoneal Dialysis International. 2001;21(3):S179–S184. [PubMed] [Google Scholar]