

Sir,
A 12-year-old boy presented with multiple raised lesions on his lower limbs of 2 years duration. The lesions started as a papule on the right leg, which increased in size, followed by occurrence of similar lesions in the right buttocks and the left knee. There was no history of cough with expectoration, weight loss, evening rise of temperature, blood tinged sputum, swellings in the neck/axillae or family history of tuberculosis. He was thin built; otherwise his systemic examination was unremarkable. BCG scar was seen on the left arm. Cutaneous examination revealed three well-defined plaques located on the right groin, right knee [Figure 1] and the left posterior thigh, varying in size from 5.1 × 3.7 cm to 7.1 × 6.2 cm. The plaques showed erythematous margins, with atrophic changes in the center. Skin biopsy showed tuberculoid granuloma with langhans giant cells in dermis [Figure 2], while tissue culture for tubercle bacilli, Periodic acid Schiff stain for fungus, and leishman stains were negative. Although Mantoux test was negative, polymerase chain reaction (PCR) from the tissue specimen for Mycobacterium tuberculosis was positive. Hematological and radiological investigations were normal while HIV testing was negative. The patient was treated with isoniazid, rifampicin, pyrazinamide and etambutol for 4 months, followed by isoniazid, rifampicin for 2 months, and the lesions showed complete resolution at the end of 6 months.
Figure 1.

Lupus vulgaris lesions on the right leg
Figure 2.
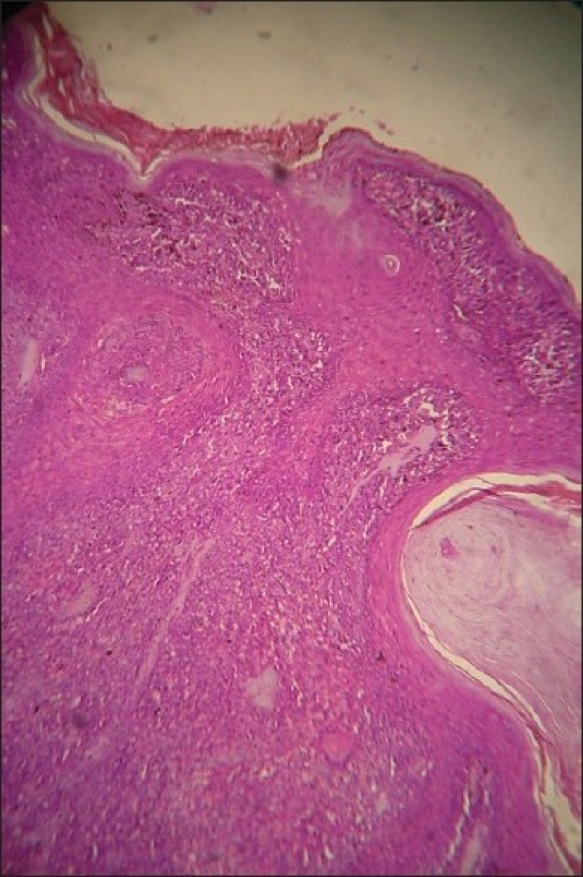
Histopathology showing granulomas with langhans giant cells
Lupus vulgaris is post-primary, paucibacillary cutaneous tuberculosis that occurs in individuals having moderate to high degree of immunity.[1] The source of infection can be either endogenous active tuberculosis foci such as glandular or pulmonary, which spreads through hematogenous/lymphatic route or an exogenous source that spreads by direct inoculation of tuberculosis bacilli into the skin.[1,2] Lupus vulgaris usually occurs singly on the face or neck, while in Indian children it is commonly reported on the legs and buttocks.[3] Common morphologic presentations include plaque, hypertrophic, atrophic, ulcerative and vegetative patterns, while clinical variants like multicentric lesions, symmetrical and sporotrichoid patterns have been recorded. Tuberculin test is usually positive, but it is difficult to demonstrate tuberculosis bacilli histopathologically or in culture. PCR, being specific and sensitive, has diagnostic significance in paucibacillary diseases like lupus vulgaris.[4]
The high incidence of lupus vulgaris on the legs in Indian children had been explained by the re-inoculation of tuberculosis bacilli through minor trauma or infection, especially during squatting.[5] Mantoux negative tuberculosis in a BCG vaccinated Indian is attributed to decreased cell mediated immunity (CMI), secondary to immunodeficiency or malnutrition and such patients are found to have increased chance of dissemination and variable response to treatment.[5,6] As our patient had no signs of immunodeficiency clinically or by laboratory tests, malnutrition could probably explain the Mantoux negativity and the occurrence of multicentric lesion. This case is reported for the unusual occurrence of multicentric lupus vulgaris in childhood and to highlight the necessity of early diagnosis and treatment of such Mantoux negative patients to prevent further dissemination and visceral involvement.
References
- 1.Gawkrodger DJ. Mycobacterial infections. In: Champion RH, Burton JL, Burns DA, Breathnach SM, editors. Rook/Wilkinson/Ebling Textbook of Dermatology. 6th ed. Oxford: Blackwell Science; 1998. pp. 1181–214. [Google Scholar]
- 2.Sehgal VN, Srivastava G, Bajaj P, Sengal R. Re-infection (secondary) inoculation cutaneous tuberculosis. Int J Dermatol. 2001;40:205–9. doi: 10.1046/j.1365-4362.2001.01138-6.x. [DOI] [PubMed] [Google Scholar]
- 3.Sethuraman G, Ramesh V, Ramam M, Sharma VK. Skin tuberculosis in children: Learning from India. Dermatol Clin. 2008;26:285–94. doi: 10.1016/j.det.2007.11.006. [DOI] [PubMed] [Google Scholar]
- 4.Chakravarti A, Dawan R, Shashidhar TB, Sahni J K. Lupus Vulgaris of external nose. Indian J Tuberc. 2006;53:220–2. [Google Scholar]
- 5.Padmavathy L, Rao LL. Ulcerative lupus vulgaris. Indian J Dermatol Venereol Leprol. 2005;71:134–5. doi: 10.4103/0378-6323.14007. [DOI] [PubMed] [Google Scholar]
- 6.Agnihotri MS, Pande SK, Verma H. Immunological significance of negative mantoux test in tuberculous patients. Indian J Tuberc. 1977;24:62–4. [Google Scholar]