

Abstract
Motor vehicle traffic is an important source of particulate pollution in cities of the developing world, where rapid growth, coupled with a lack of effective transport and land use planning, may result in harmful levels of fine particles (PM2.5) in the air. However, a lack of air monitoring data hinders health impact assessments and the development of transportation and land use policies that could reduce health burdens due to outdoor air pollution. To address this important need, a study of traffic-related PM2.5 was carried out in the city of Nairobi, Kenya, a model city for sub-Saharan Africa, in July 2009. Sampling was carried out using portable filter-based air samplers carried in backpacks by technicians on weekdays over two weeks at several sites in and around Nairobi ranging from high-traffic roadways to rural background. Mean daytime concentrations of PM2.5 ranged from 10.7 at the rural background site to 98.1 μg/m3 on a sidewalk in the central business district. Horizontal dispersion measurements demonstrated a decrease in PM2.5 concentration from 128.7 to 18.7 μg/m3 over 100 meters downwind of a major intersection in Nairobi. A vertical dispersion experiment revealed a decrease from 119.5 μg/m3 at street level to 42.8 μg/m3 on a third-floor rooftop in the central business district. Though not directly comparable to air quality guidelines, which are based on 24-hour or annual averages, the urban concentrations we observed raise concern with regard to public health and related policy. Taken together with survey data on commuting patterns within Nairobi, these results suggest that many Nairobi residents are exposed on a regular basis to elevated concentrations of fine particle air pollution, with potentially serious long-term implications for health.
Keywords: outdoor air quality, health, urban, transport, sub-Saharan Africa, Nairobi
1. Introduction
Motor vehicle traffic is an important source of harmful emissions of particulate pollution in cities of the developing world, where economic growth, coupled with a lack of effective transport and land use planning is resulting in increasing vehicle ownership and traffic congestion. These factors combine to create air pollution hotspots near roads. Urban growth is expected to continue at a rapid pace in the developing world, particularly in sub-Saharan Africa (UN, 2010) as rural populations continue to migrate to cities in search of employment and expectations of better living conditions. If nothing is done to reduce emissions and to better plan for urbanization, this trend can be expected to further exacerbate already serious air quality problems in sub-Saharan African cities as well as the health impacts that accompany them. Fine particulate matter (PM2.5), generated by fuel combustion (e.g., in motor vehicles) has been linked to a wide range of health effects, including more than 800,000 deaths in cities around the world (Cohen et al., 2004; Pope and Dockery, 2006). However, little information exists on levels of particulate air pollutants currently experienced by urban residents in Africa (Gatari et al., 2005; Maina et al., 2006; van Vliet and Kinney, 2007). This data gap hinders health impact assessments, the development of cost-effective strategies to reduce the health burden due to outdoor air pollution and the ability to influence urban transportation and planning policies in relation to air quality and health.
Nairobi, Kenya is in many ways typical of the fast growing cities of sub-Saharan Africa. Central Nairobi had a resident population of 3.2 million in 2009 with a daytime population of 4.2 million (Kenya National Bureau of Statistics (KNBS) 2008, in Ministry of Transport 2010). The resident population is up from about 1.3 million in 1989 (East African Statistical Department, in Obudho, 1997) representing a 3.9% annual growth. Similarly, the overall proportion of urban dwellers in Kenya has increased from 8% in the 1980s to over 34% in 2003 and is expected to reach 50% by 2020 (KNBS, 2008 in Ministry of Transport, 2010). The larger Nairobi metropolitan area had a population of 6.1 million in 2007, which is projected to rise to over 12 million by 2030 (Ministry of Nairobi Metropolitan Development, 2008). Much of this growth is occurring in the peri-urban regions, which are absorbing spillovers from the central city where scarce rental housing is increasingly unaffordable to average citizens. This growth, combined with a lack of investment in public transport and urban road infrastructure has resulted in increasing road deterioration, numbers of motor vehicles and congestion (Ministry of Transport and Communications, 2004). Spatially, the growth is taking the shape of urban sprawl which, along with growing urban air pollution exacerbates a number of other health risks, such as diabetes (see for example, Frumkin et al., 2004). Commercial and industrial activities remain concentrated in a central area where traffic congestion has become the norm. In an attempt to alleviate congestion, large-scale road infrastructure projects are currently underway in and around Nairobi and others are being planned. Considerations for long-term improvements in air quality and health must be taken into account as these projects are planned and implemented. Thus, the results of this study come at a crucial time.
It has been estimated that 90% of urban air pollution in rapidly growing cities in developing countries is attributable to motor vehicle emissions (UNEP, 2011) so while there are many sources of air pollution in Nairobi, including open air burning of refuse and biomass (Gatari, 2006), industrial operations and domestic cooking fires, motor vehicles play a critical role in the problem. Increasing road congestion, along with a high prevalence of old, poorly-maintained vehicles and of low quality fuels, contribute to this problem. One projection estimates that in a “do nothing” (or business as usual) scenario, the number of vehicle trips between 2004 and 2025 in the Nairobi Metropolitan Area will increase by 148% and that the average speed of trips will decrease from 35km/hr to 11km/hr as congestion increases (Japanese International Cooperation Agency, 2006) which makes it reasonable to assume that if nothing is done, urban air quality will worsen. The mixture of vehicles in 2004 was 29% passenger cars, 35% light-duty trucks, 7% heavy-duty trucks, 7% minibuses (Matatus), and 22% others (KNBS, 2007). Between 2002 and 2006, the number of trucks increased by about 60% (KNBS, 2007), reflecting increased activities in the agricultural and industrial sectors. Most trucks and buses rely on high sulfur diesel fuel (≤5000 ppm S) which leads to high particulate emissions. A large proportion of newly-registered vehicles in Nairobi are imported as used vehicles from East Asia.
There are important health implications of roadway emissions, particularly for highly exposed individuals near roadways and/or for population subgroups that are particularly sensitive to health effects, such as children and the elderly (Pope et al., 2002; Jansen et al., 2005; Ibald-Mulli, 2004). Of great concern are the large concentrations of pedestrians who walk along busy Nairobi roads. Aligula et al., (2005) reported that 49% of daily trips in Nairobi were either on foot or bicycle. However, bicycle use was limited by safety concerns (especially over lack of bicycle lanes) (Khayesi et al., 2010). Another 42% of trips used minibuses or other forms of public transport, while 9% were made in private vehicles. Another significant concern involves populations such as street vendors and traffic police, who spend their days along and on congested roadsides and roads.
Motor vehicle emissions include a range of pollutants, including particulate matter (PM), carbon monoxide, sulfur oxides, nitrogen oxides and a wide range of volatile organic compounds, which react with sunlight to form ozone Many of these pollutants have well-known health effects which may be exhibited with short term exposure, including wheezing, coughing, shortness of breath phlegm and sore throats as well as irritation of existing respiratory conditions such as asthma (Hedley et al, 2003; Frumkin et al, 2004, Schwela et al, 2006). However, PM2.5 is of particular significance because research on health effects in urban areas has demonstrated associations between both short-term and long-term average ambient PM2.5 concentrations and a variety of adverse health outcomes. These include increased post neonatal infant mortality (Woodruff et al, 2006) and premature deaths related to heart and lung diseases (e.g., Dockery et al, 1993; Schwartz, 1994; Samet et al., 2000; Pope et al., 2002). PM2.5 is a complex mixture of solid or liquid organic and inorganic particles that share the property of being less than/equal to 2.5 μm in aerodynamic diameter. Because of their small sizes, PM2.5 particles are able to penetrate deeply into the lungs where they can exert adverse effects. In 2005, the World Health Organization (WHO), based on known health effects, set a 24-hour average guideline of 25 μg/m3 and an annual average guideline of 10 μg/m3. PM2.5 includes black carbon (BC), or soot, which is emitted by incomplete combustion sources including diesel and poorly-tuned gasoline engines, and open fires. In addition to adverse health impacts (USEPA, 2002; Bell et al., 2009), BC contributes to climate change (Ramanathan and Carmichael, 2008).
Understanding and quantifying the effects of roadway traffic on PM2.5 concentrations in Nairobi would help improve the knowledge base to influence and support urgently needed policy solutions aimed at improving health through decreased transport emissions. To address this important need, the Nairobi Area Traffic Contribution to Air Pollution (NATCAP) study was carried out in the summer of 2009. The overall objective of the study was to characterize the impacts of heavy motor vehicle traffic on concentrations of PM2.5 near roadways in Nairobi so that levels of exposure and their possible impacts on health could be considered.
2. Methods
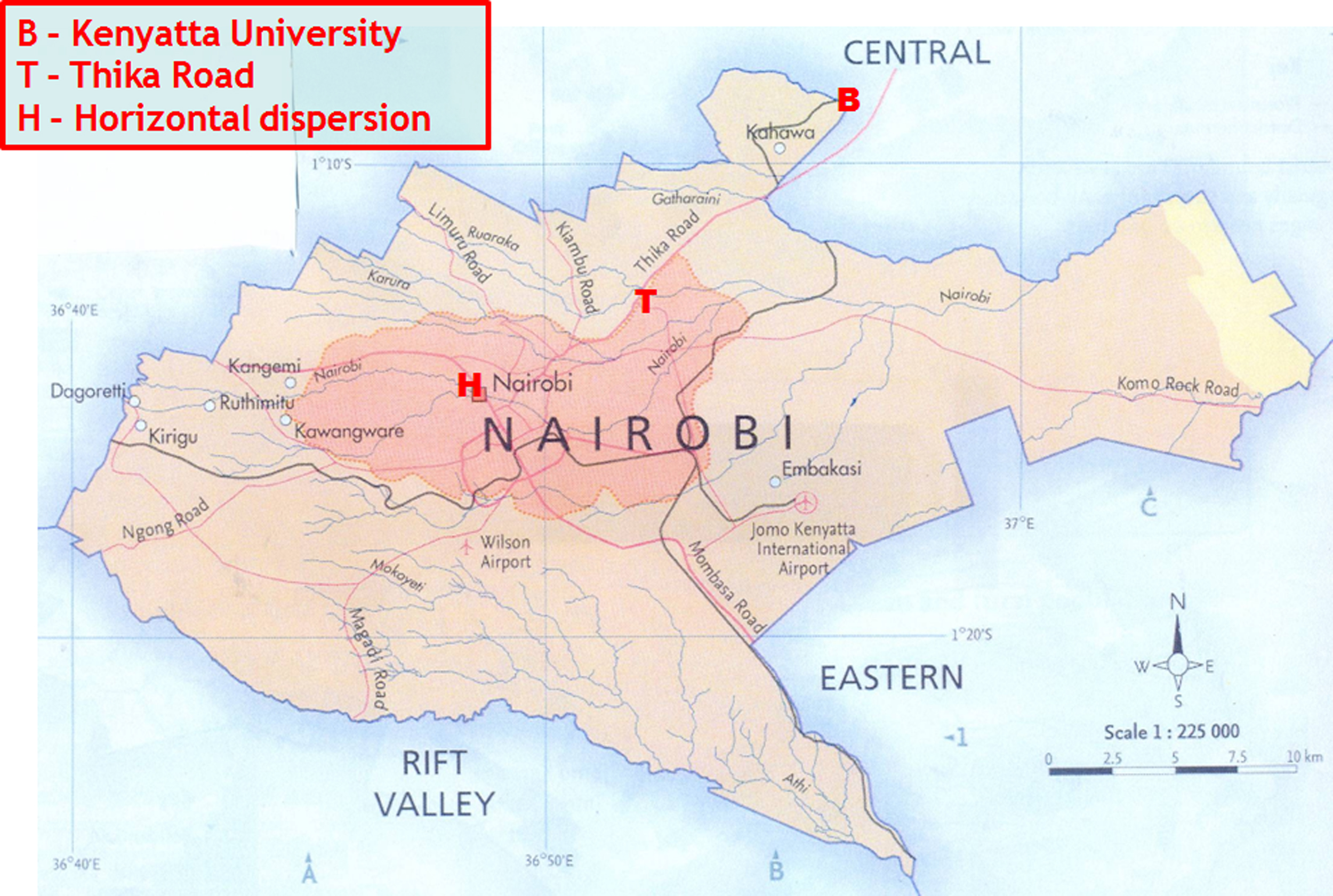
In this collaborative study, Columbia University, University of Nairobi and Jomo Kenyatta University of Agriculture and Technology together undertook an intensive air monitoring campaign for PM2.5 during two weeks in July 2009. Nairobi is located 1.32°S and 36.9°E and experiences two rainy seasons; one from March to May and another from October to December. Its proximity near the equator lends to overall mild winters, but due to its altitude (approximately 1.6 km above sea level), Nairobi experiences some seasonal variation in temperatures (Gatari and Boman, 2005). Sampling was carried out on weekdays (Monday through Friday) at a range of sites in and around Nairobi ranging from high-traffic roadways to rural background (see supplemental material Figures 1 and 2). Measurements were taken on the weekdays to capture typical concentrations at times of highest vehicle and pedestrian traffic on Nairobi streets.
Air monitoring was carried out simultaneously at five core sites from 0730 to 1830 hr for nine days, with the tenth day reserved for field blank measurements. These five sites included Ronald Ngala, Tom Mboya, and River Road, which represented heavy-traffic sites in the Central Business District of Nairobi (CBD); Thika Road, a highway linking outlying peri-urban areas and suburbs with Nairobi; and Kenyatta University, a rural background site. As part of a separate ongoing study (led by Gothenburg University, Sweden), monitoring was also carried out on the rooftop at the University of Nairobi’s main campus in the CBD. Since this site was not directly impacted by traffic, it may be viewed as an urban background site for the purposes of the present study. While included here for reference, these latter data are not directly comparable because the samples were collected over 24-hour intervals.
Nairobi’s downtown CBD is characterized by retail shops, supermarkets, and various other businesses, and has high vehicle and pedestrian traffic. In addition, the CBD serves as an important transfer point for minibuses linking urban, peri-urban and rural destinations. Monitoring was carried out at three sites within the CBD. The River Road site had high buildings on either side of the street forming a street canyon. There were several hotels in the vicinity. The Ronald Ngala site was near a major minibus stop and near a congested pickup point for passengers. The Tom Mboya site was near the Kenya National Archive building and experienced heavy pedestrian and vehicle traffic most of the day.
Thika Road serves as an important commuter route into and out of Nairobi, serving both the expanding Nairobi metropolis and the heavily populated central and eastern regions of Kenya. Traffic jams on this road begin as early as 0530 hr for those traveling into Nairobi, and again in the evening to as late as 2030 hr. Sampling was conducted on both sides of this highway.
The rural background site at Kenyatta University was located approximately 20 km northeast of downtown. The sampler was placed on a chair in an open field on a remote area of the university grounds.
In addition to the five sites sampled every day, air samples were also taken at two spatial dispersion sites for 3-4 days during the study. A horizontal dispersion site was located at the high-traffic Chiromo-Museum intersection near the University of Nairobi, where samples were taken on four days. The objective was to examine the decrease in PM2.5 concentrations with increasing distances downwind of a major intersection. At this site, the prevailing winds were south easterlies, and samples were taken simultaneously at the curbside upwind of the road (southeast of the intersection), immediately downwind (northwest of the intersection), and at 30 m and 100 m downwind in a straight line.
A vertical dispersion site situated in the Nairobi CBD was sampled for three days. It was located near the Nairobi Fire Station at a busy intersection that marks the junction of Tom Mboya Street and River Road. Tall buildings line both sides of the street, creating a street canyon, with the main source of air flowing through this canyon from the intersection. At this site, measurements were taken at the street level (~1.2 m agl), 2nd floor of the building (~4 m agl), 3rd floor (~10 m agl), and the third floor rooftop (four levels above ground, or ~17 m agl).
Air monitoring was carried out by 60 field technicians (mainly students and recent graduates from the University of Nairobi) hired specifically for the project. Supervision and quality control was carried out by a separate group of students and staff at the Institute of Nuclear Science and Technology (INST) at the University of Nairobi and from Columbia University. Technicians worked daily in one of two six-hour shifts. The first shift ran from 0700 to 1300 hr and the second shift from 1300 to 1900 hr. As mentioned above, sampling was carried out from 0730 to 1830 hr each day at each site; the extra half hour in each of the shifts was used for preparation and travel to the sites. Every group and shift had a floating student who facilitated rest times after every hour. Prior to the start of the monitoring campaign, the supervisors held a series of four meetings to strategize and train everybody who was involved in the exercise. Full staff meetings were also held on Saturdays during the study to review the previous sampling week’s challenges and successes.
Airborne particle concentrations were monitored using portable air sampling instruments housed in backpacks carried by field technicians. The instrument pumped air at 4 liters per minute (LPM) through an anodized aluminum cyclone (BGI Inc., Waltham, MA) to remove particles larger than 2.5 μm in aerodynamic diameter before depositing smaller particles on a Teflon filter fitted into a plastic cassette downstream of the cyclone. Air was drawn by a BGI personal vacuum pump powered by a rechargeable battery-pack. Flow rates were measured and recorded before and after each sampling event by trained staff from Columbia University and INST using rotameters (SKC) that were pre-calibrated by a mass flow meter (TSI Model 4199). The times of the sampling period were recorded using a digital minute timer on the pump. After sampling, filter cassettes were separated from the tubing and pumps, then capped and placed in air-tight plastic bags.
The sample filters were transported to Columbia University where they were analyzed for mass (PM2.5). Filters were then preserved for later analyses (e.g., black carbon, trace metals, PAHs). All filters were pre-weighed at Columbia University before shipment to Nairobi under controlled temperature and humidity conditions in a HEPA-filtered hood. The filters were re-weighed under the same conditions after sampling to determine PM2.5 mass.
Pumps were carried in backpacks, with the inlet nozzle placed near the shoulder to approximate the pedestrian breathing zone. For the sites in the CBD, a student carrying a backpack stood on the curbside of the road for one hour then crossed the road and sampled for another hour. This sampling process was repeated throughout the sampling period to capture an average sample of both sides of the road. At Thika Road, air samples were taken simultaneously on both curbsides of the road using two separate air monitors since it was dangerous to cross the road on foot. Dispersion site monitoring was carried out using one sampler for each sub-location (i.e., various horizontal or vertical distances), with two to three students per sampling location. The experiments were closely supervised by senior investigators to ensure proper procedures were followed. Site-to-site and day-to-day differences in particle concentrations were analyzed using one-way analysis of variance.
3. Results
Mean concentrations of PM2.5 at the five core sampling sites varied markedly, ranging from 10.7 to 98.1 μg/m3 (Table 1 and Figure 1), with highest levels observed at the three sites in the CBD, slightly lower concentrations on Thika Road (the commuter route), and very low concentrations at the rural background site at Kenyatta University. Site to site variations were statistically significant across all five sites, across the four traffic sites, and across the three CBD sites in 2-way ANOVA analyses. PM2.5 at the University of Nairobi rooftop site was intermediate to those from Thika Road and Kenyatta University. Though within the CBD, the University of Nairobi site was located on a 5th floor rooftop and away from major traffic sources. It also monitored 24-hr average concentrations which thus included nighttime concentrations which were expected to be lower than daytime concentrations monitored at the five core sites.
Table 1.
11-hr averages (0730-1830 hr) PM2.5 concentrations (μg/m3) at seven sites in Nairobi.
| Location | July 6 | July 7 | July 8 | July 9 | July 10 | July 13 | July 14 | July 15 | July 16 | Mean ± SD |
|---|---|---|---|---|---|---|---|---|---|---|
| Core Sites (RN, TM, and RR are in the central business district; TR is a commuter route; KU is in a rural location) | ||||||||||
|
| ||||||||||
| Ronald Ngala | 73.9 | 64.3 | 74.0 | 94.5 | 93.6 | 59.1 | 61.1 | 92.6 | 67.6 | 75.6±14.4 |
| Tom Mboya | 95.0 | 127.5 | 124.1 | 94.7 | 103.7 | 87.9 | 100.9 | 77.0 | 71.7 | 98.1±18.9 |
| River Road | 83.1 | 138.8 | 115.3 | 84.6 | 66.5 | 67.3 | 77.7 | 95.4 | 70.1 | 88.8±24.3 |
| Thika Rd In | 70.3 | 93.3 | 50.4 | 26.2 | 60.8 | 62.1 | 58.4 | 57.5 | 42.5 | 58.1+18.8 |
| Thika Rd Out | 79.6 | 101.1 | 81.0 | 65.8 | 77.2 | 76.9 | 73.8 | 62.8 | 90.1 | 78.7±11.7 |
| Kenyatta Univ | 7.4 | 13.3 | 12.1 | 6.9 | 5.0 | 16.0 | 13.6 | 11.5 | 10.7±3.8 | |
|
| ||||||||||
| Horizontal Dispersion Site | ||||||||||
|
| ||||||||||
| Upwind 0m | 45.7 | 38.7 | 59.2 | 59.2 | 50.7±10.2 | |||||
| Downwind 0m | 149.3 | 129.4 | 100.3 | 135.8 | 128.7± 20.7 | |||||
| Downwind 30m | 27.1 | 29.4 | 25.0 | 32.2 | 28.4+3.1 | |||||
| Downwind 100m | 19.9 | 21.1 | 14.6 | 19.2 | 18.7+2.8 | |||||
|
| ||||||||||
| Vertical Dispersion Site | ||||||||||
|
| ||||||||||
| Street level | 98.2 | 133.0 | 127.3 | 119.5+18.7 | ||||||
| 1st floor | 67.1 | 80.2 | 81.7 | 76.3+8.0 | ||||||
| 3rd floor | 46.6 | 66.3 | 57.7 | 56.9+9.9 | ||||||
| Rooftop | 33.9 | 46.4 | 48.1 | 42.8+7.8 | ||||||
|
| ||||||||||
| Urban Rooftop Reference Site (24 hour average) | ||||||||||
|
| ||||||||||
| 40.3 | 49.6 | 28.2 | 53.1 | 14.5 | 33.4 | 30.0 | 26.9 | 37.8 | 34.9±11.9 | |
Note that the University of Nairobi site was operated as part of a separate ongoing study, and is included here for reference purposes courtesy of Johan Boman, Gothenburg University, Sweden. Concentrations at the University of Nairobi site are 24-hr averages.
Fig. 1.
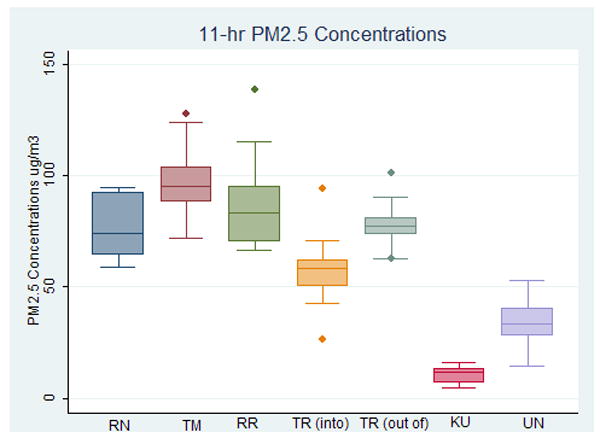
Average 0730-1830 hr weekday PM2.5 concentrations at five core sites in Nairobi. The University of Nairobi site is included for reference but is not directly comparable due to different sampling parameters (RN= Ronald Ngala, RR= River Road, TM=Tom Mboya, TR=Thika Rd, KU= Kenyatta Univ., UN= Univ. of Nairobi).
Results from the horizontal dispersion site (Table 1 and Figure 2) show a rapid reduction in PM2.5 concentrations with increasing distance from the intersection. Concentrations immediately adjacent to the intersection averaged 50.7 μg/m3 in the usual upwind direction and 128.7 μg/m3 in the usual downwind direction implying the high influence of vehicle emissions downwind. After 30 and 100 m, concentrations in the usual downwind direction were reduced to 28.4 and 18.7 μg/m3 respectively. This represented over a six-fold difference in concentrations within 100 m of the traffic source. The intersection was outside of the CBD and adjacent to university sports fields, which meant that the traffic in, out and around the intersection was the primary source of particulate matter in this location. This is reflected in the relatively low concentrations seen 100 m downwind, which were lower than the upwind location and substantially below those seen on the University of Nairobi rooftop (also shown in Table 1). These findings indicate that the concept of “urban background” is site specific and must take account of local and regional sources as well as geography in order to be interpretable.
Fig. 2.
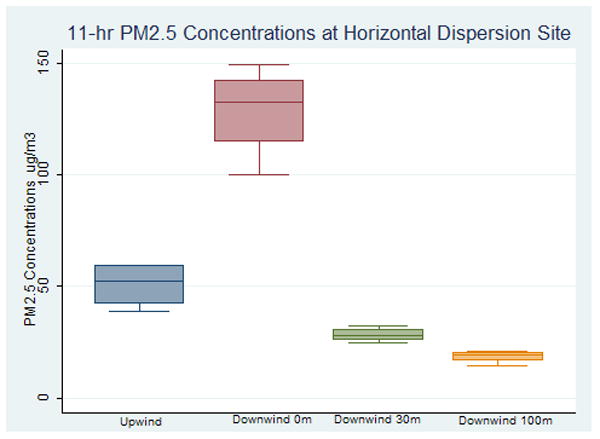
Average 0730-1830 hr weekday PM2.5 concentrations at Chiromo-Museum Road Roundabout (horizontal dispersion site).
Similar to the horizontal dispersion site, the vertical dispersion experiment (Table 1 and Figure 3) revealed a decrease in PM2.5 concentrations with vertical distance away from the roadway ground level in the street canyon site located in the CBD. Mean PM2.5 concentrations at different heights over three days of monitoring ranged from 119.5 μg/m3 at curbside, 76.3 μg/m3 on the first floor balcony, 56.9 μg/m3 on the third floor balcony, to 42.8 μg/m3 on the rooftop. The lowest concentration, on the rooftop, was similar to but greater than those monitored on the University of Nairobi rooftop site, perhaps reflecting the impact of greater traffic volumes near the vertical dispersion site.
Fig. 3.
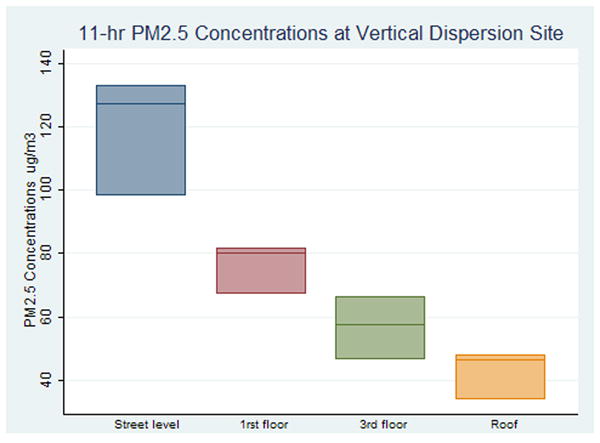
Average 0730-1830 hr weekday PM2.5 concentrations near the Nairobi Fire Station (vertical dispersion site).
4. Discussion and Policy Implications
Daytime concentrations of PM2.5 were seen to be very high at sites located adjacent to roadways in this study, ranging from 50.7 to 128.7 μg/m3 across the three CBD sites, the commuter route, and the near-roadway locations at the horizontal and vertical dispersion sites. These data represent averages of daytime levels over 3-9 days, and thus cannot be directly compared with health-based guideline concentrations. As noted above, the WHO’s 24-hour average guideline is 25 μg/m3 and the annual average guideline is 10 μg/m3 (WHO, 2006). Since our data were collected for just two weeks in July, it is of interest to know how this period compares to other seasons in Nairobi. Systematic, year-round monitoring data do not yet exist for Nairobi. However, preliminary inferences can be derived from monthly average total suspended particulate (TSP) matter and elemental concentrations (e.g., Bromine) reported for Nairobi between December 1993 and October 1004 by Gatebe and colleagues (Gatebe et al., 1996). Considerable month to month variability was seen for TSP, and July was among the lowest months reported. Bromine concentrations showed less seasonality, and July appeared to fall at or slightly below the annual mean. Bromine has been shown to be a tracer for fine particles in the east African city of Dar es Salaam, Tanzania (Bennett et al., 2005). Our data generally indicated that roadside concentrations were higher than concentrations monitored simultaneously at urban sites away from roadways. This was confirmed by the horizontal and vertical dispersion sites, which showed sharp concentration declines with distance away from roadway sources. Based on these observations, we tentatively conclude that traffic emissions were likely the dominant source of PM2.5 during our study. However, a firm conclusion in this regard would require more extensive data, including trace elements (work in progress). While it is agreed that traffic emissions world-wide contribute significantly to PM air pollution, it would be useful in more extensive future studies to determine the contribution of other sources, such as industry and biomass burning.
We can compare our horizontal dispersion results to those from a PM2.5 roadside dispersion study in Hong Kong, which employed a protocol similar to ours. In the Hong Kong study, PM2.5 concentrations decreased very slowly with distance from the road, going from 57 μg/m3 by the roadside, to 54 μg/m3 at the 30 m distance, to 48 μg/m3 at the 100 m distance (Wang et al., 2006). In comparison, at our Nairobi dispersion site, average concentrations by the roadside (0 m) were more than four times higher than average concentrations 30 m away, and over six times higher than those 100 m away. The difference between these two dispersion profiles may be attributed to differences in the geography and dominant source of ambient PM2.5 between the two cities. The Hong Kong study was set in a dense urban location, where buildings prevented PM2.5 from dispersing quickly. Our Nairobi site was located on the edge of open sports fields, allowing the uninhibited flow of wind and the rapid dispersion of pollutants away from the heavy traffic roadway. Furthermore, studies have shown that the primary source of PM2.5 in Hong Kong is not local vehicle emissions but regional industrial emissions from the Pearl River Delta (Hagler et al., 2007). In contrast, the Nairobi dispersion profile showed a sharp drop in concentrations that was determined almost entirely by roadway emissions. This result implies that concentrations could be substantially reduced by regulations directed at vehicular emissions in Nairobi. This idea is supported by a recently published 2003 study, which found that levels of PM10 were well above WHO guidelines on a roundabout connecting two Nairobi highways (University and Uhuru) and that the strong correlation between fine particulates and vehicle density indicated that vehicular emissions were the main source of fine particulate matter (Odhiambo et al, 2010). An earlier study in Nairobi reported highly elevated PM2.5 and BC concentrations measured while driving in the CBD and on Thika Road (van Vliet and Kinney, 2007).
We can also compare our particulate matter concentrations with data from those observed in other cities. In Accra, Ghana, annual average roadside PM2.5 levels ranged from 39 to 53 ug/m3 (Dionisio et al, 2010). Near-road measurements in that study were taken at the rooftop level and are fairly similar to the rooftop measurements at our vertical dispersion site. It may be plausible to assume that if measurements in the Accra study were taken on sidewalks, as in our study, that higher concentrations may have been observed.
In North America, a sidewalk air quality monitoring study conducted in an underprivileged urban neighborhood in New York City (Harlem) where diesel vehicle traffic density was disproportionately high found that PM2.5 levels over five summer days averaged 42 μg/m3 (Kinney et al, 2000). Similar to our Nairobi study, samples were taken at about shoulder-level, using portable monitors worn by project staff, An investigation into asthma hospitalizations in New York City showed that several sections of this New York City neighborhood had the highest rates (Carr et al, 1992 in Kinney et al, 2000). Findings from a more recent New York City-wide study show that average roadside PM2.5 concentrations are 12.4 μg/m3 in the summer and 15.7 μg/m3 in the winter (as a result of building-related emissions for heating). It is interesting to note that levels of PM2.5. were 15% and 27% greater at higher traffic, as opposed to lower traffic sites, in the summer and winter months, respectively (Clougherty, 2010a; Clougherty, 2010b) indicating the contribution of vehicle emissions to pollutant levels. Samples for this study were collected close to street level; samplers were mounted on lamp posts at 10-12 feet. In Europe, annual average PM2.5 concentrations at traffic sites in Stockholm, Munich, the Netherlands, and the Rotterdam area ranged from 11.6 μg/m3 in Stockholm to 20.1 μg/m3 in Rotterdam. PM2.5 concentrations at the study’s traffic sites were on average 17-18% higher than at urban background sites (Hoek et al, 2002). The authors indicate that heights at which the various samples were taken in this multi-area study were at least 1.5 meters above the surface but not in the dripline of trees, which allows us to assume that the samples were taken close to street level.
Our findings in Nairobi suggest that people who spend substantial time on or near roadways— particularly motorists, pedestrians, traffic police and those engaged in the many informal businesses located along roadways— are of particular concern regarding potential human health impacts. Those who live and work downtown in buildings adjacent to busy roads may also be exposed to high PM2.5 concentrations. Results from the vertical dispersion site showed that PM2.5 concentrations did decrease significantly with height. However, concentrations on the 3rd floor rooftop were still double the WHO 24-hour guideline. This suggests that residents of buildings adjacent to heavy traffic roadways in Nairobi, even if they live on upper level floors, may still be exposed to dangerously high particulate matter levels.
Pope and Dockery (2006) summarize the results of over 20 peer-reviewed prospective cohort studies that found that long-term exposure to elevated levels of PM leads to increased mortality from heart and lung disease. For example, in an extended analysis of a survey of six American cities, Laden et al (2006) found that with each 10-μg/m3 increase in PM2.5, the relative risk of mortality from cardiopulmonary diseases was increased by 28%. In terms of postneonatal infant mortality, the impacts are quite alarming - Woodruff et al (2006) found that each 10-μg/m3 increase in PM2.5 was associated with a near doubling of these deaths due to respiratory causes. Evidence has also shown an association between air pollution and lung cancer (Pope and Dockery, 2006) and air pollution more generally (that is, when elevated levels of other pollutants are considered) has also linked to lung cancer, particularly as a result of traffic emissions (Nyberg, 2000). Health impacts such as asthma, bronchial infections, chronic cough and decreased lung function are also linked to air pollution, as well as increased emergency room visits and hospitalizations and school absences (e.g., Pope and Dockery, 2002; Schwela et al, 2006). Results of a three-year study in Mexico City found that long-term exposure to ambient air pollutants is associated with lung-growth deficits in children; while no specific sources are identified, the authors indicate that the effect is likely due to vehicular exhaust (Rojas-Martinez et al, 2007). In addition to impacts in children, these early lung deficits may increase the risk of developing lung and heart disease (with associated increases in morbidity and mortality) later in life (Schroeder et al, 2003; Schunemann et al, 2000).
There have been questions raised about whether it is possible to extrapolate the concentration-response functions derived from studies in high-income countries to those of middle- and low-income (e.g., Smith and Akbar, 2003). Studies in Asia have been developed to respond to these concerns and while results from a coordinated time-series analysis in Bangkok, Hong Kong, Shanghai and Wuhan suggest that the effect of PM on daily mortality remain consistent with the Western industrial nations (Wong et al, 2008), there have been no cohort studies of the effects of long-term exposure to air pollution on mortality from cardiovascular and respiratory diseases in Asian populations (HEI, 2010). There is a general lack of data from sub-Saharan Africa. Furthermore, factors related to socioeconomic status may modify the effects of air pollution, leading to larger effects in some populations (HEI, 2010). Slum populations in South Asia have been found to be simultaneously at risk from both household environmental hazards, from poor food and indoor air and water quality, as well as to community hazards in the form of outdoor air pollution, traffic, etc (Smith, K.R., 1997). This pattern likely holds true for Nairobi, where health outcomes are not only significantly worse in slum populations than in other areas of Nairobi but in some cases worse than those in rural areas (Volavka-Close and Sclar, 2010; APHRC, 2002). In addition to the relationship between competing risk factors, poverty and outdoor air pollution, the varying chemical composition of particle mixtures in low and middle-income countries (e.g., they may have higher fractions of diesel exhaust and biomass fuel particles) as well as higher levels of pollutants are concerns for extrapolation (Smith and Akbar, 2003). These factors should be incorporated into critically needed efforts to assess health impacts of outdoor air pollution on the entire population, as well as related policy-making in Nairobi and other rapidly growing urban areas in developing countries. Further air monitoring, as well as epidemiologic studies in Nairobi, are needed for a comprehensive assessment of health impacts as well as any evaluation of associated costs.
If we define the population exposed to roadside pollution as all those driving, walking or working on the street, working in buildings or living in apartments above high-traffic roads, then a large fraction of Nairobi residents are expected to be exposed to harmful roadway emissions on a regular basis. Another cause for the high roadway exposure across the entire population is the high concentration of informal businesses and shops on roadsides, which are frequented by lower and middle class urbanites alike. As noted, walking is the single most common mode of transport in Nairobi (Aligula et al., 2005). People who walk do so primarily because they cannot afford other means of transport (Salon and Gulyani, 2010). This is significant because these pedestrians are the city’s poorest residents, which suggests that this already-vulnerable population group may suffer from disproportionate exposure to or effects from air pollution, particularly if their travel times are longer. Additionally, these residents typically have lower levels of access to health care and other services, so it may be more likely that health impacts of emissions will go untreated. The importance of walking as a means of transportation was confirmed by pedestrian count results in the current study for the Ronald Ngala and Tom Mboya sites, which were each frequented by an average of 90,000 people every day between 0700 and 1900 hr.
In addition to being one of the few studies to examine roadway emissions in a sub-Saharan African city, this project also showed the potential for partnerships within the local community for research and capacity building. Students and staff from University of Nairobi and Columbia University worked closely together in designing and implementing this study, as well as engaging Nairobi residents. The success of the project encourages more partnerships such as these to occur throughout research in rapidly-urbanizing sub-Saharan Africa. The importance of partnerships between the global North and South and the co-production of knowledge that they foster has been documented (e.g., Klopp et al, forthcoming).
The policy implications of this study are substantial. On a metropolitan level, Nairobi is growing quickly without accompanying transportation and infrastructure services or even an urban transportation policy, as indicated in the Kenya Ministry of Transport’s Recommendations on an Integrated National Transport Policy (INTP) (Kenya Ministry of Transport and Communications, 2004). This lack of policy is made manifest by a transportation system characterised by severe congestion, high-polluting vehicles, lack of pedestrian and bicycle lanes, lack of accessible, high quality public transport options, and deteriorating infrastructure (Ministry of Transport and Communications, 2004; Aligula et al, 2005). The Integrated National Transport Policy (INTP) recommendations evolved into a 2010 policy paper, “Sessional Paper on INTP” which was passed by the Cabinet and has been submitted to the Parliament for approval. This paper identifies the transport sector’s top challenges as poor quality of transport services, inappropriate modal split, weak adherence to environmental requirements and lack of an urban transport policy. There is brief mention that traffic congestion contributes to air pollution but at the same time it is noted that “no measures exist to determine the damage caused to the environment” due to this pollution. Links between air pollution and human health implications, as well as costs associated with health impacts must be made clear and become an integral part of transport policy formulation and implementation. It is hoped that the current paper will assist in highlighting health considerations in those policy discussions. This is particularly critical at a time when the government is moving forward with massive road expansion projects which seem to be primarily opening up space for more cars on bigger roads. While upgrading and expansion might be necessary, this alone will not solve the problems of congestion and air pollution; Los Angeles, a city that tried to build its transport system almost exclusively around freeways is a prime example of how this approach fails (Kenworthy, 1997). Thika Road, one of this study’s sampling sites, is currently undergoing upgrading and expansion, transforming the road into an eight-lane superhighway. Further research should include ongoing monitoring along this road. While congestion may initially ease, if no measures are taken to reduce demand and limit the use of automobiles through an efficient public transport system and safe, non-motorized transport alternatives, Thika and other newly-expanded roads will likely fill with cars again. This would suggest further worsening of air quality and the negative health impacts associated with it.
Supplementary Material
Map indicating monitoring locations for Nairobi urban sites and Nairobi’s location in Africa.
{kind=link}
Map showing Thika Road and Kenyatta University Location (Rural Background site).
{kind=link}
Acknowledgments
This study was initiated by the Center for Sustainable Urban Development (CSUD) and funded by the Volvo Research and Educational Foundations (VREF). CSUD is a VREF Center of Excellence for Future Urban Transport and is housed at Columbia University’s Earth Institute. The authors also acknowledge research support by the International Science Programs to the Institute of Nuclear Science and Technology, the host of this corroborative study. Additional support was provided by the NIEHS Center for Environmental Health in Northern Manhattan (ES09089). The authors also would like to thank Jonathan Chanin of CSUD for his efforts in preparing the document and Jennifer Schumacher-Kocik and Jennifer Graeff for their extensive administrative and logistical efforts related to the study.
Role of the Funding Source Funding for this research and preparation of the article was provided by the Volvo Research and Educational Foundations (VREF), the International Science Programs and the NIEHS Center for Environmental Health in Northern Manhattan (ES09089). These sponsors played no role in study design; in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the paper for publication.
Biographies
Dr. Patrick Kinney is Professor of Environmental Health Sciences at the Mailman School of Public Health at Columbia University. His research and teaching address health impacts of air pollution and climate change in a global context.
Dr. Michael Gatari Gichuru holds a PhD in Environmental Science (Physics) and his key area of research is atmospheric aerosol in the perspective of human health and climate change. He is a university lecturer in applications of nuclear techniques, and radiation detection, measurements and electronics.
Nicole Ngo is a Ph.D. candidate in Sustainable Development at Columbia University. She is interested in air pollution and its health impacts, as well as its influence on climate change.
Nicole Volavka-Close is Associate Director of the Center for Sustainable Urban Development, housed at The Earth Institute, Columbia University. Her research interests include the address of health impacts of transport and land use in the global context.
Dr. Peter K. Ndiba is a Senior Lecturer in the Department of Civil Engineering, University of Nairobi, Kenya. He teaches environmental engineering and his main research interest is heavy metals in sediments, soils, water and air.
Anna Law obtained her Bachelor’s Degree in Environmental Policy from Barnard College, Columbia University in May 2010. For her senior thesis, she sought to quantify the impacts of fine particulate matter air pollution on mortality in Nairobi and to propose policy solutions to curb fine particulate matter roadway emissions.
Dr. Anthony Gachanja is Professor of Analytical Environmental Chemistry in the Faculty of Science, Jomo Kenyatta University of Agriculture and Technology, Nairobi, Kenya. His research is in Analytical Environmental pollution studies in Kenya.
Samuel Gaita holds a MSc in Atmospheric Science (Chemistry) from Gothenburg University, Sweden. He is currently a graduate student at the Institute of Nuclear Science and Technology, University of Nairobi. His research interest is the application of radiation spectroscopy methods in atmospheric research with regard to human health and climate change.
Dr Steven N. Chillrud is a Doherty Research Professor at Lamont-Doherty Earth Observatory of Columbia University. His air pollution research focuses on identifying and characterizing exposure pathways and sources of airborne particulate matter including development and testing of new air monitoring equipment.
Dr. Elliott Sclar is Professor of Urban Planning and Director of the Center for Sustainable Urban Development housed at The Earth Institute, Columbia University. He specializes in international urban and transportation planning and economics.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Aligula EM, Abiero-Gariy Z, Mutua J, Owegi F, Osengo C, Olela R. Special Report No 7. Nairobi, Kenya: Kenya Institute for Public Policy and Research Analysis; 2005. Urban Public Transport Patterns in Kenya: A Case Study of Nairobi City. [Google Scholar]
- African Population and Health Research Center (APHRC) Populatio and Health Dynamics in Nairobi’s Informal Settlements. Nairobi: African Population and Health Research Center; 2002. [Google Scholar]
- Bennet C, Jonsson P, Lingren ES. Concentrations and sources of trace elements in particulate air pollution, Dar es Salaam, Tanzania, studied by EDXRF. X-Ray Spectrometry. 2005;34:1–6. [Google Scholar]
- Carr W, Zeitel L, Weiss K. Variations in Asthma Hospitalization and Deaths in New York City. Journal of the American Medical Association. 1992;82:59–65. doi: 10.2105/ajph.82.1.59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clougherty JE, Kheirbek I, Johnson S, Pezeshki G, Bryan Jacobson J, Eisl HM, Gorczynski JE, Ross Z, Kitson H, Benson A, Camacho A, Werbe-Fuentes J, Haviland-Markowitz J, Munoz R, Tilles A, Strickland CH, Charles-Guttman K, Markowitz S, Kass D, Matte T. The New York City Community Air Survey: Results from Summer Monitoring 2009. New York City: Department of Health and Mental Hygiene, and NYC Mayor’s Office for Long-Term Planning and Sustainability. 8 April 2010; 2009a. http://www.nyc.gov/html/doh/downloads/pdf/eode/nyccas-report-summer09.pdf. [Google Scholar]
- Clougherty JE, Kheirbek I, Johnson S, Pezeshki G, Bryan Jacobson J, Eisl HM, Gorczynski JE, Ross Z, Kitson H, Benson A, Camacho A, Werbe-Fuentes J, Haviland-Markowitz J, Munoz R, Tilles A, Strickland CH, Charles-Guttman K, Markowitz S, Kass D, Matte T. The New York City Community Air Survey: Results from Winter Monitoring 2008-2009. New York City: Department of Health and Mental Hygiene, and NYC Mayor’s Office for Long-Term Planning and Sustainability. 8 April 2010; 2009b. http://www.nyc.gov/html/doh/downloads/pdf/eode/nyccas_master_report_12_15_09.pdf. [Google Scholar]
- Cohen A, Anderson H, Ostra B, Pandey D, Krzyzanowski M, Künzli N, Gutschmidt K, Pope CA, III, Romieu I, Samet J, Smith K. Chapter 17: Urban air pollution. In: Ezzati Majid, Lopez Alan D, Rodgers Anthony, Murray ChristopherJL., editors. Comparative Quantification of Health Risks: Global and Regional Burden of Disease Attributable to Selected Major Risk Factors, Volume 1. Geneva, Switzerland: World Health Organization; 2004. pp. 1353–1434. [Google Scholar]
- Dioniso KL, Arku RE, Friedman AB, Hughes AF, Vallarino J, Carmichael H, Spengler JD, Agyei-Mensah S, Ezzati M. Air Pollution in Accra Neighborhoods: Spatial, Socioeconomic and Temporal Patterns. Environmental Science and Technology. 2010;44(7):2270–2276. doi: 10.1021/es903276s. [DOI] [PubMed] [Google Scholar]
- Dockery DW, Pope CA, III, Xu X, Spengler JD, Ware JH, Fay ME, Ferris BG, Speizer FA. An Association between Air Pollution and Mortality in Six U.S. Cities. New England Journal of Medicine. 1993;329(24):1753–59. doi: 10.1056/NEJM199312093292401. [DOI] [PubMed] [Google Scholar]
- Frumkin H, Frank L, Jackson R. Urban Sprawl and Public Health: Designing, Planning and Building for Healthy Communities. Island Press; Washington, D.C: 2004. [Google Scholar]
- Gatari MJ, Boman J. Black carbon and total carbon measurements at urban and rural sites in Kenya, East Africa. Atmospheric Environment. 2003;37:1149–1154. [Google Scholar]
- Gatebe CK, Kinyua AM, Mangala MJ, Kwach R, Njau LN, Mukolwe EA, Maina DM. Determination of suspended particulate matter of major significance to human health using nuclear techniques in Kenya. Journal of Radioanalytical and Nuclear Chemistry. 1996;203:125–134. [Google Scholar]
- Gatari MJ, Wagner A, Boman J. Elemental composition of tropospheric aerosols in Hanoi, Vietnam and Nairobi, Kenya. Science of the Total Environment. 2005;341:241–249. doi: 10.1016/j.scitotenv.2004.09.031. [DOI] [PubMed] [Google Scholar]
- Gatari MJ. PhD Thesis. Department of Chemistry, Goteborg University; Goteborg, Sweden: 2006. Studies of Atmospheric Aerosols and Development of Energy Dispersive X-Ray Fluorescence Spectrometer. [Google Scholar]
- Hagler GSW, Bergin MH, Salmon LG, Yu JZ, Wan ECH, Zheng M, Zeng LM, Kiang CS, Zhang YH, Schauer JJ. Local and regional anthropogenic influence on PM2.5 elements in Hong Kong. Atmospheric Environment. 2007;41(28):5994–6004. [Google Scholar]
- HEI International Scientific Oversight Committee. Special Report 18. Health Effects Institute; Boston, MA: 2010. Outdoor Air Pollution and Health in the Developing Countries of Asia: A Comprehensive Review. [Google Scholar]
- Hoek G, Meliefste K, Cyrys J, Lewné M, Bellander T, Brauer M, Fischer P, Gehring U, Heinrich J, van Vliet P, Brunekreef B. Spatial variability of fine particle concentrations in three European areas. Atmospheric Environment. 2002;36:4077–4088. [Google Scholar]
- Ibald-Mulli A, Timonen KL, Peters A, Heinrich J, Wolke G, Lanki T, Buzorius G, Kreyling WG, de Hartog J, Hoek G, ten Brink HM, Pekkanen J. Effects of particulate air pollution on blood pressure and heart rate in subjects with cardiovascular disease: A multicenter approach. Environmental Health Perspectives. 2004;112:369–377. doi: 10.1289/ehp.6523. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jansen KL, Larson TV, Koenig JQ, Mar TF, Fields C, Stewart J, Lippmann M. Associations between health effects and particulate matter and black carbon in subjects with respiratory disease. Environmental Health Perspective. 2005;113:1741–1746. doi: 10.1289/ehp.8153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Japanese International Cooperation Agency (JICA) Final Report. Tokyo: JICA; 2006. The Study on a Master Plan for Urban Transport in the Nairobi Metropolitan Area in the Republic of Kenya. [Google Scholar]
- Kenworthy JR. Automobile Dependence in Bangkok: An International Comparison with Implications for Planning Policies and Air Pollution. In: Fletcher T, McMichael AJ, editors. Health at the Crossroads: Transport Policy and Urban Health. West Sussex, England: John Wiley & Sons; 1997. pp. 215–233. [Google Scholar]
- Kinney PL, Aggarwal M, Northridge M, Janssen NAH, Shepard P. Airborne Concentrations of PM 2.5 and Diesel Exhaust Particles on Harlem Sidewalks: A Community-Based Pilot Study. Environmental Health Perspectives. 2000;108(3):213–218. doi: 10.1289/ehp.00108213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kenya National Bureau of Statistics, Ministry of Planning. Republic of Kenya Economic Survey. 2007 < www.cbs.go.ke>.
- Khayesi M, Monheim H, Nebe JM. Negotiating “streets for all” in urban transport planning: The case for pedestrians, cyclists and street vendors in Nairobi, Kenya. Antipode. 2010;24(1):103–126. [Google Scholar]
- Klopp J, Ngau P, Sclar E. University/City Partnerships: Creating Policy Networks for Urban Transformation in Nairobi. Metropolitan Universities Forthcoming [Google Scholar]
- Laden F, Schwartz J, Speizer FE, Dockery DW. Reduction in Fine Particulate Air Pollution and Mortality: Extended Follow-Up of the Harvard Six Cities Study. American Journal of Respiratory and Critical Care Medicine. 2006;173:667–672. doi: 10.1164/rccm.200503-443OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maina DM, Gatari MJ, Bundi P, Muturi H. Impact of road transport on air quality in Kenya; Roadside survey in the cities of Mombasa and Nairobi; Proceedings of International Aerosol Conference (IAC2006); St Paul Minnesota, USA. 10-15 September 2006.2006. [Google Scholar]
- Ministry of Nairobi Metropolitan Development. Nairobi Metro 2030: A World Class African Metropolis - Building a Safe, Secure and Prosperous Metropolitan. Nairobi: Government of Kenya; 2008. [Google Scholar]
- Ministry of Planning. Republic of Kenya Economic Survey 2007. Nairobi: Kenya National Bureau of Statistics; 2007. < www.cbs.go.ke>. [Google Scholar]
- Ministry of Transport and Communications. Recommendations on Integrated National Transport Policy: Moving a Working Nation. Nairobi: Government of Kenya; 2004. [Google Scholar]
- Ministry of Transport. Sessional Paper on Integrated National Transport Policy. Nairobi: Government of Kenya; 2010. [Google Scholar]
- Nyberg F, Gustavsson P, Järup L, Bellander T, Berglind N, Jakobsson R, Pershagen G. Urban Air Pollution and Lung Cancer in Stockholm. Epidemiology. 2000;7(5):487–495. doi: 10.1097/00001648-200009000-00002. [DOI] [PubMed] [Google Scholar]
- Obudho RA. Nairobi: National Capital and Regional Hub. In: Rakodi Carol., editor. The Urban Challenge in Africa. Tokyo, Japan: United Nations University; 1997. pp. 292–336. [Google Scholar]
- Odhiambo GO, Kinyua AM, Gatebe CK, Awange J. Motor Vehicles Air Pollution in Nairobi, Kenya. Research Journal of Environmental and Earth Sciences. 2010;2(4):178–187. [Google Scholar]
- Pope CA, III, Burnett RT, Thun MJ, Calle EE, Krewski D, Ito K, Thurston GD. Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. Journal of the American Medical Association. 2002;287(9):1132–41. doi: 10.1001/jama.287.9.1132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pope CA, III, Dockery DW. Health effects of fine particulate air pollution: Lines that connect. The Journal of Air and Waste Management Association. 2006;56:709–742. doi: 10.1080/10473289.2006.10464485. [DOI] [PubMed] [Google Scholar]
- Ramanathan V, Carmichael G. Global and regional climate changes due to black carbon. Nature Geoscience. 2008;1:221–227. [Google Scholar]
- Salon D, Gulyani S. Mobility, poverty and gender: Travel ‘choices’ of slum residents in Nairobi, Kenya. Transport Reviews. 2010;30(5):641–657. [Google Scholar]
- Samet J, Zeger S, Dominici F, et al. Research report 94. Cambridge, Mass: Health Effects Institute; 2000. The National Morbidity, Mortality, and Air Pollution Study, Part II: Morbidity and mortality from air pollution in the United States. [PubMed] [Google Scholar]
- Schwartz J. Air pollution and daily mortality: A review and meta-analysis. Environmental Research. 1994;64:36–52. doi: 10.1006/enrs.1994.1005. [DOI] [PubMed] [Google Scholar]
- Schwela D, Haq G, Huizenga C, Han W-J, Fabian H, Ajero M. Urban Air Pollution in Cities; Status, Challenges and Management. London: Earthscan; 2006. [Google Scholar]
- Smith KR. Development, Health and the Risk Transition. In: Shahi G, et al., editors. International Perspectives in Environment, Development and Health. New York: Springer; 1997. pp. 51–62. [Google Scholar]
- Smith KR, Akbar S. Health-Damaging Air Pollution: A Matter of Scale. In: McGranahan G, Murray F, editors. Air Pollution and Health in Rapidly Developing Countries. Canada: Earthscan; 2003. [Google Scholar]
- Sommer H, Künzli N, Seethaler R, Chanel O, Herry M, Masson S, Vergnaud J-C, Filliger P, Horak F, Jr, Kaiser R, Medina S, Puybonnieux-Texier V, Quénel P, Schneider J, Studnicka M. An impact assessment project of Austria, France and Switzerland. New York: OECD Report; 2000. Economic Evaluation of Health Impacts Due to Road Traffic-Related Air Pollution. [Google Scholar]
- United Nations, Department of Economic and Social Affairs. World Urbanization Prospects: The 2009 Revision. New York: United Nations; 2010. [Google Scholar]
- United Nations Environment Programme (UNEP) Kenya: Integrated assessment of the Energy Policy - with Focus on the Transport and Household Energy Sectors. United Nations; 2006. [Google Scholar]
- United Nations Environment Program (UNEP) Urban Air Pollution. 2010 December 14; http://www.unep.org/urban_environment/issues/urban_air.asp.
- van Vliet EDS, Kinney PL. Impacts of roadway emissions on urban particulate matter concentrations in sub-Saharan Africa: new evidence from Nairobi, Kenya. Environmental Research Letters. 2007;2(4) [Google Scholar]
- Volavka-Close N, Sclar ED. Improving Population Health in a Rapidly Urbanizing World. In: Vlahov D, Boufford JI, Pearson C, Norris L, editors. Urban Health; Global Perspectives. San Francisco, California: Jossey Bass; 2010. pp. 453–467. [Google Scholar]
- Wang JS, Chan TL, Ning Z, Leung CW, Cheung CS, Hung WT. Roadside measurement and prediction of CO and PM2.5 dispersion from on-road vehicles in Hong Kong. Transportation Research Part D: Transport and Environment. 2006;11:242–249. [Google Scholar]
- Wong C-M, Vichit-Vadakan V-V, Kan H, Quian Z PAPA Project Teams. Public Health and Air Pollition in Asia (PAPA): A Multicity Study of Short-term Effects of Air Pollution on Mortality. Environmental Health Perspectives. 2008;116:1195–1202. doi: 10.1289/ehp.11257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Woodruff TJ, Parker JD, Schoendorf KC. Fine Particulate Matter (PM2.5) Air Pollution and Selected Causes of Postneonatal Infant Mortality in California. Environmental Health Perspectives. 2006;105:608–612. doi: 10.1289/ehp.8484. [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organization. Air Quality Guidelines: Global Update 2005. Copenhagen, Denmark: World Health Organization Regional Office for Europe; 2006. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Map indicating monitoring locations for Nairobi urban sites and Nairobi’s location in Africa.
Map showing Thika Road and Kenyatta University Location (Rural Background site).