

Every pregnant woman in early spontaneous labor or admitted for induction of labor wishes to know if she will deliver vaginally, or if she will require an operative delivery. Will the energy, pain, and the effect of labor on the pelvic floor be worth a vaginal delivery? What are the consequences of a failed attempt at a vaginal delivery?
It would be ideal if, before the onset of labor or in its early phases, we could accurately predict who will deliver vaginally spontaneously without complications, and who will require an operative delivery (abdominal or assisted). This information would reduce morbidity, improve safety, optimize utilization of resources, and improve satisfaction of women with the labor and/or delivery process. The results of a prospective observational study of 202 nulliparous women suggested that the mode of delivery could be predicted accurately in up to 87% of cases before the onset of labor, with a combination of clinical and historical factors as well as ultrasound findings.1 Sonographic examination has the potential to improve the predictive accuracy – such an improvement is highly desirable.
The partogram was the crucial advance which allowed an objective mean to assess labor progress by plotting cervical dilatation and station as a function of time.2–15 (Figure 1) Before partograms, evaluation of labor progress was subjective and often monitored according to its duration. With the development of the partogram, in the middle part of the twentieth century, labor disorders were defined and classified (prolonged latent phase, protracted, and arrest disorders). The pelvic division of labor, which encompasses the phase of parturition during which the fetus descends through the birth canal, is defined by changes in station of the presenting part.16 It is noteworthy that descent begins before full dilation (Figure 1). The management of protracted descent (nulliparous: 1cm/hour or less; multiparous: 2cm/hour or less), arrest of descent (no change in station for 1 hour or more), or failure to descend (no change in the deceleration phase or the second stage)13 remain one of the most challenging problems of obstetrics. Indeed, the skill and judgment required to decide when and how to intervene have been defining factors of the art of obstetrics.
Figure 1.

Partogram developed by Emanuel Friedman which describes the relationship between time in the horizontal axis and two variables: cervical dilatation and station of the presenting part. Reproduced from: Friedman EA. Dysfunctional labor. In Management of Labor, CohenWR, Friedman EA (eds). University Park Press: Baltimore, 1983: 11-2415.
Operative vaginal deliveries were introduced as a heroic measure to deal with obstructed labor. The feasibility of an abdominal delivery, its improved technique and safety, coupled with a concern for fetal and neonatal welfare have changed the components of the obstetrical equation to opt for a particular mode of delivery (vaginal operative delivery versus abdominal).
Ultrasound has earned its role in obstetrics through the assessment of gestational age, fetal growth, detection of congenital anomalies, fetal well-being and cervical length. In this Editorial, we reaffirm the notion that ultrasound is superior to digital vaginal examinations in determining fetal position prior to operative delivery,17–26 and explore the concept that sonography brings objectivity in assessing the location of the presenting part (station), and may contribute substantially to the clinical management of the second stage of labor. This issue of the “Journal” contains several original contributions which support this view.
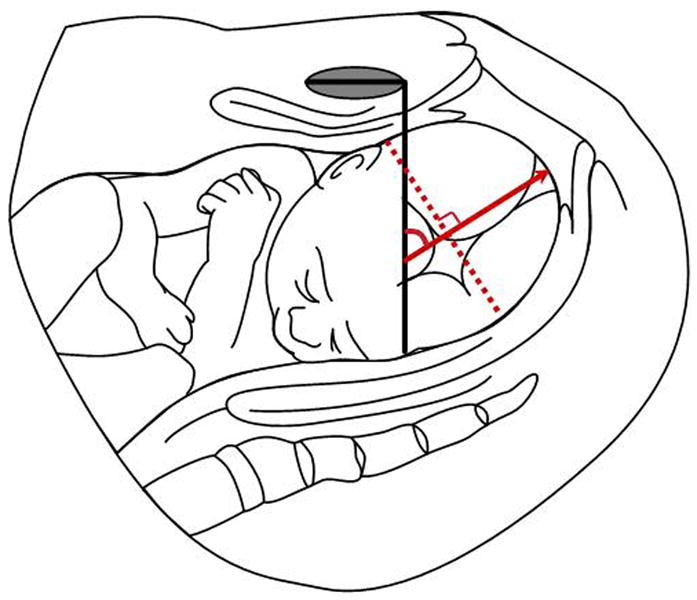
A pioneering study by Antonio Barbera et al.27 (from Professor John Hobbins' group) reports the use of transperineal/translabial ultrasound,28 and describes that the angle between the symphysis pubis and the leading part of the fetal skull (“angle of progression”) can predict which patient would deliver vaginally and which one would be at risk for requiring an abdominal delivery. The concept was originally described in a DVD in 2003 (under the sponsorship of the American College of Obstetricians and Gynecologists).29 The study is now published in this issue of the Journal.27 An angle of progression of 120 degrees or more (Figure 2) was associated in all cases with a spontaneous vaginal delivery. The angle was also associated with the duration of the examination-to-delivery interval. The intra-observer and inter-observer variability of the angle of progression were low, and there was a good correlation between clinical assessment of progress and the angle of progression.
Figure 2.

“Angle of progression”. This is the angle formed between a line placed through the midline of the symphysis pubis, and a second line (in red) drawn from the inferior apex of the symphysis tangentially to the fetal skull. In this figure, the angle of progression is greater than 120 degrees. The original figure was provided by Professor Karim Kalache (Berlin, Germany) and has been slightly modified.
This concept has been independently studied by Professor Karim Kalache at the Charité University Hospital in Berlin, in the Department of Professor Joachim Dudenhausen.30 Among 26 cases with an occiput anterior fetal position, an angle of progression of 120 degrees or more was associated with a probability of successful vaginal delivery of 90% (derived from logistic regression). Collectively, the evidence suggests that the simple determination of the angle of progression has important prognostic value.
Since engagement of the fetal head is a major prognostic factor for the outcome of labor,31–33 and its diagnosis by clinical means has many shortcomings, ultrasound has been used to improve the accuracy of its diagnosis. “Engagement” is said to have occurred when the widest diameter of the fetal presenting part has passed beyond the plane of the maternal pelvic inlet.34 In a cephalic presentation, the head usually is engaged when the leading part of the skull is at or below the level of the maternal ischial spines. The diagnosis of engagement can be made clinically by transvaginal digital examination, or transabdominal examination (using the fourth Leopold maneuver and finding that two-fifths of the fetal head is palpable).35
How accurate is the determination of fetal station and the diagnosis of engagement by digital examination?
Olivier Dupuis et al36 in Lyon, France, made a seminal contribution by rigorously assessing the accuracy of station diagnosis with digital examination. This was accomplished using a birth simulator to systematically examine the reliability of digital examination of residents (average experience of 2 years) and attending physicians (average experience of 9 years) to determine engagement and fetal station. A fetal head mannequin was placed in 11 possible fetal stations in a random order (from -5 to +5) (Figure 3). The error in the diagnosis of station was assessed by the difference between the true station (established by a sensor in the birth simulator), and the station determined by the operator using digital examination.
Figure 3.

The relationship between the bony pelvis and the presenting part to define station. It is generally held that when the largest diameter of the fetal head is at the level of the pelvic inlet, the leading part of the head will be at the level of the ischial spines (station 0). The plus and minus numbers represent centimeters below and above the ischial spines, respectively. Reproduced from: Greenhill JP, Friedman EA. Biological Principles and Modern Practice of Obstetrics. WB Saunders: Philadelphia, 1974 40.
Numerical errors occurred in 50% to 88% of cases in the resident group, and in 36% to 80% of cases in the attending physician group. The mean “group” error for residents was 30% (95% CI: 25% to 35%), and for attendings was 34% (95% CI: 27% to 41%). The mean error rate in the diagnosis of engagement was 12%, and this misdiagnosis was equally distributed between false-positives and false-negatives. Undiagnosed “high” stations accounted for 22.4% of the errors made by residents, and 15.95% of the errors made by attending physicians. Alarmingly, the misdiagnosis of a station as representing mid-pelvic, rather than a true high-pelvic station accounted for 87.5% and 66.8% of the errors made by residents and attending physicians, respectively. This study provides evidence that transvaginal digital examination of fetal head station is not reliable, even though it is the standard practice to determine labor progress in all labor and delivery units around the world. Moreover, station is the determining factor for whether or not an operative vaginal delivery should be performed. High pelvic deliveries (when the head is not engaged) have been abandoned because they are unsafe for mother and fetus. In addition, the risks associated with a mid-pelvic (station is above +2 but the head is engaged), a low and an outlet operative vaginal delivery are different36 (see Table 1 for definitions34).
Table 1. Criteria for types of forceps deliveries.
| Types of Forceps Deliveries | Criteria |
|---|---|
| Outlet Forceps | Scalp is visible at the introitus without separating labia |
| Fetal skull has reached the pelvic floor | |
| Sagittal suture is in anteroposterior diameter, or right or left occiput anterior or posterior position | |
| Fetal head is at or on perineum | |
| Rotation does not exceed 45 degrees | |
| Low Forceps | Leading point of fetal skull is at station ≥ +2 cm and not on the pelvic floor |
| Rotation is 45 degrees or less (left or right occiput anterior to occiput anterior, or left or right occiput posterior to occiput posterior). | |
| Rotation is greater than 45 degrees | |
| Midforceps | Station is above +2 cm but head is engaged |
| High Forceps | Not included in classification |
Reproduced and adapted with permission from: American College of Obstetrics and Gynecology. Operative Vaginal Delivery. Clinical management guidelines for obstetrician-gynecologists. Int J Gynecol Obstet 2001; 74:69-7634.
Evaluation of the fetal head station with ultrasound
Professor Hans Peter Dietz and his team from Sydney, Australia, proposed a simple method to evaluate the station of the fetal head using translabial ultrasound after studying prospectively 140 nulliparous women not in labor.37 A vertical line was drawn from the edge of the pubic symphysis, and then a perpendicular line was drawn to the leading edge of the fetal head (Figure 4). The minimal distance between these two landmarks is what is now referred to as the “head progression distance”. Dietz et al. provided evidence that this parameter correlated with the station of the fetal head by clinical examination (by both abdominal palpation and vaginal digital examination), and that this method was highly reproducible. Even thought the technique was originally described for the assessment of engagement, it may be valuable in the assessment of progress in the second stage of labor.37 The lower the presenting part, the greater the “head progression distance.”
Figure 4.

“Head progression distance”. This diagram describes the parameter originally proposed by Professor Hans Peter Dietz (Sydney, Australia) to assess the degree of descent of the presenting part. A line through the inferoposterior symphyseal margin (parallel to the main transducer axis) is the reference line. The minimal distance between this line and the leading edge of the presenting part is measured (line marked by calipers and is in red) and represents the head progression distance.
Two other studies have compared the methods for the diagnosis of engagement in women in labor. The first compared two clinical methods (transvaginal digital examination versus transabdominal palpation).38 The second compared transvaginal digital examination with transabdominal ultrasound.39 Both studies lacked a gold standard.
The fundamental premise which has been used to label station is that the birth canal is straight (Figure 3). This is not the case: the first part of the birth canal is indeed straight, while the second has a curvilinear trajectory (Figure 5). Barbera et al.41 report in this issue of the Journal a study in which computerized tomography of the pelvis was performed in 70 non-pregnant women. Coordinates were developed to identify specific pelvic landmarks such as the upper and lower border of the symphysis pubis, as well as the right and left ischial spines. This information was used to generate a geometric model of the birth canal which allows calculation of a set of theoretical angles for each station of the fetal head when performing transperineal ultrasound. An angle of 99° corresponded with engagement (station 0), and the range of fetal stations correlated with specific angles. An important finding of this study was that there was a poor correlation between station assessed by digital examination and station assigned by the angles. The discrepancy was greater as the fetal head descended deeper into the birth canal.41 An open question is whether the lack of correlation is due to the proven inaccuracy of digital examination. Clearly, a gold standard is required to resolve this issue.
Figure 5.

A diagram of the birth canal demonstrating that it has a curved trajectory. The presenting part descends in a straight line, and then curves as it approaches the outlet. This figure is reproduced with kind permission from Greenhill JP and Friedman EA, Biological Principles and Modern Practice of Obstetrics; W.B. Saunders Company, 197440.
Position of the fetal head in the birth canal or “head direction”
A collaborative study between the Charité Hospital of the University of Berlin and the Heinrich-Heine-University in Dusseldorf, Germany yielded a series of interesting observations with the potential to improve the assessment of progress in the second stage of labor. Professor Wolfgang Henrich et al42 focused on the study of progress in the second stage of labor by using a transducer translabially to define maternal and fetal landmarks. The main parameters were: 1) the infrapubic line; 2) the widest fetal head diameter; and 3) the head direction (with respect to the long axis of the symphysis pubis) (Figure 6).
Figure 6.
“Head direction” as described by Professor Wolfgang Henrich et al (Berlin, Germany). An infrapubic line (in black) is drawn perpendicular to the long axis of the symphysis pubis. The red dashed line represents the widest fetal head diameter. The head direction is the angle formed between the infrapubic line and another line (red arrow line) drawn perpendicular to the widest diameter of the fetal head. When this line (red arrow line) points ventrally at an angle of 30 degrees or more, it is considered “head up.” For lines below 0 degrees, the direction is called “head down,” and all other angles are considered horizontal.
Head direction was defined by the angle between the infrapubic line and another line drawn perpendicular to the widest diameter of the fetal head. Using this technique, three types of head direction were determined: head down, horizontal, and head up (Figure 6). Henrich et al42 also reported a computerized tomographic 3D reconstruction of the normal female pelvis. Such reconstruction demonstrated that a line parallel to the infrapubic line and 3 cm caudal to it, identified the plane of the ischial spines (0 station). This implies that if the widest fetal head diameter is above the infrapubic line, it also has to be far above the mid-pelvis (0 station). Henrich et al. found that when the widest diameter of the fetal head crosses the infrapubic line (thus approaching or crossing the interspinous plane), and especially if the head is “up”, an operative delivery had a favorable outcome. Poor prognostic signs for vaginal delivery were a lack of descent or lack of passage of the fetal head below the infrapubic line, and a downward or horizontal direction of the head. However, a potential limitation of this approach is that the posterior skull table is not always well-visualized, and therefore, there is some subjectivity in the determination of the widest fetal head diameter.
Dr. Tullio Ghi et al., from the group of Professor Gianluigi Pilu at the University of Bologna, Italy, report in this issue of the Journal a unique study in which a group of patients who reached full dilatation underwent serial translabial sonograms and digital examinations at 15-30 minute intervals until delivery.43 The parameters evaluated were the head direction as described by Henrich et al.42 (downward, horizontal or upward), as well as the degree of rotation of the fetal head. The latter was accomplished by placing the transducer transversely below the symphysis pubis to visualize the midline of the fetal head and classify the degree of rotation as <45° or ≥45°.
The major findings of the study were that: 1) there was a strong relationship between the “direction of the fetal head” determined by translabial ultrasound and the station as determined clinically (Table 2); 2) the orientation of the midline of the fetal head to the AP diameter of the pelvis (referred by the authors as “the degree of rotation of the fetal head”) was also strongly associated with the station of the fetal head; 3) importantly, the combined findings of an upward direction of the fetal head and a rotation of <45° were associated in 95% of cases with a +3 station of the presenting part.43
Table 2.
Relationship between fetal head direction established sonographically and the fetal station as determined by digital examination.
| Ultrasound findings (longitudinal translabial sonogram) | Most frequent station (clinical examination) |
|---|---|
| Head direction downward (n = 57) | ≤ +1 (77%) |
| Head direction horizontal (n = 59) | ≤ +2 (89.8%) |
| Head direction upward (n = 52) | ≥ +3 (88.5%) |
Based on data from Ghi et al. 43.
Ghi et al.43 proposed an approach for the management of the second stage of labor based on ultrasound. Patients with a downward direction of the fetal head would be eligible for an abdominal delivery because the presenting part is above the mid-pelvis. Conversely, those with an upward direction of the fetal head and a degree of rotation of <45° could be delivered vaginally, either spontaneously or through an operative vaginal delivery. The management of the patients with a head in the horizontal position remains uncertain. The optimal method for assessment of progress when the fetal head is in occiput posterior position is a challenge because of the difficulties in interpreting the direction of the fetal head. Indeed, even when the fetal head was close to the outlet, the head tended to remain horizontal, and the angle of rotation could be <45° when the head is still high at the pelvic inlet.
The value of three-dimensional sonography
Most of the studies thus far have relied on two-dimensional sonography. Three-dimensional sonography will add additional information because the simultaneous visualization of an orthogonal plane improves the reliability that the infrapubic line has been obtained in the correct plane, and facilitates the acquisition and analysis of the information. A recent development is the availability of software and hardware specifically designed to objectively assess the progress in the second stage of labor based on three-dimensional sonography. Studies are required to determine the optimal parameters to monitor labor progress, diagnose labor disorders, and predict the likelihood of success of an operative vaginal delivery and neonatal outcome.
The clinical challenge
One of the most difficult dilemmas in clinical obstetrics is that presented by a nulliparous woman at term who had a protracted active phase of labor, received an epidural, and now has a prolonged second stage of labor. The head appears to be low, but there is always uncertainty as to whether this reflects caput. Should this situation be handled with an operative vaginal delivery (forceps or vacuum) or a Cesarean section? An unsuccessful operative vaginal delivery could have serious consequences both to the mother and the fetus. On the other hand, a Cesarean delivery when the head is deep in the birth canal, may also lead to serious complications, such as lacerations of the uterus, vagina and bladder, and even fetal injuries caused during the extraction procedure.45–56
Ultrasound can play a role by: 1) identifying precisely the fetal position; 2) diagnosing whether caput is present and its extent; 3) assessing the fetal station; and 4) documenting the degree of progress that has been made during the second stage, when ultrasound has been used serially. Presently, obstetricians are required to document the station and the position of the fetal head, as well as the rationale for his/her decision. The accumulating body of literature suggests that ultrasound can play an important role in the objective documentation of landmarks and parameters which are valuable to manage this complex obstetrical challenge.
Reference List
- 1.Dietz HP, Lanzarone V, Simpson JM. Predicting operative delivery. Ultrasound Obstet Gynecol. 2006;27:409–15. doi: 10.1002/uog.2731. [DOI] [PubMed] [Google Scholar]
- 2.Calkins LA. On predicting the length of labor: I. First stage. Am J Obstet Gynecol. 1941;42:802–11. [Google Scholar]
- 3.Calkins LA. Second stage of labor: The descent phase. Am J Obstet Gynecol. 1944;48:798–803. [Google Scholar]
- 4.Friedman EA. The graphic analysis of labor. Am J Obstet Gynecol. 1954;68:1568–75. doi: 10.1016/0002-9378(54)90311-7. [DOI] [PubMed] [Google Scholar]
- 5.Friedman EA. Cervimetry: an objective method for the study of cervical dilatation in labor. Am J Obstet Gynecol. 1956;71:1189–93. doi: 10.1016/0002-9378(56)90424-0. [DOI] [PubMed] [Google Scholar]
- 6.Friedman EA, Sachtleben MR. Station of the fetal presenting part. III. Interrelationship with cervical dilatation. Am J Obstet Gynecol. 1965;93:537–42. doi: 10.1016/0002-9378(65)90512-0. [DOI] [PubMed] [Google Scholar]
- 7.Friedman EA, Sachtleben MR. Station of the fetal presenting part. II. Effect on the course of labor. Am J Obstet Gynecol. 1965;93:530–36. doi: 10.1016/0002-9378(65)90511-9. [DOI] [PubMed] [Google Scholar]
- 8.Friedman EA, Sachtleben MR. Station of the fetal presenting part. I. Pattern of descent. Am J Obstet Gynecol. 1965;93:522–29. doi: 10.1016/0002-9378(65)90510-7. [DOI] [PubMed] [Google Scholar]
- 9.Friedman EA, Sachtleben MR. Station of the fetal presenting part. IV. Slope of descent. Am J Obstet Gynecol. 1970;107:1031–34. doi: 10.1016/0002-9378(70)90624-1. [DOI] [PubMed] [Google Scholar]
- 10.Philpott RH, Castle WM. Cervicographs in the management of labour in primigravidae. II. The action line and treatment of abnormal labour. J Obstet Gynaecol Br Commonw. 1972;79:599–602. doi: 10.1111/j.1471-0528.1972.tb14208.x. [DOI] [PubMed] [Google Scholar]
- 11.Philpott RH, Castle WM. Cervicographs in the management of labour in primigravidae. I. The alert line for detecting abnormal labour. J Obstet Gynaecol Br Commonw. 1972;79:592–98. doi: 10.1111/j.1471-0528.1972.tb14207.x. [DOI] [PubMed] [Google Scholar]
- 12.Beazley JM. Use of partograms in labor. Proc R Soc Med. 1972;65:700. doi: 10.1177/003591577206500817. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Friedman EA. Labor: Clinical Evaluation and Management. New York: Appleton-Century-Crofts; 1978. [Google Scholar]
- 14.Bottoms SF, Sokol RJ, Rosen MG. Short arrest of cervical dilatation: a risk for maternal/fetal/infant morbidity. Am J Obstet Gynecol. 1981;140:108–16. doi: 10.1016/0002-9378(81)90264-7. [DOI] [PubMed] [Google Scholar]
- 15.Friedman EA. Dysfunctional Labor. In: Cohen WR, Friedman EA, editors. Management of Labor. Baltimore: University Park Press; 1983. pp. 11–24. [Google Scholar]
- 16.Cohen WR. The pelvic division of labor. In: Cohen WR, Friedman EA, editors. Management of labor. Baltimore: University Park Press; 1983. pp. 41–64. [Google Scholar]
- 17.Gardberg M, Laakkonen E, Salevaara M. Intrapartum sonography and persistent occiput posterior position: a study of 408 deliveries. Obstet Gynecol. 1998;91:746–49. doi: 10.1016/s0029-7844(98)00074-x. [DOI] [PubMed] [Google Scholar]
- 18.Akmal S, Tsoi E, Kametas N, Howard R, Nicolaides KH. Intrapartum sonography to determine fetal head position. J Matern Fetal Neonatal Med. 2002;12:172–77. doi: 10.1080/jmf.12.3.172.177. [DOI] [PubMed] [Google Scholar]
- 19.Sherer DM, Miodovnik M, Bradley KS, Langer O. Intrapartum fetal head position I: comparison between transvaginal digital examination and transabdominal ultrasound assessment during the active stage of labor. Ultrasound Obstet Gynecol. 2002;19:258–63. doi: 10.1046/j.1469-0705.2002.00641.x. [DOI] [PubMed] [Google Scholar]
- 20.Sherer DM, Miodovnik M, Bradley KS, Langer O. Intrapartum fetal head position II: comparison between transvaginal digital examination and transabdominal ultrasound assessment during the second stage of labor. Ultrasound Obstet Gynecol. 2002;19:264–68. doi: 10.1046/j.1469-0705.2002.00656.x. [DOI] [PubMed] [Google Scholar]
- 21.Akmal S, Kametas N, Tsoi E, Hargreaves C, Nicolaides KH. Comparison of transvaginal digital examination with intrapartum sonography to determine fetal head position before instrumental delivery. Ultrasound Obstet Gynecol. 2003;21:437–40. doi: 10.1002/uog.103. [DOI] [PubMed] [Google Scholar]
- 22.Souka AP, Haritos T, Basayiannis K, Noikokyri N, Antsaklis A. Intrapartum ultrasound for the examination of the fetal head position in normal and obstructed labor. J Matern Fetal Neonatal Med. 2003;13:59–63. doi: 10.1080/jmf.13.1.59.63. [DOI] [PubMed] [Google Scholar]
- 23.Dupuis O, Ruimark S, Corinne D, Simone T, Andre D, Rene-Charles R. Fetal head position during the second stage of labor: comparison of digital vaginal examination and transabdominal ultrasonographic examination. Eur J Obstet Gynecol Reprod Biol. 2005;123:193–97. doi: 10.1016/j.ejogrb.2005.04.009. [DOI] [PubMed] [Google Scholar]
- 24.Zahalka N, Sadan O, Malinger G, Liberati M, Boaz M, Glezerman M, et al. Comparison of transvaginal sonography with digital examination and transabdominal sonography for the determination of fetal head position in the second stage of labor. Am J Obstet Gynecol. 2005;193:381–86. doi: 10.1016/j.ajog.2004.12.011. [DOI] [PubMed] [Google Scholar]
- 25.Rozenberg P, Porcher R, Salomon LJ, Boirot F, Morin C, Ville Y. Comparison of the learning curves of digital examination and transabdominal sonography for the determination of fetal head position during labor. Ultrasound Obstet Gynecol. 2008;31:332–37. doi: 10.1002/uog.5267. [DOI] [PubMed] [Google Scholar]
- 26.Rayburn WF, Siemers KH, Legino LJ, Nabity MR, Anderson JC, Patil KD. Dystocia in late labor: determining fetal position by clinical and ultrasonic techniques. Am J Perinatol. 1989;6:316–19. doi: 10.1055/s-2007-999602. [DOI] [PubMed] [Google Scholar]
- 27.Barbera A, Pombar X, Prugino G, Lezotte D, Hobbins J. A new method to assess fetal head descent in labor with transperineal ultrasound. Ultrasound Obstet Gynecol. 2009 doi: 10.1002/uog.6329. [DOI] [PubMed] [Google Scholar]
- 28.Jeanty P, d'Alton M, Romero R, Hobbins JC. Perineal scanning. Am J Perinatol. 1986;3:289–95. doi: 10.1055/s-2007-999882. [DOI] [PubMed] [Google Scholar]
- 29.Barbera A, Becker T, Macfarlane h, Hobbins J. Assessment of fetal head descent in labor with transperineal ultrasound. ACOG. 2003;176 doi: 10.1002/uog.6329. Ref Type: Audiovisual Material. [DOI] [PubMed] [Google Scholar]
- 30.Kalache K, Duckelmann AM, Michaelis S, Lange J, Cichon G, Dudenhausen J. Transperineal ultrasound in prolonged second stage of labor with occipito-anterior presenting fetuses - How well does the angle of progression predict the mode of delivery? Ultrasound Obstet Gynecol. 2009 doi: 10.1002/uog.6294. [DOI] [PubMed] [Google Scholar]
- 31.Falzone S, Chauhan SP, Mobley JA, Berg TG, Sherline DM, Devoe LD. Unengaged vertex in nulliparous women in active labor. A risk factor for cesarean delivery. J Reprod Med. 1998;43:676–80. [PubMed] [Google Scholar]
- 32.Roshanfekr D, Blakemore KJ, Lee J, Hueppchen NA, Witter FR. Station at onset of active labor in nulliparous patients and risk of cesarean delivery. Obstet Gynecol. 1999;93:329–31. doi: 10.1016/s0029-7844(98)00451-7. [DOI] [PubMed] [Google Scholar]
- 33.Murphy K, Shah L, Cohen WR. Labor and delivery in nulliparous women who present with an unengaged fetal head. J Perinatol. 1998;18:122–25. [PubMed] [Google Scholar]
- 34.Operative vaginal delivery. Clinical management guidelines for obstetrician-gynecologists. American College of Obstetrics and Gynecology. Int J Gynaecol Obstet. 2001;74:69–76. doi: 10.1016/s0020-7292(01)00434-9. [DOI] [PubMed] [Google Scholar]
- 35.Crichton D. A reliable method of establishing the level of the fetal head in obstetrics. S Afr Med J. 1974;48:784–87. [PubMed] [Google Scholar]
- 36.Dupuis O, Silveira R, Zentner A, Dittmar A, Gaucherand P, Cucherat M, et al. Birth simulator: reliability of transvaginal assessment of fetal head station as defined by the American College of Obstetricians and Gynecologists classification. Am J Obstet Gynecol. 2005;192:868–74. doi: 10.1016/j.ajog.2004.09.028. [DOI] [PubMed] [Google Scholar]
- 37.Dietz HP, Lanzarone V. Measuring engagement of the fetal head: validity and reproducibility of a new ultrasound technique. Ultrasound Obstet Gynecol. 2005;25:165–68. doi: 10.1002/uog.1765. [DOI] [PubMed] [Google Scholar]
- 38.Knight D, Newnham JP, McKenna M, Evans S. A comparison of abdominal and vaginal examinations for the diagnosis of engagement of the fetal head. Aust N Z J Obstet Gynaecol. 1993;33:154–58. doi: 10.1111/j.1479-828x.1993.tb02381.x. [DOI] [PubMed] [Google Scholar]
- 39.Sherer DM, Abulafia O. Intrapartum assessment of fetal head engagement: comparison between transvaginal digital and transabdominal ultrasound determinations. Ultrasound Obstet Gynecol. 2003;21:430–36. doi: 10.1002/uog.102. [DOI] [PubMed] [Google Scholar]
- 40.Greenhill JP, Friedman EA. Biological Principles and Modern Practice of Obstetrics. Philadelphia: W.B. Saunders; 1974. [Google Scholar]
- 41.Barbera A, Imani F, Becker T, Lezotte D, Hobbins J. The anatomic relationship between the pubic symphysis and the ischial spines and its clinical significance in the assessment of fetal head engagement and station during labor. Ultrasound Obstet Gynecol. 2009 doi: 10.1002/uog.6322. [DOI] [PubMed] [Google Scholar]
- 42.Henrich W, Dudenhausen J, Fuchs I, Kamena A, Tutschek B. Intrapartum translabial ultrasound (ITU): sonographic landmarks and correlation with successful vacuum extraction. Ultrasound Obstet Gynecol. 2006;28:753–60. doi: 10.1002/uog.3848. [DOI] [PubMed] [Google Scholar]
- 43.Ghi T, Farina A, Pedrazzi A, Rizzo N, Pelusi G, Pilu G. Diagnosis of station and rotation of the fetal head in the second stage of labour with intrapartum translabial ultrasound. Ultrasound Obstet Gynecol. 2009 doi: 10.1002/uog.6313. [DOI] [PubMed] [Google Scholar]
- 44.Fuchs I, Tutschek B, Henrich W. Visualization of the fetal fontanels and skull sutures by three-dimensional translabial ultrasound during the second stage of labor. Ultrasound Obstet Gynecol. 2008;31:484–486. doi: 10.1002/uog.5309. [DOI] [PubMed] [Google Scholar]
- 45.Bashore RA, Phillips WH, Jr, Brinkman CR., III A comparison of the morbidity of midforceps and cesarean delivery. Am J Obstet Gynecol. 1990;162:1428–34. doi: 10.1016/0002-9378(90)90902-j. [DOI] [PubMed] [Google Scholar]
- 46.Al Kadri H, Sabr Y, Al Saif S, Abulaimoun B, Ba'Aqeel H, Saleh A. Failed individual and sequential instrumental vaginal delivery: contributing risk factors and maternal-neonatal complications. Acta Obstet Gynecol Scand. 2003;82:642–48. doi: 10.1034/j.1600-0412.2003.00162.x. [DOI] [PubMed] [Google Scholar]
- 47.Murphy DJ, Liebling RE, Verity L, Swingler R, Patel R. Early maternal and neonatal morbidity associated with operative delivery in second stage of labour: a cohort study. Lancet. 2001;358:1203–07. doi: 10.1016/S0140-6736(01)06341-3. [DOI] [PubMed] [Google Scholar]
- 48.Murphy DJ, Liebling RE, Patel R, Verity L, Swingler R. Cohort study of operative delivery in the second stage of labour and standard of obstetric care. BJOG. 2003;110:610–15. [PubMed] [Google Scholar]
- 49.Bhide A, Guven M, Prefumo F, Vankalayapati P, Thilaganathan B. Maternal and neonatal outcome after failed ventouse delivery: comparison of forceps versus cesarean section. J Matern Fetal Neonatal Med. 2007;20:541–45. doi: 10.1080/14767050701412297. [DOI] [PubMed] [Google Scholar]
- 50.Sadan O, Ginath S, Gomel A, Abramov D, Rotmensch S, Boaz M, et al. What to do after a failed attempt of vacuum delivery? Eur J Obstet Gynecol Reprod Biol. 2003;107:151–55. doi: 10.1016/s0301-2115(02)00344-5. [DOI] [PubMed] [Google Scholar]
- 51.Rozenberg P, Gillet A, Ville Y. Transvaginal sonographic examination of the cervix in asymptomatic pregnant women: review of the literature. Ultrasound Obstet Gynecol. 2002;19:302–11. doi: 10.1046/j.1469-0705.2002.00645.x. [DOI] [PubMed] [Google Scholar]
- 52.Glavind K, Bjork J. Incidence and treatment of urinary retention postpartum. Int Urogynecol J Pelvic Floor Dysfunct. 2003;14:119–21. doi: 10.1007/s00192-002-1014-3. [DOI] [PubMed] [Google Scholar]
- 53.Bollard RC, Gardiner A, Duthie GS, Lindow SW. Anal sphincter injury, fecal and urinary incontinence: a 34-year follow-up after forceps delivery. Dis Colon Rectum. 2003;46:1083–88. doi: 10.1007/s10350-004-7284-8. [DOI] [PubMed] [Google Scholar]
- 54.Hughey MJ, McElin TW, Lussky R. Forceps operations in perspective. I. Midforceps rotation operations. J Reprod Med. 1978;20:253–59. [PubMed] [Google Scholar]
- 55.Chiswick ML, James DK. Kielland's forceps: association with neonatal morbidity and mortality. Br Med J. 1979;1:7–9. doi: 10.1136/bmj.1.6155.7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Towner D, Castro MA, Eby-Wilkens E, Gilbert WM. Effect of mode of delivery in nulliparous women on neonatal intracranial injury. N Engl J Med. 1999;341:1709–14. doi: 10.1056/NEJM199912023412301. [DOI] [PubMed] [Google Scholar]