

Abstract
The HER2 oncogene was recently reported to be amplified and overexpressed in esophageal adenocarcinoma. However, the relationship of HER2 amplification in esophageal adenocarcinoma with prognosis has not been well defined. The scoring systems for clinically evaluating HER2 in esophageal adenocarcinoma are not established. The aims of the study were to establish a HER2 scoring system and comprehensively investigate HER2 amplification and overexpression in esophageal adenocarcinoma and its precursor lesion. Using a tissue microarray, containing 116 cases of esophageal adenocarcinoma, 34 cases of BE, 18 cases of low grade dysplasia and 15 cases of high grade dysplasia, HER2 amplification and overexpression were analyzed by HercepTest and CISH methods. The amplification frequency in an independent series of 116 esophageal adenocarcinoma samples was also analyzed using Affymetrix SNP 6.0 microarrays. In our studies, we have found that HER2 amplification does not associate with poor prognosis in total 232 esophageal adenocarcinoma patients by CISH and high density microarrays. We further confirm the similar frequency of HER2 amplification by CISH (18.10%; 21/116) and SNP 6.0 microarrays (16.4%, 19/116) in esophageal adenocarcinoma. HER2 protein overexpression was observed in 12.1 % (14/116) of esophageal adenocarcinoma and 6.67% (1/15) of HGD. No HER2 amplification or overexpression was identified in BE or LGD. All HER2 protein overexpression cases showed HER2 gene amplification. Gene amplification was found to be more frequent by CISH than protein overexpression in esophageal adenocarcinoma (18.10% vs 12.9%). A modified two-step model for esophageal adenocarcinoma HER-2 testing is recommend for clinical esophageal adenocarcinoma HER-2 trial.
Keywords: Barrett’s esophagus, dysplasia, adenocarcinoma, HER2, immunohistochemistry, DNA microarray, tissue microarray, CISH, overexpression, amplification, prognosis
INTRODUCTION
Esophageal adenocarcinoma (EAC) is thought to develop as a result of gastroesophageal reflux (GERD) which initiates a metaplastic change in the lower esophageal epithelium. Accumulation of genetic and epigenetic changes then results in progression to dysplasia and cancer in some individuals.1–2 The incidence of EAC has increased rapidly in the last three decades and the prognosis is usually very poor with 5-year survival rates ranging from 14–22%.3–6 The surgical treatment of EAC can offer cure for some, however, many patients have locally advanced or disseminated disease at presentation and require systemic therapy. Current chemotherapy regimens provide only minimal survival benefit, predominantly when used in combination with surgery or radiation. Identification of genetic alterations in EAC that offer potential for biologically targeted treatment is one of the best hopes to improve the selectivity of therapy and enhance patient survival.
The HER2 (c-erbB2) gene, a proto-oncogene, is located on chromosome 17q11.2–12 and encodes epidermal growth factor receptor 2 (HER2), a transmembrane glycoprotein receptor p185HER2, which is targeted by the humanized monoclonal antibody trastuzumab (Herceptin). 7 HER2 is amplified and overexpressed in approximately 25% of breast cancer patients and is associated with an aggressive clinical course and poor prognosis. 8 Trastuzumab treatment in combination with chemotherapy for breast cancer patients with HER2 amplification/over-expression has shown a significant clinical efficacy in both the metastatic and adjuvant settings.9 In EAC, HER2 overexpression and amplification has been reported at frequencies similar to those observed in breast cancer.8, 10–16 In EAC however, the relationship between HER2 amplification and prognosis is controversial.12, 17 Recent studies have shown that anti-HER2 treatment enhanced radiosensitivity of esophageal cancer cell lines with HER2 overexpression.18 In EAC, although the initial results from nineteen EAC patients did not show significant improvement of patient survival19, ToGA clinical trials in patients with most gastric adenocarcinoma (236 vs 243 patients) and some gastroesophageal junction adenocarcinoma (58 vs 48 patients) have shown a significant survival benefit for patients treated with a combination of Trastuzumab and standard chemotherapy.20,21 The interest for treatment of EAC therefore remains high.
The guidelines for detection and interpretation of HER2 amplification/over-expression in breast cancer have been well established and anti-HER2 targeted treatment is routinely considered in the management of these patients.22 Recently, Hofmann and colleague23 established a modified HER2 Scoring system in gastric cancer to identify suitable patients for enrollment in clinical trastuzumab trial. They found an incomplete moderate to strong basal/lateral membranous HER2 staining pattern and higher rate of tumor heterogeneity in gastric adenocarcinoma compared with breast cancer. However, the clinical assessment of HER2 amplification and overexpression with immunohistochemistry and CISH in EAC is not well defined. In addition, the data on the frequency of HER2 amplification and overexpression in EAC and its precursor lesions including columnar cell metaplasia, Barrett’s esophagus and dysplasia is very limited, particularly in US populations. Therefore, the aims of this study are 1) to comprehensively investigate the frequency of HER2 overexpression and amplification in esophageal EAC and precursor lesion using HER2 IHC, CISH and SNP 6.0 microarray; 2) to establish clinical methods to assess HER2 amplification and overexpression; 3) to determine whether HER2 amplification is a prognostic marker for EAC patients by CISH and high definition microarray in separate large clinical specimen; 4) to determine the relationship of HER2 amplification with clinical factors including sex, age, lymph node metastasis and tumor stage.
MATERIALS AND METHODS
Construction of Tissue Microarray (TMA)
TMAs, containing 38 cases of Barrett’s esophagus (BE), 81 cases of columnar cell metaplasia (CCM), 86 cases of squamous epithelium (SE), 18 cases of low grade dysplasia (LGD), 15 cases of high grade dysplasia (HGD), and 116 cases of EAC, were constructed from the representative areas of formalin-fixed specimens collected between 1997–2005 in the Department of Pathology and Laboratory Medicine, University of Rochester Medical Center/Strong Memorial Hospital, Rochester, New York. Five-micron sections were cut from tissue microarrays and were stained with H&E to confirm the presence of the expected tissue histology within each tissue core. Additional sections were cut for IHC and CISH analysis.
Patients for Tissue Microarrays
All the 116 patients with esophageal adenocarcinoma used for the tissue microarray construction were treated with esophagectomy in Strong Memorial Hospital/University of Rochester between 1997–2005. These patients included 104 males (89.6%) and 12 females (10.4%). The patient age ranged from 34 to 85 years with a mean of 65 years. The follow up period after esophagectomy ranged from 0.03 to 142 months with a mean of 39 months.
Patients for Affymetrix SNP 6.0 Analysis
Frozen tumors were obtained from 116 patients undergoing esophagectomy at the University of Pittsburgh Medical Center, Pittsburgh, PA between 2002 and 2008. Patient age ranged from 43–88 and the cohort consisted of 95 males and 21 females. Final pathologic stages were stage I (28), stage II (31), stage III (49) and stage IV (7). All tumor specimens were evaluated by a pathologist and were determined to be >70% tumor cell representation. Further details of this patient cohort and comprehensive genomic analysis of these tumors is to be published elsewhere. In both institutes, all research was performed under protocols approved at both participating institutions.
Affymetrix SNP 6.0 Analysis
Genomic DNA was isolated using the QiaAmp DNA Mini Kit (Qiagen, CA) and 600ng was used for labeling and array hybridization at the SUNY Upstate Medical University microarray core facility (Syracuse, NY) using kits and protocols provided by Affymetrix. Array data quality was assessed using Affymetrix Genotyping Console (GTC) 3.0 and all further data analysis was performed using Nexus 5.0 Copy Number Analysis software (Biodiscovery, Inc. CA).
Immunohistochemistry (IHC)
Tissue sections from the TMA were deparaffinized, rehydrated through graded alcohols, and washed with phosphate buffered saline (PBS). Antigen retrieval for HER2 was performed by heating sections in 99°C water bath for 40 minutes. After endogenous peroxidase activity was quenched and nonspecific binding was blocked, ready-to-use mouse monoclonal antibody anti-HER2 (DAKO, CA) was incubated at room temperature for 30 minutes. The secondary antibody (Flex HRP) was allowed to incubate for 30 minutes. After washing, sections were incubated with Flex DAB Chromogen for 10 minutes and counterstained with Flex Hematoxylin for 5 minutes. A breast carcinoma with known HER2 overexpression served as positive control. Negative control was performed by replacing anti-HER2 antibody with normal serum.
Chromogenic In Situ Hybridization (CISH)
HER2 CISH was performed according to the manufacturer’s protocol (DAKO DuoCISH kit, DAKO, CA) and stained in the Dako Autostainer. Briefly, TMA sections were deparaffined in xylene, rehydrated through graded alcohols and washed in diluted Wash Buffer for 3 minutes. Endogenous peroxidase was blocked by Peroxidase Block solution for 5 minutes. Sections were subsequently incubated with CISH Antibody Mix for 30 minutes. After washing, sections were incubated with Red Chromogen Solution and Blue Chromogen Solution for 10 minutes, respectively. Sections were counterstained with Hematoxylin, dried and mounted. A breast carcinoma and esophageal adenocarcinoma with known HER2 amplification was used as positive control. Negative control was performed by replacing HER2 probe by normal serum.
Scoring of IHC and CISH
All sections were reviewed independently by Z.Z. and Y.H. blinded to all clinical and pathologic information. Discordant cases were reviewed by D.H. and a final consensus was reached. For HER2 IHC, percentage (0–100%) of positive cells was determined. Gastric HER2 scoring criteria were used for evaluation of these samples. The intensity of HER2 staining was graded as 0, 1+, 2+, or 3+. HER2 protein was considered overexpressed if 10% or more of cells stained with a moderate to strong intensity and showed either complete or a basal/lateral membrane staining pattern (Fig 2). The luminal part of well to moderately differentiated tumor glands often show negative stain. This pattern is also observed in gastric adenocarcinoma 23. For HER2 CISH, the hybridization signals were counted in 50 nuclei per tissue core (Fig. 3). All overlapping nuclei were excluded, only nuclei with a distinct nuclear border were evaluated. The ratio between HER2 and chromosome 17 centromere copy numbers was calculated. The HER2 gene was considered as amplification when the ratio of gene-specific: centromere probe signals was ≥2.0.
Figure 2.

Chromogenic in situ hybridization (CISH) showing HER2 gene normal (A) and amplification (B) in esophageal adenocarcinoma (× 1000). (red signals: HER2; blue signals: chromosome 17)
Figure 3.

HER2 immunohistochemical staining showing 0 immunostaining (A, ×400), 1+ immunostaining (B, × 400), 2+ immunostaining (C, × 400) and 3+ immunostaining (D, × 400) in esophageal adenocarcinoma. Both 2+ and 3+ uniform staining are considered as HER2 protein overexpression. Incomplete membranous “U” shape stain is presented in B.
Statistical analysis
Kaplan-Meir survival estimator and logrank test was used to analyze the patient survival between HER2 amplified group and non- HER2 amplified group. Both a univariate model with HER2 as the soul explanatory variable and a multivariate model with several other clinical covariates, including gender, age, lymph node metastasis and tumor stage, were used. In addition, Fisher’s exact test and Chi-square test were used to compare HER2 positivity rate between EAC, high and low grade dysplasia, CCM and SE subpopulations. p-value less than 0.05 is considered statistically significant.
RESULTS
Defining the HER2/ERBB2 Amplicon in EAC With High Density microarrays
Analysis of 116 EAC specimens using high density microarrays revealed amplification in 16.4% (19/116). In 8.6% (10/116), amplification was considered high level (log2 ratio >0.6). The minimal region of amplification spans 68kb (Figure 1) and contains only 3 genes (ERBB2, C17orf37 and GRB7). In this cohort study, the median overall survival of HER2 amplification is 21 months and non- HER2 amplification is 25 months. No association was found with HER2 amplification and either disease free survival (p=0.709) or overall survival (p=0.27).
Figure 1.
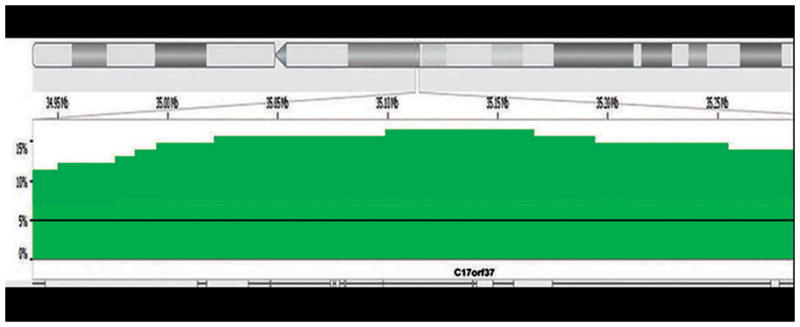
Frequency histogram showing amplification of the ERBB2 (HER2) locus at chromosome 17q12 in 116 esophageal adenocarcinoma samples. The minimal amplicon (peak) spans 68kb and contains only three genes, ERBB2, C17orf37 and GRB7. This locus is amplified in 19/116 (16.4%) cases in this patient cohort, approximately half of which are considered high copy amplification events (darker green).
CISH analysis
The HER2 CISH results are summarized in Table 1. No HER2 gene amplification was identified in esophageal SE (n=86), CCM (n=81), BE (n=34) and LGD (n=18). One of 15 cases of HGD (6.67%) showed HER2 gene amplification (Table 1) and 21 of 116 cases of EAC (18.10%) showed HER2 gene amplification (Table 1, Figure 2). EAC showed statistically significant higher HER2 gene amplification compared to the LGD, BE, CCM, and SE groups (p<0.05), but not when compared to HGD group (p>0.05).
Table 1.
Results of immunohistochemistry for HER2 oncoprotein overexpression and CISH for HER2 gene amplification in esophageal squamous epithelium, CCM, BE, dysplasia and adenocarcinoma.
| * Tissue | n | HER2 overexpression | HER2 amplification | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| SE | 86 | 0 | 0 | 0 | 0 |
| CCM | 81 | 0 | 0 | 0 | 0 |
| BE | 34 | 0 | 0 | 0 | 0 |
| LGD | 18 | 0 | 0 | 0 | 0 |
| HGD | 15 | 1 | 6.67 | 1 | 6.67 |
|
| |||||
| EAC | 116 | 14^ | 12.07 | 21 | 18.10 |
SE, squamous epithelium; CCM, columnar cell metaplasia; BE, Barrett’s esophagus; LGD, low grade dysplasia; HGD, high grade dysplasia; EAC, esophageal adenocarcinoma.
11 cases with positive HER2 IHC from TMA and 3 cases from whole slides.
Immunohistochemical Analysis
The HER2 immunohistochemical staining results are summarized in Table 1 and Figure 3. No HER2 protein overexpression was identified in esophageal SE (n=86), CCM (n=81), BE (n=34) and LGD (n=18). One of 15 cases of HGD (6.67%) showed HER2 overexpression (Table 1). 11 of 116 cases of EAC (9.48%) showed HER2 overexpression from TMA (Table 1, Figure 2). The whole slides from 10 cases with HER2 amplification and non-HER2 overexpression were used to investigate the heterogeneity of HER2 overexpression. Three cases in whole slides showed focal positive IHC (2+). Total 14 of 116 cases of EAC (12.07%) showed HER2 overexpression. EAC showed statistically significant higher HER2 protein overexpression compared to the LGD, BE, CCM, and SE groups (p<0.05), but not when compared to HGD group (p>0.05).
Association between Immunohistochemical and CISH Analyses
The correlation between HER2 protein overexpression by IHC and HER2 gene amplification by CISH in 116 cases of EAC is summarized in Table 2. All 14 cases of EAC with HER2 protein overexpression identified by IHC also showed HER2 gene amplification by CISH. Ten cases with HER2 gene amplification identified by CISH showed HER2 protein overexpression in 3 cases with whole slides IHC (Table 2). No HER2 expression showed in the other seven cases. Total 95 cases (81.90%) of EAC showed neither HER2 protein overexpression nor HER2 gene amplification. Concordance between IHC and CISH was 76%.
Table 2.
Correlation between immunohistochemistry (IHC) and chromogenic in situ hybridization (CISH) in esophageal adenocarcinoma
| IHC score | |||||
|---|---|---|---|---|---|
| 3+ | 2+ | 1+ | 0 | Total | |
| CISH+ | 5 | 9* | 3 | 4 | 21 |
|
| |||||
| CISH− | 0 | 0 | 6 | 89 | 95 |
|
| |||||
| Total | 5 | 9 | 9 | 93 | 116 |
• Including 3 cases on whole slides with 2+ IHC staining.
Association of HER 2 amplification with survival and other clinical factors
The median survival after esophagectomy between HER2 amplification group and no HER2 amplification group is 25 and 23 months, respectively by CISH. A survival analysis was based on Cox regression and log-rank test showed that there is no statistical significance in overall survival between the two groups (p=0.19, Figure 4). When this regression was refit by using one of the following clinical covariates: age, gender, the stage, and metastatic lymph nodes of the tumor, instead of HER2, we found that age (p=0.064) and gender (p=0.448) were not significantly associated with patient survival, but the stage (p<0.001) and the number of metastatic lymph nodes of the tumor (p<0.001) have strong association with patient survival.
Figure 4.
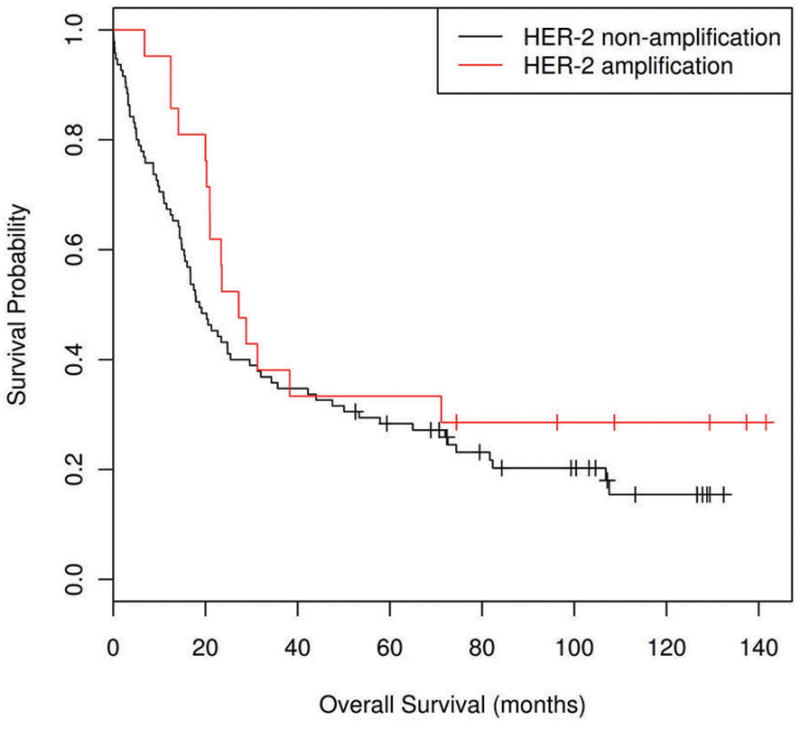
Kaplan-Meier analysis showing there was no survival difference between HER2 amplification group (n=21) and non-HER2 amplification group (n=95) (p=0.19).
In addition, we studied the association between HER2 amplification and these clinical factors (Table 3). Of 116 EAC patients, 21 had HER2 amplification. Nineteen were male, and 2 female (M:F ratio, 9.5:1), with a mean age of 63 years (range, 51 to 74 years). The remaining patients (85 males and 10 females [M:F ratio, 8.5:1]; mean age, 85 years [34 to 85 years]) had no amplification. A Fisher’s exact test shows that there is no significant association between HER2 and gender (p=1.0), age (p =0.188,), the stage (p =0.325), and the number of metastatic lymph nodes (p =0.234). However, the frequency of HER2 amplification was found to be significantly higher (p=0.004) in moderately differentiated tumors (13/22) compared with poor or well differentiated tumors (1/6 and 7/61 respectively).
Table 3.
Association of HER2 amplified group and non-HER2 amplified group with multiple clinical factors
| HER2 amplified | HER2 non-amplified | p value | |||
|---|---|---|---|---|---|
| AGE | 63 (51–74) | 65 (34–85) | 0.188 | ||
| GENDER | MALE | FEMAL | MALE | FEMAL | 1.0 |
| 19 | 2 | 85 | 10 | ||
| POS | NEG | POS | NEG | ||
| LN METASTASIS | 13 | 8 | 69 | 26 | 0.234 |
| pSTAGING | 0.325 | ||||
| I | 3 | 10 | |||
| II | 8 | 25 | |||
| III | 10 | 60 | |||
| Median survival (months) | 25 (7–71) | 23 (0.03–108) | 0.19 | ||
| Differentiation | 0.004 | ||||
| poor | 7 | 61 | |||
| moderate | 13 | 22 | |||
| well | 1 | 6 |
DISCUSSION
In the present study, we provide evidence that HER2 amplification does not associate with poor prognosis in total 232 EAC patients by CISH (116 patients) and high density microarrays (116 patients). We further confirm the frequency of HER2 amplification and overexpression in EAC and high grade dysplasia (see table 1) by various methods including high density microarrays, CISH and IHC. In addition, we recommend a modified 2-step model for clinical HER2 study in EAC patients, similar to what has been proposed for the HER2 evaluation of gastric adenocarcinomas.23
Data on the association between HER2 amplification and survival duration in EAC are limited and conflicting. Brien et al.17 found that patients with HER2 amplification (n=11) had shorter survival durations than did patients without amplification (n=43). However, Reichelt et al.12 found no survival difference between the HER2 (n=16) and no HER2 amplification groups (n=90)(p=0.953). In addition, Rauser et al.28 found that HER2 gene amplification was associated with increased disease-specific mortality on 3-dimensional fluorescence in situ hybridization (FISH) analysis in thick slides (16 μm), but not on FISH and immunohistochemical analyses in thin (4 μm) sections. Our results indicate no association of HER2 amplification with patient survival in a large cohort studies (total 232 patients) by both CISH and high density microarrays.
In EAC, recently Reichelt et al. 12 found that 15% (16/110) of tumors had HER2 gene amplification with FISH. Similarly, Brien et al. showed that 19% (12/63) of EACs had HER2 gene amplification.17 In addition, with 3-dimentional FISH method in thick slides (16 μm, n=124), Rauser et al.24 found that HER2 amplification was 10.5% in high-level amplification (≥ 6.0 signals) and 59.7% in low-level copy number change ( ≥ 2.5–4.0 signals). However, in thin slides (4 μm, n=123), HER2 amplification was found in 9.3 % in high-level amplification (≥ 6.0 signals) and 5.6 % in low-level copy number change ( ≥ 2.5–4.0 signals). In the current study, we found that HER2 amplification was 18% (21/116) detected by CISH and 16.4% (19/116) by high definition microarray in cases of EAC. In addition we found no evidence of HER2 amplification in LGD, BE, CCM or normal esophageal SE. Thus, the frequency of HER2 amplification in EAC appears to be consistent between studies with a range of 15–19% and this event appears not to occur prior to the development of HGD. However, there is a huge difference between traditional FISH in thin section (5.6%) and three-dimensional FISH in thick section (59.7%) to detect the low-level HER2 amplification. They considered that the tumor cell nuclei were truncated due to standarized thin tissue sectioning. Therefore, three dimension FISH need to be further evaluated to help better understand any prognostic significance.
With previous gene amplification with PCR and microarray analysis, the 17q gain was found in various percentage from 21–33 % in Albrecht et al.25(n=18), van Dekken et al.26(n=28) and Miller et al 27 (n=87). In current studies with high definition microarray analysis, 16.4% (19/116) had HER2 amplification detected. The incidences of amplification defined by high density microarrays in our study is close to reported FISH and CISH results, but lower than those of previous studies.
The guidelines for detection and interpretation of HER2 amplification/over-expression in breast cancer have been well established and anti-HER2 targeted treatment is routinely considered in the management of these patients.22, 28–30 Recently, HER2 scoring for gastric cancer has been modified due to HER2 stain pattern and heterogeneity,17 which helps to improve the concordance between IHC and FISH and will help select the most appropriate HER2 positive patients for clinical trials with a combination of Trastuzumab and standard chemotherapy. The guideline for HER2 scoring in EAC is critical for enrolling patient for clinical trial. In our study, all HER2 with 2+ and 3+ expression cases identified with IHC showed HER2 amplification with CISH. The result is similar to the results of Reichelt’s study from Germany,12 but it does not agree to the gastric carcinoma studies. 23 With 2+ expression of HER2, only 36% of IHC 2+ cases were also FISH positive in gastric carcinoma. There are many causes of disagreement including IHC reactivity of EAC, antibody, IHC stain methods, tissue fixation condition and etc. Actually, the HercepTest kit (DACO) was used in both studies. In addition, our studies were repeated several times in different IHC methods for the best results. In our study, modified 2-step model is recommended for the guideline of clinical HER2 study in EAC. In this model, IHC is first used to detect HER2 overexpression with 2+ and 3+ intensity and >10% of positive cells. If HER2 protein is overexpressed, HER2 DNA amplification can be assumed, and CISH analysis may not needed. If HER2 protein is not overexpressed, CISH or FISH analysis should be performed to rule out gene amplification. The HER2 gene was considered as amplification when the ratio of gene-specific: centromere probe signals was ≥2.0 in our study, which is also the criteria used by Hoffman and colleagues23. The definition for HER2 overexpression should be 2+ and 3+ instead of 3+ only in breast and gastric cancer since all 2+ expression cases in EAC showed HER2 amplification by CISH. The negative expression of HER2 in EAC also need to do CISH since 4 of 89 patients show positive for CISH test with negative IHC HER2 expression. In addition, the “U” shaped stain pattern in EAC without complete membrane is common pattern in well differentiated EAC, which is considered as positive IHC stain. The heterogeneity of HER2 overexpression in gastric adenocarcinoma is higher than that in breast cancer.23 We also found that the heterogeneity in EAC is in our preliminary data in ten CISH positive and IHC negative cases. There is a potential problem to evaluate HER2 overexpression of the biopsy specimen in clinical practice. The heterogeneity will be further studied in following research. At present, HER2 tests in multiple biopsies of EAC and gastric adenocarcinoma are recommended in biopsy only specimen.
For our study, we used CISH instead of FISH because of the increased stability of the CISH labeled slides and the ease of interpretation of results which does not require a fluorescent microscope and dark room. Furthermore the use of a light microscope allows us to see both signals and morphology simultaneously. Our experience and that of other groups showed that CISH results are equivalent to FISH and that CISH is a reliable method for detecting HER2 genomic abnormalities.31–32 While both have similar turnaround time and cost in the laboratory, the DNA-specific probes for CISH are 25–50% cheaper than those for FISH.31 Because of the disadvantages of FISH, CISH has shown a great potential to replace FISH for detecting HER2 gene amplificaiton.32 In addition, our results showed that CISH is more sensitive than IHC to detect HER2 abnormalities. This may be because DNA is more stable than protein during the specimen processing. However, the amplification without overexpression in some tumors also was reported12.
In summary, our study showed that HER2 is overexpressed at the protein level and amplified at the DNA level in a subset of esophageal adenocarcinoma and high grade dysplasia. We observed neither HER2 protein overexpression nor DNA amplification in normal esophageal squamous epithelium, columnar cell metaplasia, Barrett’s esophagus or low grade dysplasia. Modified 2-step model for the evaluation of the HER2 status in EAC is suggested by our studies. Our results showed that HER2 amplification is not a prognostic predictor for esophageal adenocarcinoma. However, HER2 amplification/overexpression in a subset of esophageal adenocarcinoma and high grade dysplasia and suggests that these patients would be potential candidates for anti-HER2 targeted treatment.
Acknowledgments
Thanks Dr. Jorge Yao for TMA construction; Qi Yang for immunohistochemistry and CISH study.
Footnotes
Disclosure/conflict of interest: All authors declare no conflict of interest.
References
- 1.Bailey T, Biddlestone L, Shepherd N, et al. Altered cadherin and catenin complexes in the Barrett’s esophagus-dysplasia-adenocarcinoma sequence: correlation with disease progression and dedifferentiation. The American journal of pathology. 1998;152(1):135–44. [PMC free article] [PubMed] [Google Scholar]
- 2.Maru DM, Singh RR, Hannah C, et al. MicroRNA-196a is a potential marker of progression during Barrett’s metaplasia-dysplasia-invasive adenocarcinoma sequence in esophagus. The American journal of pathology. 2009;174(5):1940–8. doi: 10.2353/ajpath.2009.080718. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Gamliel Z, Krasna MJ. Multimodality treatment of esophageal cancer. Surg Clin North Am. 2005;85(3):621–30. doi: 10.1016/j.suc.2005.01.011. [DOI] [PubMed] [Google Scholar]
- 4.Luketich JD, Alvelo-Rivera M, Buenaventura PO, et al. Minimally invasive esophagectomy: outcomes in 222 patients. Annals of surgery. 2003;238(4):486–94. doi: 10.1097/01.sla.0000089858.40725.68. discussion 94–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Swanson SJ, Batirel HF, Bueno R, et al. Transthoracic esophagectomy with radical mediastinal and abdominal lymph node dissection and cervical esophagogastrostomy for esophageal carcinoma. Ann Thorac Surg. 2001;72(6):1918–24. doi: 10.1016/s0003-4975(01)03203-9. discussion 24–5. [DOI] [PubMed] [Google Scholar]
- 6.Pohl H, Welch HG. The role of overdiagnosis and reclassification in the marked increase of esophageal adenocarcinoma incidence. J Natl Cancer Inst. 2005;97(2):142–6. doi: 10.1093/jnci/dji024. [DOI] [PubMed] [Google Scholar]
- 7.Baselga J, Tripathy D, Mendelsohn J, et al. Phase II study of weekly intravenous recombinant humanized anti-p185HER2 monoclonal antibody in patients with HER2/neu-overexpressing metastatic breast cancer. J Clin Oncol. 1996;14(3):737–44. doi: 10.1200/JCO.1996.14.3.737. [DOI] [PubMed] [Google Scholar]
- 8.Slamon DJ, Clark GM, Wong SG, et al. Human breast cancer: correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science. 1987;235(4785):177–82. doi: 10.1126/science.3798106. [DOI] [PubMed] [Google Scholar]
- 9.Goldenberg MM. Trastuzumab, a recombinant DNA-derived humanized monoclonal antibody, a novel agent for the treatment of metastatic breast cancer. Clin Ther. 1999;21(2):309–18. doi: 10.1016/S0149-2918(00)88288-0. [DOI] [PubMed] [Google Scholar]
- 10.Rossi E, Villanacci V, Bassotti G, et al. Her-2/neu in barrett esophagus: a comparative study between histology, immunohistochemistry, and fluorescence in situ hybridization. Diagn Mol Pathol. 2006;15(3):125–30. doi: 10.1097/01.pdm.0000213455.22527.f7. [DOI] [PubMed] [Google Scholar]
- 11.Rossi E, Grisanti S, Villanacci V, et al. Her-2 Overexpression/Amplification in Barrett’s Esophagus Predicts Early Transition from Dysplasia to Adenocarcinoma: A Clinico-Pathologic Study. J Cell Mol Med. 2008 doi: 10.1111/j.1582-4934.2008.00517.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Reichelt U, Duesedau P, Tsourlakis M, et al. Frequent homogeneous HER-2 amplification in primary and metastatic adenocarcinoma of the esophagus. Mod Pathol. 2007;20(1):120–9. doi: 10.1038/modpathol.3800712. [DOI] [PubMed] [Google Scholar]
- 13.Langer R, Von Rahden BH, Nahrig J, et al. Prognostic significance of expression patterns of c-erbB-2, p53, p16INK4A, p27KIP1, cyclin D1 and epidermal growth factor receptor in oesophageal adenocarcinoma: a tissue microarray study. Journal of clinical pathology. 2006;59(6):631–4. doi: 10.1136/jcp.2005.034298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Dreilich M, Wanders A, Brattstrom D, et al. HER-2 overexpression (3+) in patients with squamous cell esophageal carcinoma correlates with poorer survival. Dis Esophagus. 2006;19(4):224–31. doi: 10.1111/j.1442-2050.2006.00570.x. [DOI] [PubMed] [Google Scholar]
- 15.Slamon DJ, Godolphin W, Jones LA, et al. Studies of the HER-2/neu proto-oncogene in human breast and ovarian cancer. Science. 1989;244(4905):707–12. doi: 10.1126/science.2470152. [DOI] [PubMed] [Google Scholar]
- 16.Zhang D, Salto-Tellez M, Do E, Putti TC, Koay ES. Evaluation of HER-2/neu oncogene status in breast tumors on tissue microarrays. Human pathology. 2003;34(4):362–8. doi: 10.1053/hupa.2003.60. [DOI] [PubMed] [Google Scholar]
- 17.Brien TP, Odze RD, Sheehan CE, McKenna BJ, Ross JS. HER-2/neu gene amplification by FISH predicts poor survival in Barrett’s esophagus-associated adenocarcinoma. Human pathology. 2000;31(1):35–9. doi: 10.1016/s0046-8177(00)80195-1. [DOI] [PubMed] [Google Scholar]
- 18.Sato S, Kajiyama Y, Sugano M, et al. Monoclonal antibody to HER-2/neu receptor enhances radiosensitivity of esophageal cancer cell lines expressing HER-2/neu oncoprotein. Int J Radiat Oncol Biol Phys. 2005;61(1):203–11. doi: 10.1016/j.ijrobp.2004.05.017. [DOI] [PubMed] [Google Scholar]
- 19.Safran H, Dipetrillo T, Akerman P, et al. Phase I/II study of trastuzumab, paclitaxel, cisplatin and radiation for locally advanced, HER2 overexpressing, esophageal adenocarcinoma. Int J Radiat Oncol Biol Phys. 2007;67(2):405–9. doi: 10.1016/j.ijrobp.2006.08.076. [DOI] [PubMed] [Google Scholar]
- 20.Jorgensen JT. Target HER2 treatment in advanced gastric cancer. Oncology. 2010;78(1):26–33. doi: 10.1159/000288295. [DOI] [PubMed] [Google Scholar]
- 21.Bang YJ, Van Cutsem E, Feyereislova A, et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label, randomised controlled trial. Lancet. 2010;376(9742):687–97. doi: 10.1016/S0140-6736(10)61121-X. [DOI] [PubMed] [Google Scholar]
- 22.Wolff AC, Hammond ME, Schwartz JN, et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for human epidermal growth factor receptor 2 testing in breast cancer. Arch Pathol Lab Med. 2007;131(1):18–43. doi: 10.5858/2007-131-18-ASOCCO. [DOI] [PubMed] [Google Scholar]
- 23.Hofmann M, Stoss O, Shi D, et al. Assessment of a HER2 scoring system for gastric cancer: results from a validation study. Histopathology. 2008;52(7):797–805. doi: 10.1111/j.1365-2559.2008.03028.x. [DOI] [PubMed] [Google Scholar]
- 24.Rauser S, Weis R, Braselmann H, et al. Significance of HER2 low-level copy gain in Barrett’s cancer: implications for fluorescence in situ hybridization testing in tissues. Clin Cancer Res. 2007;13(17):5115–23. doi: 10.1158/1078-0432.CCR-07-0465. [DOI] [PubMed] [Google Scholar]
- 25.Albrecht B, Hausmann M, Zitzelsberger H, et al. Array-based comparative genomic hybridization for the detection of DNA sequence copy number changes in Barrett’s adenocarcinoma. The Journal of pathology. 2004;203(3):780–8. doi: 10.1002/path.1576. [DOI] [PubMed] [Google Scholar]
- 26.van Dekken H, Geelen E, Dinjens WN, et al. Comparative genomic hybridization of cancer of the gastroesophageal junction: deletion of 14Q31-32.1 discriminates between esophageal (Barrett’s) and gastric cardia adenocarcinomas. Cancer research. 1999;59(3):748–52. [PubMed] [Google Scholar]
- 27.Miller CT, Moy JR, Lin L, et al. Gene amplification in esophageal adenocarcinomas and Barrett’s with high-grade dysplasia. Clin Cancer Res. 2003;9(13):4819–25. [PubMed] [Google Scholar]
- 28.Cobleigh MA, Vogel CL, Tripathy D, et al. Multinational study of the efficacy and safety of humanized anti-HER2 monoclonal antibody in women who have HER2-overexpressing metastatic breast cancer that has progressed after chemotherapy for metastatic disease. J Clin Oncol. 1999;17(9):2639–48. doi: 10.1200/JCO.1999.17.9.2639. [DOI] [PubMed] [Google Scholar]
- 29.Joensuu H, Kellokumpu-Lehtinen PL, Bono P, et al. Adjuvant docetaxel or vinorelbine with or without trastuzumab for breast cancer. N Engl J Med. 2006;354(8):809–20. doi: 10.1056/NEJMoa053028. [DOI] [PubMed] [Google Scholar]
- 30.Wolff AC, Hammond ME, Schwartz JN, et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for human epidermal growth factor receptor 2 testing in breast cancer. J Clin Oncol. 2007;25(1):118–45. doi: 10.1200/JCO.2006.09.2775. [DOI] [PubMed] [Google Scholar]
- 31.Mayr D, Heim S, Weyrauch K, et al. Chromogenic in situ hybridization for Her-2/neu-oncogene in breast cancer: comparison of a new dual-colour chromogenic in situ hybridization with immunohistochemistry and fluorescence in situ hybridization. Histopathology. 2009 doi: 10.1111/j.1365-2559.2009.03427.x. [DOI] [PubMed] [Google Scholar]
- 32.Gong Y, Sweet W, Duh YJ, et al. Chromogenic in situ hybridization is a reliable method for detecting HER2 gene status in breast cancer: a multicenter study using conventional scoring criteria and the new ASCO/CAP recommendations. Am J Clin Pathol. 2009;131(4):490–7. doi: 10.1309/AJCPI00TVGIGYXAA. [DOI] [PubMed] [Google Scholar]