

Abstract
Both implicit and explicit cognitions play an important role in the development of addictive behavior. This study investigated the influence of a single-session motivational interview (MI) on implicit and explicit alcohol-related cognition and whether this intervention was successful in consequently decreasing alcohol use in at-risk adolescents. Implicit and explicit alcohol-related cognitions were assessed at pretest and one month posttest in 125 Dutch at-risk adolescents ranging in age from 15 to 23 (51 males) with adapted versions of the Implicit Association Test (IAT) and an expectancy questionnaire. Motivation to change, alcohol use and alcohol-related problems were measured with self-report questionnaires, at pretest, at posttest after one month, and at the six-month follow-up. Although the quality of the intervention was rated positively, the results did not yield support for any differential effects of the intervention on drinking behavior or readiness to change at posttest and six-month follow-up. There were indications of changes in implicit and explicit alcohol-related cognitions between pretest and posttest. Our findings raise questions regarding the use of MI in this particular at-risk adolescent population and the mechanisms through which MI is effective.
Keywords: implicit cognition, explicit cognition, adolescence, alcohol use, motivational interviewing
Dual process models predict that both implicit and explicit cognitive processes influence behavior (e.g. Strack & Deutsch, 2004). Implicit cognitive processes represent relatively automatic underlying motivational processes, while explicit cognitions are related to slower deliberate thought processes that may inhibit more automatic, impulsive thinking and behavior (Greenwald & Banaji, 1995; Strack & Deutsch, 2004). In addiction research, both implicit alcohol associations and explicit alcohol expectancies have been shown to predict unique variance in concurrent and prospective alcohol use (e.g., Goldman & Darkes, 2004; Jones, Corbin, & Fromme, 2001; Stacy, 1997; Thush & Wiers, 2007).
Furthermore, dual process models of addiction predict that the influence of implicit appetitive processes on subsequent addictive behavior can be reduced by explicit deliberate processes that are dependent on moderators such as motivation and executive functioning (e.g., Stacy, Ames, & Knowlton, 2004; Wiers et al., 2007). In line with this notion, recent studies indicated that the impact of implicit alcohol cognitions on alcohol use in at-risk adolescents was moderated by working memory capacity (Grenard et al., 2008; Thush et al., 2008). In addition to the ability to refrain from more impulsive use of alcohol, it is also important that adolescents are motivated to do so. Indeed, prior research has shown that the influence of implicit processes on behavior increases when motivation not to act on these automatic associations is low (Olson & Fazio, 2004).
The importance of having adaptive motivational structures in the context of changing one’s tendencies toward more addictive behaviors has been demonstrated by a large body of research (Miller & Rollnick, 2002). Research showed that individuals with more adaptive motivational structures (e.g., having positive life goals) demonstrated that they are better able to control their drinking than those with maladaptive motivational structure. In addition, research showed that in treatment, alcohol abusers with adaptive motivational structures show a more immediate response to treatment, less problem denial, and more motivation for change than those with maladaptive motivational structures (Cox & Klinger, 2002).
Indeed, brief interventions that use the technique of motivational interviewing (MI; Miller & Rollnick, 2002) have consistently yielded greater support for their efficacy to reduce hazardous drinking in young adults compared with educational or information-only interventions (e.g. Marlatt et al., 1998; for review, see Larimer & Cronce, 2002, 2007). However, although brief MI has been proven to be effective in reducing hazardous drinking in young adult populations and there have been some MI outcome studies on other drug use that showed positive intervention effects (e.g., McCambridge & Strang, 2004), there is little research yet and largely mixed evidence for the effectiveness of MI in reducing alcohol use in (at-risk) adolescents (for review, see Grenard, Ames, Pentz & Sussman, 2006). Furthermore, only a few studies have tried to identify the cognitive mechanisms through which MI might work (e.g., Bosari & Carey, 2000; Wood, Capone, Laforge, Erickson, & Brand, 2007). Still, motivational interventions represent one of the most promising approaches especially in difficult at-risk, nontreatment-seeking populations (Grenard et al., 2007; Moyer, Finney, Swearingen, & Vergun, 2002).
This study investigated the influence of MI on implicit and explicit alcohol-related cognitions and alcohol use in at-risk adolescents in a randomized field study. It was hypothesized that in the experimental group, motivation to change and negative expectancies (two related concepts; Jones & McMahon, 1998) would increase compared with the information-only control group. Second, it was hypothesized that the experimental group would decrease their drinking compared with the control group. Third, the intervention was not expected to directly affect implicit alcohol-related cognitions; we rather expected that a reduction in drinking would be achieved through a moderating effect of an increased motivation to change (Stacy et al., 2004; Wiers et al., 2007).
Method
Participants
Recruited from five low-level vocational schools, a total of 125 Dutch adolescents (51 male and 74 female) in the age range of 15 to 23 (mean age = 17.07, SD = 1.64) were included at pretest and randomly assigned to the experimental intervention group (n = 61) and information-only control group (n = 64). Out of the total sample, 80 participants (64 %) indicated having one or more binge-drinking episodes (five or more Dutch standard alcoholic drinks on one occasion) in the last month.
Material
Alcohol use
Alcohol use was assessed with a Dutch version of the alcohol use questionnaires as described in Ames et al. (2007).
Alcohol-related problems
An index of alcohol-related problems was assessed using an 18-item version of the Rutgers Alcohol Problems Index (RAPI; White & Labouvie, 1989; Cronbach’s α =.79).
Implicit Association Test (IAT)
In the IAT, participants categorize four categories of stimuli as quickly as possible while only using a left or right response key (see Greenwald, McGhee, & Schwartz, 1998). In this study, three adapted versions of the original IAT were used in which both stimulus pictures and words were used. One IAT assessed the association between “active” positive arousal words versus “neutral” words with photos of objects related to alcohol or objects related to soft drinks. Another IAT assessed the association between “relaxed” positive sedation words versus neutral words with alcohol related objects or soft drink-related objects. Last, one IAT assessed the association between “miserable” negative words versus neutral words with words with alcohol related objects or soft drink-related objects. These attribute categories were chosen because they represent the three main categories of alcohol expectancies (Goldman & Darkes, 2004). The D-2SD penalty score for practice and test was chosen as the main reaction time measure (Greenwald, Nosek, & Banaji, 2003). The internal consistency between practice and test items was acceptable (Cronbach’s α = .57–.64).
Expectancy Questionnaire
The direct measure of alcohol-related cognitions included 18 items representing an explicit version of the IAT attribute words (as in Wiers, van Woerden, Smulders, & De Jong, 2002). The questionnaire consisted of three scales: a positive-arousal, a positive-sedation and a negative outcome scale (Cronbach’s alphas ranging from .70 to .87). Note that positive sedation is not equivalent to negative reinforcement, which is related to problem drinking (Wiers, 2008).
Readiness to change
Readiness to change was measured with a ruler specifically designed for this purpose (LaBrie, Quinlan, Schiffman, & Earleywine, 2005). The anchors for the 10-point readiness-to-change ruler were “I never think about my alcohol/drug use” and “My alcohol/drug use has changed. I now drink/use drugs less.”
Procedure
Pretest
After obtaining active consent from the participants (and if the participant was a minor also the parents), participants were tested in groups of four at school in a separate test room during school time. The IATs were administered first on a laptop with a separate response device in counterbalanced order. Next, the participants filled out the expectancy questionnaire. The alcohol use and alcohol-related problems questionnaires and readiness-to-change ruler were administered last. The total assessment took approximately 45 minutes for each participant. Directly after, participants were randomly assigned to the intervention or control group.
Intervention
The intervention consisted of an MI in which normative feedback on adolescent substance use was provided. During an MI session, various counseling skills are used (e.g., reflective listening and affirmations) to elicit “change talk” (Miller & Rollnick, 2002). The main objective is to stimulate new thinking on one’s personal substance use, which could then result in behavior change. The interviews were conducted by psychology graduate students trained in MI and in utilizing the written protocol (see Grenard et al., 2007). The interview was conducted in approximately 30 minutes. Last, the participant received five information flyers about the biological and cognitive effects of various substances. On the backside of the flyers, the address of the appropriate community health center and several drug information Web sites and telephone lines were listed. Additional details on the conducted MIs are available from the first author upon request.
Information-only control group
After filling out the pretest, participants in the control group received the same five information flyers as the participants in the experimental group did.
Posttest and follow-up
One month later, the participants followed the same assessment procedure as was followed at pretest. Of the 125 participants, 113 participants (90.40%) were present at posttest. Approximately six months after the intervention, of the 103 participants that could be contacted again by mail, 74 participants (71.8 %) returned completed questionnaires on alcohol use, alcohol-related problems, and motivation to change.
Data Reduction
To obtain a normally distributed dependent variable and to reduce the chances of a Type I error by multiple testing, we computed a log transformed standardized alcohol use index score out of six different correlated alcohol use outcome measures (for details on this procedure, see Thush, Wiers, Ames et al., 2007, 2008; Cronbach’s α = .85).
Results
Drop Out and Outliers
Of the 61 participants included in the experimental group, only 6 participants did not discuss alcohol use to a great extent.1 Of the 12 participants who dropped out at posttest, 5 participants belonged to the control group and 7 participants belonged to the experimental group, χ2(1) = 0.48, p = .49. At follow-up, participants and those who dropped out only differed significantly in their baseline alcohol use; those who dropped out had a lower alcohol use than the participants. Analyses included only those participants reporting that they had consumed alcohol in their lifetime: 15 participants reported that they had never consumed alcohol and were therefore eliminated from all further analyses. In addition, the scores on the IAT of 7 participants who exceeded the mean error scores by more than 3 SDs were excluded from further analyses that concerned that specific IAT (see Greenwald et al., 2003). Thus, the final analytical sample at pretest consisted of 110 participants (experimental group = 55; control group = 55), at posttest of 100 participants (experimental group = 50, control group = 50) and at follow-up of 70 participants (experimental group = 36, control group = 34).
Quality of the Intervention
To assess the quality of the conducted interviews, 20% of all taped interviews were rated by using the Motivational Interview Treatment Integrity Code (MITI; Moyers, Martin, Manuel, Hendrickson, & Miller, 2005). In general, there were no signs that the intervention was not performed according to MI standards or protocol; on average, the quality of the interviews was good (Table 1). Detailed data on the quality of the MIs are available from the first author upon request.
Table 1.
Means and SDs on the Motivational Interview (MI) Treatment Integrity Code (N = 11)
| M | SD | |
|---|---|---|
| Empathy | 5.55 | 0.69 |
| Spirit | 5.00 | 0.63 |
| Information | 2.33 | 1.41 |
| MI true | 3.00 | 1.55 |
| MI untrue | 0.30 | 0.48 |
| Closed questions | 24.09 | 5.43 |
| Open questions | 12.85 | 5.06 |
| Simple reflections | 4.36 | 1.69 |
| Complex reflections | 1.27 | 1.49 |
Note. During 20 minutes of each interview, the following variables were rated. Empathy = extent to which the interviewer understood the participants perspective rated on a seven-point Likert scale ranging from low to high; Spirit = extent to which the interviewer showed MI adherence on a seven-point Likert scale ranging from low to high; Information = total number of times information was given; MI true = total number of times interviewer acted according to MI standards; MI untrue = total number of times interviewer acted not according to MI standards; Closed questions = number of closed-ended questions; Open questions = number of open-ended questions; Simple reflections = number of reflections that expressed understanding or a paraphrase of the participants words; Complex reflections = number of reflections that expressed a deeper value of the participants words.
Short-term Effects of the Intervention
Implicit associations
A 2 (Time) × 2 (Condition) mixed analysis of covariance (ANCOVA) controlling for age and gender revealed a borderline significant Time × Condition effect for the implicit positive arousal associations with alcohol, F(1, 89) = 3.42, p = .07. However, both the decrease in implicit positive arousal associations between pretest and posttest in the experimental group and the increase in implicit positive arousal associations with alcohol between pretest and posttest in the control group were not significant, respectively, t(44) = −1.22, p = .23, and t(47) = 1.47, p = .15.
Alcohol outcome expectancies
A 2 (Time) × 2 (Condition) mixed analysis of covariance controlling for age and gender revealed a borderline significant Time × Condition effect for the explicit positive sedation alcohol expectancies, F(1, 92) = 3.78, p = .055. However, the increase in explicit positive sedation alcohol expectancies between pretest and posttest in the experimental group was not significant, t(46) = 1.02, p = .32, nor was the decrease in explicit positive sedation alcohol expectancies between pretest and posttest control group t(48) = −1.56, p = .13. Contrary to our hypothesis, there was no significant Time × Condition effect for the explicit negative alcohol expectancies, F(1, 92) = 1.86, p = .176.
Readiness to change
A 2 (Time) × 2 (Condition) mixed ANCOVA controlling for age and gender did not reveal a significant Time × Condition effect for the readiness to change score, F(1, 85) = 0.01, p > .50.
Alcohol use
A 2 (Time) × 2 (Condition) mixed ANCOVA controlling for age and gender did not reveal a significant Time × Condition effect for the alcohol use index, F(1, 93) = 0.12, p > .50. Given that there was no significant change in the alcohol use index, we did not perform the additional analyses to investigate the possible moderation of motivation on the influence of implicit alcohol associations on subsequent drinking behavior.
Long-term Effect of the Intervention
We analyzed the long-term effects of the intervention by constructing a Latent Growth Model (LGM; Meredith & Tisak, 1990) by using AMOS 7.0 (Arbuckle, 2006). Based on the delta χ2 test, we decided that the model represented in Figure 1 fits the data relatively well compared with more elaborate models, such as a model with a quadratic effect of time. This model was accepted as fitting the data (χ2(6) = 3.687, p = .719, RMSEA = .000, CFI = 1.000, TLI = 1.028). The regression weights in Table 2 show that there was a nonsignificant effect of condition on intercept (B = 0.124, p = .291) and on slope (B = 0.001, p = .884). This means that the two treatment conditions did not significantly differ with respect to baseline value and change of the alcohol use index over time. That is, there was no effect of condition on baseline functioning, and no interaction between time and condition. The main effect of time was also non-significant (B = −0.004, p = .159). The initial level of alcohol use index was significantly different from zero (B = −0.174, p = .036).
Figure 1.
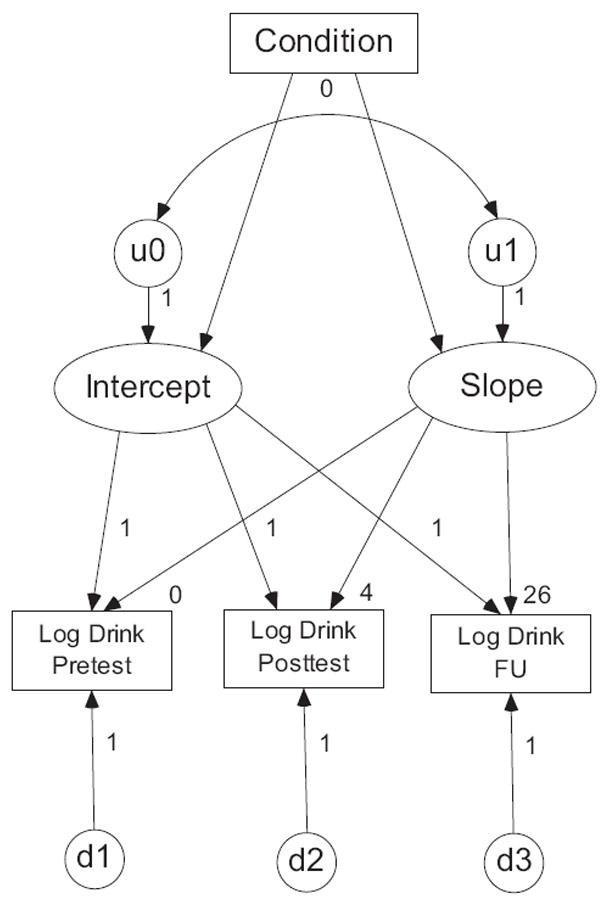
Latent growth model for the log alcohol use index. Condition = control or experimental group; Intercept = baseline log alcohol use index; Slope = change log alcohol use index; Log Drink Pretest = log alcohol use index score at pretest; Log Drink Posttest = log alcohol use index score at posttest; Log Drink FU = log alcohol use index score at six month follow up. The labels mark path coefficients that were constrained across assessment points. By fixing all paths from the intercept factor to each measurement point to 1 and all paths from the slope factor to each measurement point to 0, 4, 26 (representing the number of weeks between time points), this model represents linear growth. The path from condition to intercept tests whether the experimental group differs from the control group in baseline functioning. This is the main effect of condition. The path from condition to slope tests whether individual growth within the experimental group differs from individual growth in the control group. This is the interaction between time and condition we are primarily interested in evaluating. Both the variance U1 and the covariance between U0 and U1 were fixed at 0 to make the model admissible (these values were estimated negative if not fixed). The variances of the latent variables d1–d3 were estimated equal to each other; the model where each variance was estimated individually did not lead to a significant increase in model fit compared with this model.
Table 2.
Summary of the Parameter Estimates in the Latent Growth Model (N = 110)
| Estimate | SE | P | |
|---|---|---|---|
| Regression weights | |||
| Intercept | −.174 | .083 | .036 |
| Slope | −.004 | .003 | .159 |
| Condition × Intercept | .124 | .117 | .291 |
| Condition × Slope | .001 | .004 | .884 |
| Variances | |||
| D1 | .104 | .012 | *** |
| D2 | .104 | .012 | *** |
| D3 | .104 | .012 | *** |
| U0 | .309 | .048 | *** |
| U1 | .000 | ||
| Covariance | |||
| U0 ↔ U1 | .000 |
Note. Condition = control or experimental group; Intercept = baseline log alcohol use index; Slope = change log alcohol use index. Both the variance U1 and the covariance between U0 and U1 were fixed at 0 to make the model admissible, hence that they do not have a standard error or p value.
p < .001.
Discussion
This study investigated the influence of MI on explicit and implicit alcohol-related cognitions and alcohol use in at-risk adolescents. The first hypothesis, that in the experimental group motivation to change and negative expectancies would increase compared with the control group, could not be confirmed. Second, we could not find the hypothesized effect that the experimental group would decrease their drinking compared with the control group. Given these null findings, the moderation hypothesis that a reduction in drinking would be due to increased motivation to change could not be tested.
A possible explanation for the lack of support for an intervention effect on drinking behavior might be that there was no increase in readiness to change in the experimental group. Although it is assumed that MI increases motivation to change (Miller & Rollnick, 2002) and the intervention was according to MI standards, readiness to change was not effected by the intervention. This raises some questions regarding the effectiveness of MI in some (at-risk) adolescent populations. Although MI has been proven to be effective in reducing hazardous drinking in (young) adult populations, this strategy might be less effective in (at-risk) adolescents, which could be explained by the differential response to alcohol in adolescents and (young) adults. During adolescence the positive arousal effects of drinking are being experienced more so than the negative effects (National Institute on Alcohol Abuse and Alcoholism, 2005). Therefore, these adolescents might feel they do not have sufficient reason for changing their drinking behavior (cf., Thush, Wiers, Theunissen, et al., 2007). Consequently, it would be useful for future research to investigate the developmental variation in intervention response in some more detail.
Even though there were no changes in drinking behavior or readiness to change, some borderline significant changes in both implicit and explicit alcohol-related cognitions between pretest and posttest were found. Based on current dual process models, we especially did not hypothesize any changes in implicit cognitive processes, given that these processes are generally quite robust and not easy to change with a short intervention (e.g. Fazio & Towles-Schwen, 1999; Strack & Deutsch, 2004). Furthermore, there is mixed evidence for the malleability of implicit cognitions over the course of treatment although very few studies have examined this question to date (Wiers, Van de Luitgaarden, Van den Wildenberg, & Smulders, 2005; c.f., Huijding & de Jong, 2007; Teachman & Woody, 2003). At this point, the authors cannot provide a plausible explanation for the current results, and further research is needed to investigate the possible influence of interventions on the pretest/posttest assessment of explicit and implicit cognitions.
The present results should be interpreted with some caution, given some limitations. First, although we screened for schools with a high proportion of at-risk adolescents, we did not use a probability sampling strategy at an individual level. In addition, although participants were recruited at five different schools, we did not have the statistical power to adequately perform a multiple group analysis. Therefore, the present results should thus be interpreted with some caution with regard to the generalization to other (at-risk) adolescent populations. Second, there are some limitations regarding the sequence of the measures used in the current study and the measures themselves. Because the IAT, and the alcohol expectancy, alcohol use, and readiness to change questionnaires were performed in a fixed sequence possibly order effects could have played a role in the current results. However, this fixed sequence was chosen as the optimal procedure to minimize method-related variance in a study focusing on individual differences (cf. Asendorpf, Banse, & Mücke, 2002). Finally, it must be noted that not all participants in the experimental group discussed alcohol use to a great extent: 6 participants discussed other lifestyle issues or substance use. Nevertheless, the results did not differ with or without these participants.
Summarizing, although these limitations must be taken into consideration, we believe that this study does provide useful information. Although we did not find that the current MI intervention influenced motivation to change or drinking behavior, MI is assumed to affect readiness to change and this in turn is strongly connected to behavior change (Miller & Rollnick, 2002). Our findings raise some questions regarding the use of a brief MI in this particular at-risk adolescent population and the mechanisms through which MI is effective. Future experimental research regarding the influence of MI on alcohol-related cognitions can possibly shed some light on these issues.
Acknowledgments
This research was supported by grants from the Dutch Health Care Research Organization (ZON-Mw; 31000065) and the National Institute on Drug Abuse (NIDA; DA16094).
Footnotes
Parts of these data were presented at the biennial meeting of the Society for Research on Adolescence in Chicago (March 2008).
Given that the results did not differ for the analytical sample with or without these participants, we decided to include these participants to have more statistical power to conduct the long-term analyses.
Contributor Information
Carolien Thush, Department of Clinical Psychological Science, Maastricht University, Maastricht, the Netherlands.
Reinout W. Wiers, Department of Clinical Psychological Science, Maastricht University, Maastricht, the Netherlands
Mirjam Moerbeek, Department of Methodology and Statistics, Utrecht University, Utrecht, the Netherlands.
Susan L. Ames, Institute for Health Promotion and Disease Prevention Research, University of Southern California
Jerry L. Grenard, Institute for Health Promotion and Disease Prevention Research, University of Southern California
Steve Sussman, Institute for Health Promotion and Disease Prevention Research, University of Southern California.
Alan W. Stacy, Institute for Health Promotion and Disease Prevention Research, University of Southern California
References
- Ames SL, Grenard JL, Thush C, Sussman S, Wiers RW, Stacy AW. Comparison of indirect assessments of marijuana-related associations among at-risk adolescents. Experimental Clinical Psychopharmacology. 2007;15:204–218. doi: 10.1037/1064-1297.15.2.218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arbuckle JL. AMOS 7.0 user’s guide. Chicago: SPSS Press; 2006. [Google Scholar]
- Asendorpf JB, Banse R, Mücke D. Double dissociation between implicit and explicit personality self-concept: The case of shy behavior. Journal of Personality and Social Psychology. 2002;83:380–393. [PubMed] [Google Scholar]
- Bosari B, Carey KB. Effects of a brief motivational intervention with college student drinkers. Journal of Consulting and Clinical Psychology. 2000;68:728–733. [PubMed] [Google Scholar]
- Cox WM, Klinger E. Motivational structure relationships with substance use and processes of change. Addictive Behaviors. 2002;27:925–940. doi: 10.1016/s0306-4603(02)00290-3. [DOI] [PubMed] [Google Scholar]
- Fazio RH, Towles-Schwen T. The MODE model of attitude-behavior processes. In: Chaiken S, Trope Y, editors. Dual process theories in social psychology. New York: Guilford Press; 1999. pp. 97–116. [Google Scholar]
- Goldman MS, Darkes J. Alcohol expectancy multiaxial assessment: A memory network-based approach. Psychological Assessment. 2004;16:4–15. doi: 10.1037/1040-3590.16.1.4. [DOI] [PubMed] [Google Scholar]
- Greenwald AG, Banaji MR. Implicit social cognition: Attitudes, self-esteem, and stereotypes. Psychological Review. 1995;102:4–27. doi: 10.1037/0033-295x.102.1.4. [DOI] [PubMed] [Google Scholar]
- Greenwald AG, McGhee DE, Schwartz JLK. Measuring individual differences in implicit cognition: The Implicit Association Test. Journal of Personality and Social Psychology. 1998;74:1464–1480. doi: 10.1037//0022-3514.74.6.1464. [DOI] [PubMed] [Google Scholar]
- Greenwald AG, Nosek BA, Banaji MR. Understanding and using the Implicit Association Test: 1. An improved scoring algorithm. Journal of Personality and Social Psychology. 2003;85:197–216. doi: 10.1037/0022-3514.85.2.197. [DOI] [PubMed] [Google Scholar]
- Grenard JL, Ames SL, Pentz MA, Sussman S. Motivational interviewing with adolescents and young adults for drug-related problems. International Journal of Adolescent Medical Health. 2006;18:53–67. doi: 10.1515/ijamh.2006.18.1.53. [DOI] [PubMed] [Google Scholar]
- Grenard JL, Ames SL, Wiers RW, Thush C, Stacy AW, Sussman S. Brief intervention for substance use among at-risk adolescents: An initial study. Journal of Adolescent Health. 2007;40:188–191. doi: 10.1016/j.jadohealth.2006.08.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grenard JL, Ames SL, Wiers RW, Thush C, Sussman S, Stacy AW. Working memory moderates the predictive effects of drug-related associations on substance use. Psychology of Addictive Behaviors. 2008;22:426–432. doi: 10.1037/0893-164X.22.3.426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Huijding J, de Jong P. Beyond fear and disgust: The role of (automatic) contamination-related associations in spider phobia. Journal of Behavior Therapy and Experimental Psychiatry. 2007;38:200–211. doi: 10.1016/j.jbtep.2006.10.009. [DOI] [PubMed] [Google Scholar]
- Jones BT, Corbin W, Fromme K. A review of expectancy theory and alcohol consumption. Addiction. 2001;91:57–72. doi: 10.1046/j.1360-0443.2001.961575.x. [DOI] [PubMed] [Google Scholar]
- Jones BT, McMahon J. Alcohol motivations as outcome expectancies. In: Miller WR, Heather N, editors. Treating addictive behaviors Applied clinical psychology. 2. New York: Plenum Press; 1998. pp. 75–91. [Google Scholar]
- LaBrie JW, Quinlan T, Schiffman JE, Earleywine ME. Performance of alcohol and safer sex change rulers compared with readiness to change questionnaires. Psychology of Addictive Behaviors. 2005;19:112–115. doi: 10.1037/0893-164X.19.1.112. [DOI] [PubMed] [Google Scholar]
- Larimer ME, Cronce JM. Identification, prevention and treatment: A review of individual-focused strategies to reduce problematic alcohol consumption by college students. Journal of Studies on Alcohol. 2002;14(Suppl 1):148–63. doi: 10.15288/jsas.2002.s14.148. [DOI] [PubMed] [Google Scholar]
- Larimer ME, Cronce JM. Identification, prevention and treatment revisited: Individual-focused college drinking prevention strategies 1999–2006. Addictive Behaviors. 2007;32:2439–2468. doi: 10.1016/j.addbeh.2007.05.006. [DOI] [PubMed] [Google Scholar]
- Marlatt GA, Baer JS, Kivlahan DR, Dimeff LA, Larimer ME, Quigley LA, et al. Screening and brief intervention for high-risk college student drinkers: Results from a 2-year follow-up assessment. Journal of Consulting and Clinical Psychology. 1998;66:604–615. doi: 10.1037//0022-006x.66.4.604. [DOI] [PubMed] [Google Scholar]
- McCambridge J, Strang J. The efficacy of single-session motivational interviewing in reducing drug consumption and perceptions of drug-related risk and harm among young people: Results from a multi-site cluster randomized trial. Addiction. 2004;99:39–52. doi: 10.1111/j.1360-0443.2004.00564.x. [DOI] [PubMed] [Google Scholar]
- Meredith W, Tisak J. Latent curve analysis. Psychometrika. 1990;55:107–122. [Google Scholar]
- Miller WR, Rollnick S. Motivational interviewing: Preparing people to change addictive behaviors. 2. New York: Guilford; 2002. [Google Scholar]
- Moyer A, Finney J, Swearingen C, Vergun P. Brief interventions for alcohol problems: A meta-analytic review of controlled investigations in treatment-seeking and non-treatment-seeking populations. Addiction. 2002;97:279–92. doi: 10.1046/j.1360-0443.2002.00018.x. [DOI] [PubMed] [Google Scholar]
- Moyers TB, Martin T, Manuel JK, Hendrickson SML, Miller WR. Assessing competence in the use of motivational interviewing. Journal of Substance Abuse Treatment. 2005;28:19–26. doi: 10.1016/j.jsat.2004.11.001. [DOI] [PubMed] [Google Scholar]
- National Institute on Alcohol Abuse and Alcoholism (NIAAA) The effects of alcohol on physiological processes and biological development. Alcohol Research and Health. 2005;28:125–31. [PMC free article] [PubMed] [Google Scholar]
- Olson MA, Fazio RH. Trait interferences as a function of automatically activated racial attitudes and motivation to control prejudiced reactions. Basic Applied Social Psychology. 2004;26:1–11. [Google Scholar]
- Stacy AW. Memory activation and expectancy as prospective predictors of alcohol and marijuana use. Journal of Abnormal Psychology. 1997;106:61–73. doi: 10.1037//0021-843x.106.1.61. [DOI] [PubMed] [Google Scholar]
- Stacy AW, Ames SL, Knowlton BJ. Neurologically plausible distinctions in cognition relevant to drug use etiology and prevention. Substance Use and Misuse. 2004;39:1571–1623. doi: 10.1081/ja-200033204. [DOI] [PubMed] [Google Scholar]
- Strack F, Deutsch R. Reflective and impulsive determinants of social behavior. Personality and Social Psychology Review. 2004;8:220–247. doi: 10.1207/s15327957pspr0803_1. [DOI] [PubMed] [Google Scholar]
- Teachman BA, Woody SR. Automatic processing in spider phobia: Implicit fear association over the course of treatment. Journal of Abnormal Psychology. 2003;112:100–109. [PubMed] [Google Scholar]
- Thush C, Wiers RW. Explicit and implicit alcohol-related cognitions and the prediction of future drinking in adolescents. Addictive Behaviors. 2007;32:1367–1383. doi: 10.1016/j.addbeh.2006.09.011. [DOI] [PubMed] [Google Scholar]
- Thush C, Wiers RW, Ames SL, Grenard JL, Sussman S, Stacy AW. Apples and oranges? Comparing indirect measures of alcohol-related cognition predicting alcohol use in at-risk adolescents. Psychology of Addictive Behaviors. 2007;21:587–591. doi: 10.1037/0893-164X.21.4.587. [DOI] [PubMed] [Google Scholar]
- Thush C, Wiers RW, Ames SL, Grenard JL, Sussman S, Stacy AW. Interactions between implicit cognition and working memory in the prediction of alcohol use in at-risk adolescents. Drug and Alcohol Dependence. 2008;94:116–124. doi: 10.1016/j.drugalcdep.2007.10.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thush C, Wiers RW, Theunissen N, Van den Bosch J, Opdenacker J, van Empelen P, et al. A randomized clinical trial of a targeted intervention to moderate alcohol use and alcohol-related problems in at-risk adolescents. Pharmacology Biochemistry and Behavior. 2007;86:368–376. doi: 10.1016/j.pbb.2006.07.023. [DOI] [PubMed] [Google Scholar]
- White HR, Labouvie EW. Towards the assessment of adolescent problem drinking. Journal of Studies on Alcohol. 1989;50:30–37. doi: 10.15288/jsa.1989.50.30. [DOI] [PubMed] [Google Scholar]
- Wiers RW. Alcohol and drug expectancies as anticipated changes in affect: Negative reinforcement is not sedation. Substance Use and Misuse. 2008;43:501–516. doi: 10.1080/10826080701203021. [DOI] [PubMed] [Google Scholar]
- Wiers RW, Bartholow BD, van den Wildenberg E, Thush C, Engels R, Sher K, et al. Automatic and controlled processes and the development of addictive behaviors in adolescents: A review and a model. Pharmacology, Biochemistry and Behavior. 2007;86:263–283. doi: 10.1016/j.pbb.2006.09.021. [DOI] [PubMed] [Google Scholar]
- Wiers RW, Van de Luitgaarden J, Van den Wildenberg E, Smulders FTY. Challenging implicit and explicit alcohol-related cognitions in young heavy drinkers. Addiction. 2005;100:806–819. doi: 10.1111/j.1360-0443.2005.01064.x. [DOI] [PubMed] [Google Scholar]
- Wiers RW, van Woerden N, Smulders FTY, De Jong PJ. Implicit and explicit alcohol-related cognitions in heavy and light drinkers. Journal of Abnormal Psychology. 2002;111:648–658. doi: 10.1037/0021-843X.111.4.648. [DOI] [PubMed] [Google Scholar]
- Wood M, Capone C, Laforge R, Erickson DJ, Brand NH. Brief motivational interview and alcohol expectancy challenge with heavy drinking college students: A randomized factorial study. Addictive Behaviors. 2007;32:2509–2528. doi: 10.1016/j.addbeh.2007.06.018. [DOI] [PubMed] [Google Scholar]