

Abstract
Objective
To estimate the effect of birth-weight difference between the current and index pregnancy on VBAC failure in patients whose prior cesarean was for cephalopelvic disproportion (CPD).
Methods
This was a retrospective cohort study of women with one cesarean for CPD, comparing the rate of VBAC failure in women whose infant was smaller, the same, or larger in the VBAC attempt compared to cesarean. The primary outcome was VBAC attempt failure, defined as a patient that attempted VBAC but subsequently required a cesarean for any indication. Univariable, stratified, and multivariable analyses were used.
Results
Of 13,706 patients attempting VBAC, 1,511 had one prior cesarean for CPD. Compared to patients with the same birth weight, a lower birth weight had fewer failed VBAC attempts (adjusted odds ratio (29.6% vs 37.8%, AOR) 0.7, 95% confidence interval (CI) 0.5-1.0) and a higher birth weight had more failed VBAC attempts (54.5% vs 37.8%, AOR 2.0, 95% CI 1.5-2.8).
Conclusions
Birth-weight difference has a moderate effect on the rate of VBAC success in patients whose prior cesarean was for CPD.
Introduction
The indication for prior cesarean has an impact on the success of a subsequent attempt at vaginal birth. Although a cesarean for non-recurring indications, such as malpresentation, is associated with relatively high success rates (80%) in vaginal birth after cesarean (VBAC) attempts, success rates fall when the prior cesarean was for a recurring indication, such as cephalopevic disproportion (CPD) or failed induction.(1) In these cases, patients may rightfully ask what the likelihood of a successful VBAC is if the current baby is bigger or smaller than the baby for whom the cesarean was performed; they may also request that repeat ultrasounds be performed in order to determine the difference in weight between this pregnancy and the prior. The majority of prior publications in this area have focused on the absolute birth weight of the infant in the VBAC attempt and the probability of a successful VBAC.(2-4) However, limited clinical research is available to inform the patient or clinician on the impact of fetal size in this pregnancy compared to the prior birth in the decision of delivery mode.
In this study, we attempt to estimate the effect of birth weight difference between the current and index pregnancy on VBAC failure in patients whose prior cesarean was for cephalopelvic disproportion.
Methods
This was a secondary analysis of a retrospective, multicenter cohort study of women with a prior cesarean delivery.(5) Seventeen tertiary and community hospitals, all with institutional review board approval, participated in a study designed to estimate the rate of and risk factors for uterine rupture in VBAC attempts. The study was conducted from 1995-2000. Methods of the study have been published in detail previously, but a brief description follows.(5)
Subjects were identified at each site using International Classification of Disease, 9th Revision (ICD-9) codes for “previous cesarean delivery, delivered;” trained research nurses used standardized, closed-end data collection forms to extract data from medical charts. Three percent of charts were re-extracted for quality control. Data collected included: maternal demographics, medical and obstetric history, social history, family history, details of the index pregnancy, antepartum course, labor and delivery events, complications, and maternal outcomes.
For the primary analysis, women with one prior cesarean delivery for CPD who attempted VBAC were divided into three groups: birth weight in the VBAC attempt was the same as in the prior cesarean delivery (within 100-g), birth weight in the VBAC attempt was more than 100-g smaller than in the cesarean delivery, or birth weight in the VBAC attempt was more than 100-g larger than in the cesarean delivery. One hundred grams was chosen as a prior study demonstrated a decrease in the odds of successful VBAC for every 100-g increase in birth weight difference.(6) The primary outcome evaluated was VBAC attempt failure, defined as a patient that attempted VBAC but subsequently required a cesarean for any indication. Receiver operating characteristics (ROC) curves were generated to evaluate the utility of birth weight difference to predict VBAC failure. Secondary analyses were performed using an exposure of birth weight in the VBAC attempt of 250-g and 500-g greater or less than the cesarean delivery birth weight.
Women were excluded if they had a prior classical cesarean or more than one prior cesarean. As we were primarily interested in viable pregnancies, women were excluded from the analysis if the VBAC birth weight was documented as less than 500g. A documented birth weight of less than 500g for the cesarean was excluded as this was likely to represent a classical cesarean.
Because cephalopelvic disproportion can be difficult to diagnose,(7) a secondary analysis of this data set was performed, including women whose diagnoses could have included CPD. These indications were failed induction and non-reassuring fetal status. A failed induction may actually represent CPD, for example in the case of a macrosomic fetus that fails to descend into the pelvis. A prior cesarean for non-reassuring fetal status may represent a patient with a protracted labor curve and an NICHD category two tracing,(8) where the physician suspected CPD. Because it is difficult to clarify these subtleties from a retrospective study, we elected to include these indications in secondary analyses.
Secondary outcomes examined include uterine rupture, blood transfusions, postpartum fever, and a composite of complications that included uterine rupture, bladder injury, uterine artery laceration, and bowel injury. Definitions of each outcome may be found in prior publications.(5)
The exposure and comparison groups were compared with descriptive and univariable statistics using ANOVA for continuous variables and χ2 or Fisher’s exact tests for categorical variables. Potentially confounding variables of the exposure-outcome association were identified in the stratified analyses. Multivariable logistic regression models for the primary outcome were then developed to estimate the effect of change in birth weight between the current and index pregnancy on VBAC failure. Covariates for initial inclusion in multivariable statistical models were selected using results of the univariable and stratified analyses and based on historical known confounding factors for VBAC success (prior vaginal delivery, diabetes, and spontaneous labor).(1, 9) Factors were removed in a backward step-wise fashion, based on significant changes (10%) in the exposure adjusted odds ratio or significant differences between hierarchical models using the likelihood ratio test. The statistical analysis was performed using STATA, version 10 Special Edition (College Station, TX).
Results
The initial chart review identified 25,076 patients with the ICD-9 code “previous cesarean delivery, delivered,” 13,706 of whom attempted VBAC. Birth weight data for both the index and current pregnancy were available in 91.0% of these patients. Of these, 1,511 had one prior cesarean for CPD. An additional 1,175 had one prior cesarean for failed induction and 1,292 had one prior cesarean for non-reassuring fetal status. Patients in the three exposure groups (smaller birth weight, same birth weight, and larger birth weight) were similar with respect to age, gravidity, race, presence of a hypertensive disorder, spontaneous labor, and oxytocin use (Table 1). Women in the same birth weight category were slightly more likely to deliver at a university hospital and to have their labor augmented and were less likely to have a prior vaginal delivery, have diabetes, or be induced.
Table 1.
Characteristics of Patients by Birth Weight Difference
| Lower Birth Weight (n = 1756) |
Same Birth Weight† (n = 575) |
Higher Birth Weight (n = 1644) |
p | |
|---|---|---|---|---|
| Maternal age (yrs) | 30.1 ± 5.5 | 29.9 ± 5.6 | 29.8 ± 5.6 | 0.24 |
| Gravidity | 3.2 ± 1.4 | 3.0 ± 1.4 | 3.2 ± 1.5 | 0.20 |
| University Hospital (%) | 911 (51.9) |
262 (45.5) |
850 (51.7) |
0.02 |
| Prior vaginal delivery (%) | 476 (27.1) |
127 (22.0) |
444 (27.0) |
0.04 |
| African American Race (%) | 545 (31.0) |
178 (30.9) |
557 (33.9) |
0.16 |
| Labor Type | ||||
| Spontaneous (%) | 773 (44.0) |
257 (44.6) |
757 (46.0) |
0.49 |
| Augmented (%) | 352 (20.0) |
141 (24.5) |
355 (21.6) |
0.07 |
| Induced (%) | 632 (36.0) |
178 (30.9) |
533 (32.4) |
0.03 |
| Oxytocin Use (%) | 783 (44.6) |
269 (46.7) |
719 (43.7) |
0.46 |
| Medical Problems | ||||
| Diabetes (%) | 115 (6.6) |
11 (1.9) |
98 (6.0) |
<0.01 |
| Any Hypertension* (%) | 96 (5.5) |
26 (4.5) |
84 (5.1) |
0.66 |
| Indication for Prior Cesarean | <0.01 | |||
| Cephalopelvic disproportion (%) |
802 (45.7) |
225 (39.1) |
484 (29.4) |
|
| Failed induction (%) | 525 (29.9) |
183 (31.8) |
467 (28.4) |
|
| Nonreassuring Fetal Status (%) | 430 (24.5) |
168 (29.2) |
694 (42.2) |
Includes chronic hypertension, gestational hypertension, and preeclampsia
Same birthweight = within 100 grams of previous birthweight
In women attempting VBAC whose prior cesarean was for CPD, 586 (38.9%) had a failed VBAC attempt. When grouped according to lower birth weight, same birth weight, or higher birth weight in the VBAC attempt compared to the cesarean, a modest effect of birth weight difference on VBAC failure rate is seen (Table 2). Compared to patients in the same birth weight category, women whose infant was a lower birth weight had a moderately lower rate of failed VBAC (29.6% vs 37.8%, adjusted odds ratio (AOR) 0.7, 95% confidence interval (CI) 0.5-1.0). The higher birth weight category had a moderately higher rate of failed VBAC compared to the same birth weight (54.5% vs 37.8%, AOR 2.0, 95% CI 1.5-2.8).
Table 2.
Risk of Failed VBAC in patients with a Prior Cesarean for CPD
| Lower Birth Weight |
RR (95% CI) |
Adjusted OR (95% CI) |
Same Birth Weight (Reference) |
Higher Birth Weight |
RR (95% CI) |
Adjusted OR (95% CI) |
||
|---|---|---|---|---|---|---|---|---|
| n = 802 | n = 225 | n = 484 | ||||||
|
Prior
Cesarean for CPD Only (n=1515) |
Failed VBAC (%) | 237 (29.6) |
0.8 (0.6-1.0) |
0.7† (0.5-1.0) |
85 (37.8) |
264 (54.5) |
1.4 (1.2-1.7) |
2.0† (1.5-2.8) |
| Uterine Rupture (%) |
8 (1.0) |
0.4 (0.2-1.4) |
- | 5 (2.2) |
11 (2.2) |
1.0 (0.4-2.9) |
- | |
| Blood transfusion (%) |
4 (0.5) |
- | - | 0 | 5 (1.0) |
- | - | |
| Post-partum fever (%) |
80 (10.0) |
0.6 (0.4-0.8) |
0.5‡ (0.3-0.8) |
39 (17.3) |
66 (13.6) |
0.8 (0.5-1.1) |
0.7‡ (0.5-1.2) |
|
| Composite Complications* (%) |
19 (2.4) |
0.7 (0.3-1.5) |
0.7§ (0.3-1.6) |
8 (3.5) |
22 (4.5) |
1.3 (0.6-2.8) |
1.3§ (0.6-3.0) |
|
Includes uterine rupture, bladder injury, uterine artery laceration, and bowel injury
Adjusted for prior vaginal delivery, labor induction, and black race
Adjusted for prior vaginal delivery and black race
Adjusted for prior vaginal delivery
Unable to perform calculation either due to small number of cases or reference group of 0
Birth weight was used as a continuous variable to predict the failure of VBAC. Figure 1 displays the generated ROC curve for birth weight difference used to predict failed VBAC; the area under the curve is 0.68.
Figure 1.
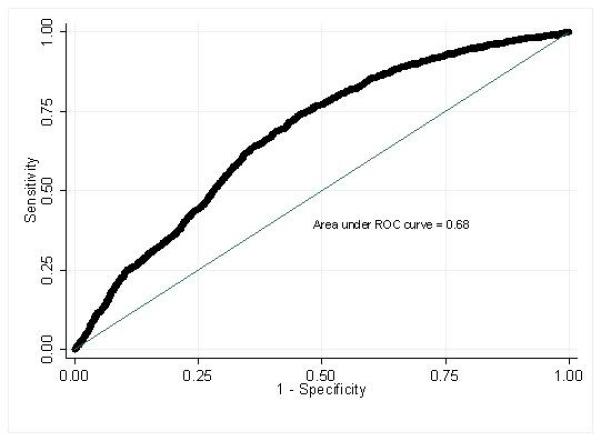
displays the generated ROC curve for birth weight difference used to predict failed VBAC; the area under the curve is 0.68.
The risk of uterine rupture, composite complications, and blood transfusion was not significantly different when lower or higher birth weight was compared to the same birth weight group. The risk of postpartum fever was lower in the lower birth weight group compared to the same birth weight group (10.0% vs 17.3%, AOR 0.5, 95% CI 0.3-0.8). The risk of postpartum fever was similar between the higher and same birth weight categories (13.6% vs 17.3%, AOR 0.8, 95% CI 0.5-1.1).
A similar pattern was seen when patients were included whose prior cesarean was performed for failed induction (Table 3). Again, patients with a lower birth weight in their VBAC attempt compared to their cesarean had a 30% lower rate of failed VBAC, while patients with a higher birth weight had a 40% higher rate of failed VBAC. Patients in the lower birth weight group had a 50% lower rate of composite complications and a 40% lower rate of postpartum fever compared to the same birth weight group; the risk of uterine rupture and blood transfusion was similar. The risk of complications in the higher birth weight group was similar to the same birth weight group.
Table 3.
Risk of Failed VBAC in patients with a Prior Cesarean for CPD or Failed Induction
| Lower Birth Weight n = 1327 |
RR (95% CI) |
Adjusted OR (95% CI) |
Same Birth Weight (Reference) n = 408 |
Higher Birth Weight n = 951 |
RR (95% CI) |
Adjusted OR (95% CI) |
||
|---|---|---|---|---|---|---|---|---|
|
Prior
Cesarean for CPD or Failed Induction (n=2691) |
Failed VBAC (%) | 417 (31.4) |
0.8 (0.7-0.9) |
0.7† (0.5-0.8) |
168 (41.2) |
479 (50.4) |
1.2 (1.1-1.4) |
1.4† (1.2-1.9) |
| Uterine Rupture (%) |
10 (0.8) |
0.4 (0.2-1.1) |
- | 7 (1.7) |
15 (1.6) |
0.9 (0.4-2.2) |
- | |
| Blood transfusion (%) |
8 (0.6) |
0.8 (0.2-3.1) |
- | 3 (0.7) |
11 (1.2) |
1.6 (0.4-5.6) |
- | |
| Post-partum fever (%) |
143 (10.8) |
0.6 (0.5-0.8) |
0.6‡ (0.4-0.8) |
71 (17.4) |
133 (14.0) |
0.8 (0.6-1.0) |
0.8‡ (0.6-1.1) |
|
| Composite Complications* (%) |
30 (2.3) |
0.5 (0.3-0.9) |
0.5§ (0.3-0.9) |
18 (4.4) |
42 (4.4) |
1.0 (0.6-1.7) |
1.0§ (0.6-1.8) |
Includes uterine rupture, bladder injury, uterine artery laceration, and bowel injury
Adjusted for prior vaginal delivery, labor induction, and black race
Adjusted for prior vaginal delivery and black race
Adjusted for prior vaginal delivery
Unable to perform calculation either due to small number of cases or reference group of 0
When including patients whose prior cesarean was for CPD, failed induction or nonreassuring fetal status, the risk of failed VBAC was moderately lower in patients whose infant was smaller compared to women whose infants were the same size (Table 4). The risk of failed VBAC attempt was slightly increased in patients in the higher birth weight category compared to same birth weight (42.1% vs 38.7%, AOR 1.2, 95% CI 1.0-1.5). Patients in the lower birth weight group had a 40% lower rate of postpartum fever but were similar to the same birth weight group with respect to uterine rupture, blood transfusion, and composite complications. The risk of complications in the higher birth weight group was similar to the same birth weight.
Table 4.
Risk of Failed VBAC in patients with a Prior Cesarean for CPD, Failed Induction, or NRFS
| Lower Birth Weight n = 1757 |
RR (95% CI) |
Adjusted OR (95% CI) |
Same Birth Weight (Reference) n = 576 |
Higher Birth Weight n = 1645 |
RR (95% CI) |
Adjusted OR (95% CI) |
||
|---|---|---|---|---|---|---|---|---|
|
Prior
Cesarean for CPD, Failed Induction, or NRFS (n=3984) |
Failed VBAC (%) | 534 (30.4) |
0.8 (0.7-0.9) |
0.7† (0.6-0.8) |
223 (38.7) |
693 (42.1) |
1.1 (1.0-1.2) |
1.2† (1.0-1.5) |
| Uterine Rupture (%) |
19 (1.1) |
0.9 (0.4-2.1) |
- | 7 (1.2) |
19 (1.1) |
1.0 (0.4-2.3) |
- | |
| Blood transfusion (%) |
11 (0.6) |
1.2 (0.3-4.3) |
- | 3 (0.5) |
15 (0.9) |
1.8 (0.5-6.0) |
- | |
| Post-partum fever (%) |
180 (10.2) |
0.7 (0.5-0.8) |
0.6‡ (0.5-0.8) |
88 (15.3) |
210 (12.8) |
0.8 (0.7-1.1) |
0.8‡ (0.6-1.1) |
|
| Composite Complications* (%) |
46 (2.6) |
0.7 (0.4-1.2) |
0.7§ (0.4-1.2) |
21 (3.6) |
56 (3.4) |
0.9 (0.6-1.5) |
1.0§ (0.6-1.6) |
Includes uterine rupture, bladder injury, uterine artery laceration, and bowel injury
Adjusted for prior vaginal delivery, black race and labor induction
Adjusted for prior vaginal delivery and black race
Adjusted for prior vaginal delivery
Unable to perform calculation either due to small number of cases or reference group of 0
Similar results were obtained when using an exposure based on birth weight differences of 250-g and 500-g. A modest decrease in failed VBAC attempts were seen for the smaller birth weight group (AOR 0.5, 95% CI 0.4-0.6 for 250-g, AOR 0.5, 95% CI 0.4-0.7) and a modest increase in failed VBAC attempts was seen in the larger birth weight group (AOR 1.3, 95% CI 1.1-1.4 for 250-g, AOR 1.4, 95% CI 1.2-1.6 for 500-g) in subjects with a prior cesarean for CPD. (Data not shown, available upon request.)
In patients whose prior cesarean was for CPD, the effect of incremental increases in birth weight was examined (Table 5). A distinct pattern of increased risk of VBAC failure as birth weight gradually increased was not seen. Thus, these data do not support the presence of a dose-response relationship between birth weight difference and failed VBAC attempt.
Table 5.
Risk of Failed VBAC for Patients by Incremental Increases in Birth Weight Difference
| Failed VBAC (n, %) |
RR (95% CI) |
AOR (95% CI) |
|
|---|---|---|---|
| 0-100g (n = 119) |
49 (41.2) |
Ref | Ref |
| 101-250g (n = 148) |
80 (54.1) |
1.3 (1.0-1.7) |
1.7* (1.1-2.9) |
| 251-500g (n = 169) |
89 (52.7) |
1.3 (1.0-1.7) |
1.5† (0.9-2.5) |
| 501-750g (n =105) |
56 (53.3) |
1.3 (1.0-1.7) |
1.6* (0.9-2.7) |
| 751-1000g (n = 37) |
25 (67.6) |
1.6 (1.2-2.2) |
3.1* (1.4-6.8) |
| >1000g (n = 25) |
14 (56.0) |
1.4 (0.9-2.0) |
1.9* (0.8-4.6) |
Adjusted for prior vaginal delivery
Adjusted for prior vaginal delivery and diabetes
Discussion
In this large retrospective cohort, birth weight difference between the VBAC attempt and a prior cesarean for cephalopelvic disproportion had a moderate, though statistically significant, impact on VBAC failure; however, examination of the ROC curve reveals that birth weight difference is not a useful predictor of VBAC failure based on the modest area under the curve and the lack of a clear discriminatory point that could discern those that are destined for VBAC failure. A similar, though diminished, impact of birth weight difference was seen in patients whose prior cesarean was performed for failed induction and non-reassuring fetal status. Therefore, we conclude that the effect of birth weight difference is small and should not be used as a critical factor in deciding whether VBAC should be attempted. Allowing women with a larger infant than their prior pregnancy to attempt VBAC does not seem to increase the risk of complications.
We used actual birth weights in our analysis; however, clinicians must utilize estimated fetal weight either from physical exam or ultrasound, which has an error of 15-20% at term.(10, 11) Given the error in estimating fetal weight at term, the misclassification bias created by using estimated fetal weight would further decrease the ability to predict VBAC failure. Since actual birth weight does not generate a clinically useful prediction model for predicting failed VBAC, we anticipate that ultrasound-based estimated fetal weight will not either.
Several prior studies have examined the effect of macrosomia on VBAC success. Zelop et al found that a macrosomic fetus was associated with a decreased rate of VBAC success and no change in the risk of uterine rupture.(4) Elkousy et al confirmed the finding that macrosomia negatively impacts the rate of VBAC success, a finding which is exacerbated in the population with a prior indication of CPD. Although informative about the impact of macrosomia on VBAC, these studies do not include information about the impact of birth weight difference.
In a secondary analysis of a large prospective cohort study, Peaceman et al found that as the birth weight difference between the VBAC attempt and prior cesarean increased, the rate of VBAC success fell.(6) Every 100-g increase in infant birth weight resulted in a 3.8% decrease in the odds of a vaginal delivery. One of the main differences between their study and ours was the definition of the exposure; Peaceman et al included failed induction as part of CPD, whereas we analyzed this in a secondary analysis as failed inductions may or may not represent a subset of CPD patients. Additionally, we also included NRFS as a subset of CPD, and we examined complication rates in these groups.
The strengths of this study are its large size and comprehensive clinical data available, allowing us to examine outcomes, including maternal complications, in this very specific subset of patients. Also, we analyzed patients with a prior cesarean for failed induction or non-reassuring fetal status separately, as these may or may not represent cases of cephalopelvic disproportion.
An inherent limitation of a retrospective study is the possibility of selection bias. Specifically, physicians may encourage women who are “good” VBAC candidates (i.e. prior vaginal delivery, spontaneous labor) to attempt VBAC and encouraging patients who are poor candidates to undergo elective repeat cesarean. This type of selection bias may have diminished the observed impact of a larger infant on the rate of VBAC failure. Also, as the birth weight difference increased, the number of patients attempting VBAC decreased, thus limiting our power to detect a difference.
As this cohort was designed to investigate maternal risks associated with VBAC, we were unable to examine infant outcomes. Although we have extensive information available regarding maternal co-morbidities, information on maternal body mass index (BMI), which has been noted to be a variable affecting VBAC success, is unavailable in this cohort.(12, 13) Finally, a small number of patients did not have birth weight data available for both pregnancies, leading to another potential selection bias. However, these patients comprise only 9% of the study population and were characteristically similar to those in the study sample with few exceptions (less likely to be African American, more likely to deliver at a university hospital, slight differences in labor type).
Despite these limitations, we feel that clinically important conclusions can be drawn. Although birth weight difference modestly impacts VBAC success in patients with a prior cesarean for CPD, evaluation of birth weight difference incrementally and the ROC curve did not reveal a clear cutoff where the risk of failed VBAC became unacceptable. Therefore, we conclude that although VBAC failure increases moderately as VBAC birth weight increases over the index cesarean birth weight, we cannot make recommendations on a difference over which VBAC should not be attempted.
Acknowledgments
Supported by a grant from NICHD (RO1 HD 35631; to GAM). Dr. Harper is supported by a grant from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (T32HD- PI: Macones) and by UL1RR024992.
Footnotes
Financial Disclosure: The authors did not report any potential conflicts of interest.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Landon MB, Leindecker S, Spong CY, Hauth JC, Bloom S, Varner MW, et al. The MFMU Cesarean Registry: factors affecting the success of trial of labor after previous cesarean delivery. American Journal of Obstetrics & Gynecology. 2005;193(3 Pt 2):1016–23. doi: 10.1016/j.ajog.2005.05.066. [DOI] [PubMed] [Google Scholar]
- 2.Elkousy MA, Sammel M, Stevens E, Peipert JF, Macones G. The effect of birth weight on vaginal birth after cesarean delivery success rates. American Journal of Obstetrics & Gynecology. 2003;188(3):824–30. doi: 10.1067/mob.2003.186. [DOI] [PubMed] [Google Scholar]
- 3.Nwokoro CA, Njokanma OF, Orebamjo T, Okeke GC. Vaginal birth after primary cesarean section: the fetal size factor. Journal of Obstetrics & Gynaecology. 2003;23(4):392–3. doi: 10.1080/0144361031000119565. [DOI] [PubMed] [Google Scholar]
- 4.Zelop CM, Shipp TD, Repke JT, Cohen A, Lieberman E. Outcomes of trial of labor following previous cesarean delivery among women with fetuses weighing >4000 g. American journal of obstetrics and gynecology. 2001 Oct;185(4):903–5. doi: 10.1067/mob.2001.117361. [DOI] [PubMed] [Google Scholar]
- 5.Macones GA, Peipert J, Nelson DB, Odibo A, Stevens EJ, Stamilio DM, et al. Maternal complications with vaginal birth after cesarean delivery: a multicenter study. American Journal of Obstetrics & Gynecology. 2005;193(5):1656–62. doi: 10.1016/j.ajog.2005.04.002. [DOI] [PubMed] [Google Scholar]
- 6.Peaceman AM, Gersnoviez R, Landon MB, Spong CY, Leveno KJ, Varner MW, et al. The MFMU Cesarean Registry: impact of fetal size on trial of labor success for patients with previous cesarean for dystocia. American Journal of Obstetrics & Gynecology. 2006;195(4):1127–31. doi: 10.1016/j.ajog.2006.06.003. [DOI] [PubMed] [Google Scholar]
- 7.Dystocia and augmentation of labor. Obstetrics and gynecology. 2003 Dec;102(6):1445–54. doi: 10.1016/j.obstetgynecol.2003.10.011. ACOG Practice Bulletin Number 49, December 2003. [DOI] [PubMed] [Google Scholar]
- 8.Macones GA, Hankins GD, Spong CY, Hauth J, Moore T. The 2008 National Institute of Child Health and Human Development workshop report on electronic fetal monitoring: update on definitions, interpretation, and research guidelines. Obstetrics and gynecology. 2008 Sep;112(3):661–6. doi: 10.1097/AOG.0b013e3181841395. [DOI] [PubMed] [Google Scholar]
- 9.Dharan VB, Srinivas SK, Parry S, Ratcliffe SJ, Macones G. Pregestational diabetes: a risk factor for vaginal birth after cesarean section failure? American journal of perinatology. Mar;27(3):265–70. doi: 10.1055/s-0029-1239487. [DOI] [PubMed] [Google Scholar]
- 10.Anderson NG, Jolley IJ, Wells JE. Sonographic estimation of fetal weight: comparison of bias, precision and consistency using 12 different formulae. Ultrasound Obstet Gynecol. 2007 Aug;30(2):173–9. doi: 10.1002/uog.4037. [DOI] [PubMed] [Google Scholar]
- 11.Nahum GG, Stanislaw H. Ultrasonographic prediction of term birth weight: how accurate is it? American Journal of Obstetrics & Gynecology. 2003;188(2):566–74. doi: 10.1067/mob.2003.155. [DOI] [PubMed] [Google Scholar]
- 12.Durnwald CP, Ehrenberg HM, Mercer BM. The impact of maternal obesity and weight gain on vaginal birth after cesarean section success. Am J Obstet Gynecol. 2004 Sep;191(3):954–7. doi: 10.1016/j.ajog.2004.05.051. [DOI] [PubMed] [Google Scholar]
- 13.Hibbard JU, Gilbert S, Landon MB, Hauth JC, Leveno KJ, Spong CY, et al. Trial of labor or repeat cesarean delivery in women with morbid obesity and previous cesarean delivery. Obstet Gynecol. 2006 Jul;108(1):125–33. doi: 10.1097/01.AOG.0000223871.69852.31. [DOI] [PubMed] [Google Scholar]