

Abstract
Background
This cross-sectional study was conducted to obtain epidemiologic data on chronic musculoskeletal pain in the Japanese people, and with it a better understanding of the actual conditions and problems involved.
Methods
A questionnaire covering basic information, chronic musculoskeletal pain, daily life, quality of life, and social loss was prepared and mailed to 11507 individuals aged 18 years or older. Subjects were selected randomly nationwide in accordance with the demographic composition of Japan.
Results
The prevalence of chronic musculoskeletal pain was 15.4%. The prevalence was highest in people in their 30s to 50s. Pain occurred most frequently in the low back, neck, shoulder, and knee. Among symptomatic subjects, 42% sought treatment, by visiting a medical institution (19%), taking folk remedies (20%), or both (3%). Treatment was generally prolonged, with 70% of those treated reporting treatment durations of more than a year. Although 69% reported that their symptoms had improved, 30% reported unchanged or aggravated symptoms and dissatisfaction with treatment. Among symptomatic subjects, a high percentage of both men and women had lost jobs, left school, been absent from work or school, or had changed jobs. Basic activities of daily living (ADL) were disturbed in men, and the instrumental ADL (IADL) score was low in women. SF-36 scale scores were significantly lower in every area for subjects with chronic pain.
Conclusions
Chronic musculoskeletal pain does not necessarily improve even with prolonged treatment. It adversely affects daily life and both physical and mental health. Because those suffering pain often increasingly need assistance in daily activities, people around them are also affected. The therapeutic system and treatment procedures for chronic musculoskeletal pain merit prompt review.
Introduction
The National Livelihood Survey provides data on symptoms currently prevalent in the Japanese general population. According to this survey, low back pain, shoulder stiffness, joint pain, and headache are highly ranked [1]. The Japanese government has not implemented specific measures to address chronic pain types, for various reasons; for example, the pain is not life-threatening, therapy is cross-disciplinary, and conditions are not clearly defined. However, a US 2-year national survey that began in 1998 revealed that more than 9% of the adult population suffers from high levels of chronic pain, that medical resources are wasted on “doctor shopping” or ineffective treatment, and that the social cost of the difficulty of working in the presence of pain was 65 billion dollars annually, all of which drew attention to chronic pain as a medical and public health issue [2].
In Japan, even basic information needed to plan control measures for chronic pain has been lacking. Epidemiologic surveys of the prevalence of chronic pain have been conducted in countries in Europe and North America and have revealed that 9–24% of the adult population suffers from chronic pain, although there are variations in the numerical data because of differences between target populations and questionnaire contents [3–5]. In Asia, similar investigations have recently been carried out in Hong Kong and Singapore [6, 7]. To our knowledge, only one national-level survey of pain has been conducted in Japan. This large-scale study, reported by Hattori et al. [8], surveyed 18000 individuals living in different parts of Japan and found an estimated chronic pain prevalence of 13.4%. However, it should be noted that their study was conducted by an Internet survey in 2004, and the difficulty of internet access for those in their 60s or older, or those whose activities were limited by chronic pain, may have limited the range of possible participants. In view of these circumstances, the objective of this study was to determine the prevalence and actual status of chronic musculoskeletal pain in Japan and to gather the data necessary for formulating control measures from the perspectives of clinical medicine, public health, and administrative policy.
Methods
This epidemiologic survey used a mail-in survey panel designed by Nippon Research Center to obtain random samples from around Japan. This panel used an address-based random sampling system with a distribution of gender and age approximating that observed in the national population census. To obtain more than 10000 valid samples, a questionnaire was sent to 19198 subjects on the assumption that the response would be 55%. Valid responses were obtained from 11507 individuals (6365 females and 5142 males), so the response was 60% (Table 1).
Table 1.
Outline of the survey on the actual condition of chronic musculoskeletal pain
| 1. Region and subjects of survey: all over Japan |
| 2. Survey method: postal questionnaire survey |
| 3. Sampling method: stratified random sampling |
|
4. Period of survey: October to December 2010 11507 effective recovered samples, recovery 60% |
| 5. Screening conditions |
| (1) Male and female subjects aged 18 years old or older |
| (2) Persons who had had pain within the past month |
| (3) Pain persisting for at least 6 months |
| (4) Visual analog scale (VAS) equal to or exceeding 5 |
The questionnaire included questions on the following topics:
basic information (gender, age, place of residence, and occupation);
the actual status of chronic musculoskeletal pain (severity, site, and duration of pain);
treatment history (institution, treatment details and duration, cost, therapeutic effect, and degree of satisfaction);
activities of daily living (ADL) and quality of life (QOL) (using the Katz ADL scale and the Lawton instrumental ADL and SF-36 scales); and
social cost (job loss or changes, absences, resignation, and so forth).
In addition to simple summation, the prevalence of chronic pain was determined in relation to gender, area of residence, and city scale, and was compared by use of the chi-squared test. Subjects with and without chronic pain were compared with regard to the effect on working and by their scores on the Katz ADL scale, the Lawton instrumental ADL scale, and 8 subscale scores in the SF-36 quality-of-life (QOL) assessment. For the Katz ADL scale, the presence of disturbance was determined for 6 basic activities—bathing, dressing, using the toilet, getting into bed, continence, and eating—according to the need for partial or complete assistance. For intergroup comparisons, logistic regression analysis was used for category data and multiple regression analysis was used for continuous quantities, and p values were obtained after adjusting for age categories. The level of statistical significance was p < 0.05. This study was approved by the IRB of Keio University.
Results
Prevalence of chronic musculoskeletal pain
When asked, “Have you ever had pain associated with bone, muscle, joints, or nerves, such as neck pain, shoulder stiffness, low back pain, or extremity pain?”, 86% (9891) of the respondents answered, “Yes”. The time, duration, and severity of pain reported are shown in Fig. 1a–c. When chronic pain was defined as (1) a symptom present within the past month that (2) has continued for at least 6 months, and (3) corresponds to a visual analog scale (VAS) of at least 5, [5, 8] the prevalence among total respondents was 15.4% (1770 individuals) (Fig. 1d).
Fig. 1.
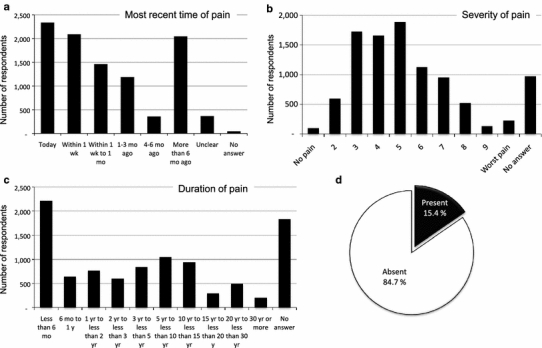
a Most recent occurrence of pain. b Severity of pain (visual analog scale). c Duration of pain. d Prevalence: percentages of those reporting the presence or absence of chronic musculoskeletal pain
Background factors found in those with chronic musculoskeletal pain
The prevalence of chronic musculoskeletal pain was significantly higher among women (16.8%) than men (13.6%). With regard to age, prevalence was highest in people in their 40s (18.6%), followed by those in their 30s (18.3%) and 50s (17%). Prevalence in relation to regions’ population was highest (16.4%) in 19 large cities, and decreased along with population density to the lowest (13.7%), which was found in rural districts (Table 2). A comparison of prevalence by occupation revealed higher prevalence among those doing professional work (20.5%), office and technical work (18.1%), and part-time work (16.9%), whereas the lowest prevalence was found in students (7.0%), followed by workers in agriculture, forestry, and fisheries (12%) and those with no occupation (13%) (Fig. 2).
Table 2.
Prevalence of chronic pain by gender, age category, area, and city size
| Number | Prevalence (%) | p value for χ 2 test | |
|---|---|---|---|
| All | 1770/11507 | 15.4 | |
| Gender | |||
| Women | 1071/6365 | 16.8 | <0.01 |
| Men | 699/5142 | 13.6 | |
| Age | |||
| 18–29 | 178/1295 | 13.8 | <0.01 |
| 30–39 | 357/1956 | 18.3 | |
| 40–49 | 369/1987 | 18.6 | |
| 50–59 | 318/1869 | 17.0 | |
| 60–69 | 296/2271 | 13.0 | |
| 70–79 | 223/1890 | 11.8 | |
| 80+ | 29/239 | 12.1 | |
| Area | |||
| Hokkaido | 80/551 | 15.7 | 0.494 |
| Touhoku | 103/755 | 13.6 | |
| Kanto | 710/4361 | 16.3 | |
| Chubu | 211/1323 | 16.0 | |
| Hokuriku | 67/480 | 14.0 | |
| Kinki | 289/1974 | 14.6 | |
| Chugoku | 96/680 | 14.1 | |
| Shikoku | 50/340 | 14.7 | |
| Kyushu | 164/1083 | 15.1 | |
| City size | |||
| Big city | 559/3403 | 16.4 | 0.058 |
| ≥150000 | 572/3659 | 15.6 | |
| <150000 | 471/3171 | 14.9 | |
| County | 129/942 | 13.7 | |
| No answer | 39/332 | 11.8 | |
Fig. 2.

Prevalence of chronic pain by occupations
Common sites of chronic musculoskeletal pain
Individuals with chronic musculoskeletal pain most frequently reported pain in the low back (65%), followed by the neck and shoulder (55% each), and the knee and surrounding area (26%) (multiple answers were allowed). The low back, shoulder, and neck were also highly ranked among sites of pain persisting for the longest periods (Fig. 3).
Fig. 3.
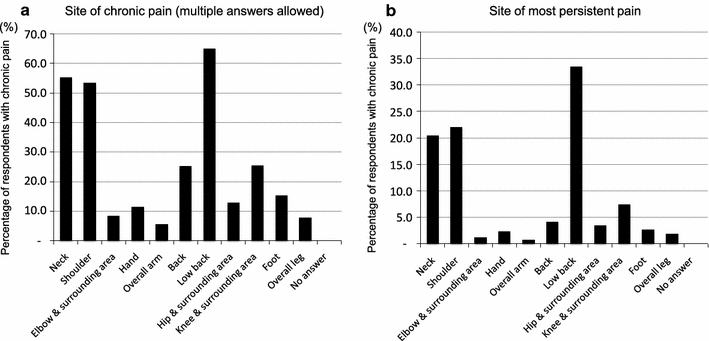
a Site of chronic pain (multiple answers allowed). b Site of most persistent pain
Actual status of treatment for chronic musculoskeletal pain
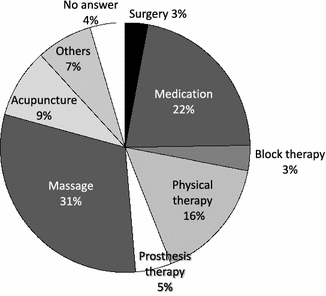
Analysis of answers regarding the current therapeutic status of chronic musculoskeletal pain showed that 42% of the symptomatic individuals sought treatment, at a medical facility (19%), through folk remedies (20%), or both (3%). Thus, medical institutions and folk remedies accounted for almost the same proportion of treatment (Fig. 4). The most commonly reported treatment frequency was less than once every 2 weeks (35%), followed by once weekly (25%), several times weekly (15%), and once every 2 weeks (15%). Treatment tended to be prolonged, with a duration of more than a year reported by approximately 70% of those who sought treatment (Fig. 5). The type of treatment most frequently chosen was massage (31%), followed by medication (22%), physical therapy (16%), and acupuncture (9%) (Fig. 6). The monthly cost of treatment (self-pay) was most frequently ¥3000–4000 (11%) or ¥5000–6000 (11%), but of special note is that approximately 8% of the symptomatic respondents spent ¥10000–15000 per month (Fig. 7).
Fig. 4.
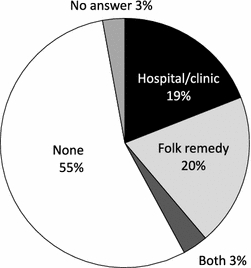
Type of treatment chosen for chronic pain
Fig. 5.
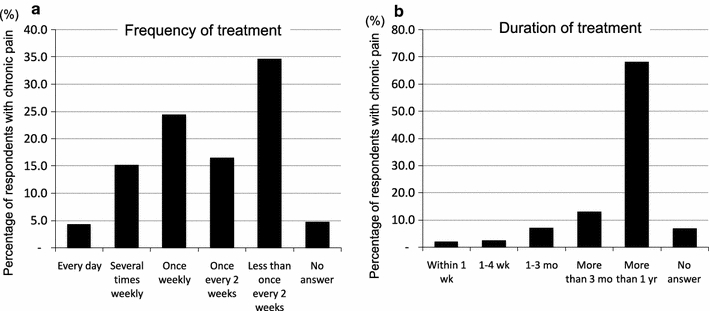
Treatment for chronic pain. a frequency; b duration
Fig. 6.
Type of treatment received for chronic pain
Fig. 7.
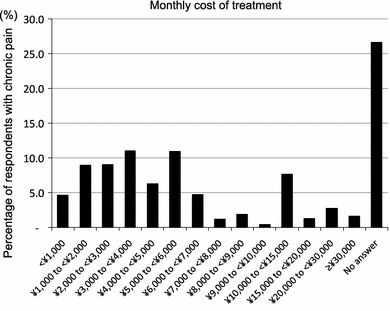
Monthly cost of treatment (self-pay) for chronic pain, excluding temporal expenditure, for example hospital admission and surgery
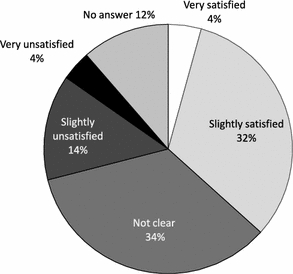
Of those with chronic pain who sought treatment, 49% changed their medical institution during treatment. The major reasons given for the change were that the previous treatment was not satisfactory (40%), a family member or a friend introduced a new institution (33%), the change was to a specialist for the specific pain (7%), or they were referred to another medical institution (7%) (Fig. 8). Very few reported that the pain was successfully eliminated by treatment (0.3%), although many reported an improvement (12%) or slight improvement (56%) of their symptoms, resulting in some improvement in almost 70%. Others reported that their symptoms were unchanged (21%), or slightly or distinctly aggravated (2%) (Fig. 9). In rating their satisfaction with the treatment received, only 4% considered their treatment to be very satisfactory. The remainder reported that their treatment was slightly satisfactory (32%), slightly unsatisfactory (14%), very unsatisfactory (4%), or they were “not clear” (34%) (Fig. 10).
Fig. 8.
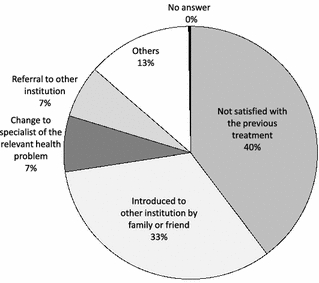
Reasons for changing medical institutions
Fig. 9.
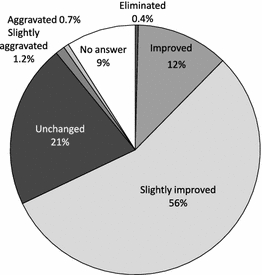
Efficacy of treatment for chronic pain
Fig. 10.
Satisfaction with treatment received
The effect of chronic musculoskeletal pain on daily and social life
An effect on work was defined as being present when respondents reported losing a job or leaving school (1.8% of the total respondents), absence from work or school (3.1%), changing jobs (1.2%), or changing the content of work (2.3%); some effect was found in 10% of the respondents. To determine the effect of chronic musculoskeletal pain on work, the results were compared between those with and without chronic pain. The percentage of those with versus without chronic pain was 14.6 versus 7.2% among women, and 17.6 versus 7.4% among men. Thus, the effect on work was statistically significant in those with chronic pain (Table 3). Analysis of the effect of chronic pain on basic ADL revealed that chronic pain affected continence in women, and bathing, dressing, using the toilet, continence, and eating in men. On the other hand, with regard to instrumental ADL (IADL), the Lawton score was lower in those with chronic pain among female respondents (Table 3). Comparison of the SF-36 QOL scores in those with and without chronic pain revealed that all the scores were significantly lower in those with chronic pain, for both women and men. It is worthy of special mention that chronic pain affected not only the responders’ physical health and ability to function in their roles, but also in their mental health and outlook in daily life (Table 3).
Table 3.
Effect on working, BADL, IADL and QOL score by chronic pain
| Women | Men | |||||
|---|---|---|---|---|---|---|
| Chronic pain (+) | Chronic pain (−) | Age-adjusted p value | Chronic pain (+) | Chronic pain (−) | Age-adjusted p value | |
| Number (%) | Number (%) | Number (%) | Number (%) | |||
| Effect on working | ||||||
| No effect | 889 (85.4) | 4788 (92.8) | <0.001 | 565 (82.4) | 4052 (92.6) | <0.001 |
| Effect (+) | 152 (14.6) | 371 (7.2) | 121 (17.6) | 323 (7.4) | ||
| Job loss/leaving school | 43 (4.1) | 71 (1.4) | 36 (5.3) | 55 (1.3) | ||
| Absence from work or school | 34 (3.3) | 130 (2.5) | 42 (6.1) | 154 (3.5) | ||
| Changing job | 36 (3.5) | 54 (1.1) | 16 (2.3) | 37 (0.9) | ||
| Changing the content of work | 39 (3.8) | 116 (2.3) | 27 (3.9) | 77 (1.8) | ||
| Dependence in BADL | ||||||
| Bathing | 9/1064 (0.9) | 25/5251 (0.5) | 0.067 | 9/696 (1.3) | 30/4420 (0.7) | 0.027 |
| Dressing | 8/1064 (0.8) | 22/5254 (0.4) | 0.073 | 10/696 (1.4) | 23/4420 (0.5) | 0.001 |
| Using the toilet | 2/1064 (0.2) | 11/5254 (0.2) | 0.983 | 5/696 (0.7) | 7/4422 (0.2) | 0.003 |
| Getting into bed | 1/1062 (0.1) | 11/5240 (0.2) | 0.516 | 3/695 (0.4) | 7/4419 (0.2) | 0.08 |
| Incontinence | 9/1063 (0.9) | 21/5256 (0.4) | 0.018 | 8/697 (1.2) | 26/4421 (0.6) | 0.024 |
| Eating | 1/1062 (0.1) | 10/5255 (0.2) | 0.6 | 6/697 (0.9) | 11/4421 (0.3) | 0.003 |
| IADL | ||||||
| Lawton score | 7.79 ± 0.64 | 7.85 ± 0.60 | <0.001 | 4.86 ± 0.50 | 4.87 ± 0.43 | 0.115 |
| QOL | ||||||
| PF | 47.74 ± 12.98 | 51.14 ± 10.31 | <0.001 | 49.51 ± 11.60 | 52.73 ± 9.11 | <0.001 |
| RP | 45.50 ± 11.78 | 49.62 ± 9.85 | <0.001 | 47.94 ± 11.40 | 51.12 ± 9.18 | <0.001 |
| BP | 39.87 ± 6.72 | 47.96 ± 9.32 | <0.001 | 40.56 ± 6.98 | 50.29 ± 9.33 | <0.001 |
| GH | 46.40 ± 10.16 | 51.67 ± 9.74 | <0.001 | 46.03 ± 10.37 | 51.91 ± 9.94 | <0.001 |
| VT | 44.04 ± 10.23 | 49.76 ± 9.70 | <0.001 | 45.11 ± 10.50 | 51.20 ± 9.76 | <0.001 |
| SF | 46.29 ± 11.75 | 49.43 ± 10.53 | <0.001 | 48.61 ± 11.36 | 51.68 ± 9.21 | <0.001 |
| RE | 46.48 ± 11.63 | 49.63 ± 9.86 | <0.001 | 48.58 ± 11.01 | 51.34 ± 8.95 | <0.001 |
| MH | 46.83 ± 10.63 | 50.41 ± 9.49 | <0.001 | 47.66 ± 10.56 | 51.34 ± 9.38 | <0.001 |
Discussion
Characteristic features of this survey
Large-scale surveys have been carried out in Europe and the US in recent years to evaluate the effect of chronic pain on society, and new policies for treating chronic pain have evolved on the basis of the results of such surveys. However, in Japan, there has been a paucity of basic information on the status of chronic pain; only one previous survey, conducted by Hattori et al. [8], has been reported. Our study differs from the epidemiologic study conducted by Hattori et al. in the following aspects:
our survey focused specifically on chronic musculoskeletal pain;
samples were made to approximate the population composition of Japan by random sampling with distribution quotas for gender, age, and location; and
the survey was carried out not via the Internet, but by sending and recovering questionnaires.
The actual status of chronic musculoskeletal pain in Japan
Our survey found 15.4% prevalence of chronic musculoskeletal pain. This figure is substantially higher than the 13.4% prevalence reported by Hattori et al., which was based on chronic pain in any part of the body, and not restricted to the musculoskeletal system [8]. However, Hattori et al. used stratified random sampling via the Internet from an already-registered panel. This may have resulted in lower-than-actual prevalence, because Internet usage may have placed a large bias against middle-aged or elderly people, who often have chronic pain.
Regarding the possible background factors in persons with chronic pain, both our study and the Hattori study found greater prevalence in women. There were some differences in age-related findings between the two studies; Hattori et al. found prevalence was lowest in those less than 30 years of age, tended to rise through the 30s and 40s, and was highest in middle-aged or elderly persons (50 years of age or older). However, in our study we found significantly higher prevalence (17–19%) in those in their 30s to 50s—often called the working generation—than in other age groups. This was consistent with our findings that the prevalence was higher in large city areas than in rural districts, and that high prevalence of chronic musculoskeletal pain was found in those engaged in professional jobs, office or technical work, part-time jobs, and labor service/skilled work, whereas it was low in those without any occupation or those engaged in agriculture, forestry, and fisheries work.
The discrepancy between the two studies may be attributable to the difference between examining chronic musculoskeletal pain and examining any chronic pain. However, because both studies reported the low back, neck, shoulder, and knee as frequent sites of pain, it is more likely that the discrepancy is because of the previously mentioned difference in survey method.
Issues in the actual treatment of chronic musculoskeletal pain
Currently, 45% of persons with chronic musculoskeletal pain are receiving treatment. The proportion of people receiving treatment from medical facilities, for example hospitals and clinics, is almost the same as that of people who are using folk medicine. Reflecting this finding, the major types of treatment reported were massage and acupuncture, accounting for 40%, followed by medication (22%), physical therapy (16%), and prosthetic therapy (5%).
The frequency of treatment was less than once every 2 weeks for most respondents (35%), followed by once weekly (25%) and several times weekly or once every 2 weeks (15% each). Treatment was usually prolonged; 70% of those receiving treatment reported that they had been undergoing treatment for a year or longer. Just over half of those who sought treatment did not feel their treatment was satisfactory, reporting that they were slightly unsatisfied (14%), very unsatisfied (4%), or “not clear” (34%). Approximately half of those who sought treatment reported having changed their medical institution, and most of these (40%) reported that the previous treatment was not satisfactory. Therefore, the results of this study cast light on the issue that “doctor shopping”, or changing medical institutions repeatedly in a short period of time, is common with people who have chronic musculoskeletal pain and are not satisfied with their current treatment.
The cost of treatment (self-pay) was most frequently at the ¥3000 or ¥5000 level per month (11% each). It is noteworthy that approximately 8% of persons spent ¥10000–15000 per month. Taking into consideration the tendency toward prolonged treatment, it is apparent that the healthcare cost of chronic musculoskeletal pain is quite high and has a large effect on medical economics.
Effect of chronic musculoskeletal pain on daily and social life
When the respondents with and without chronic pain were compared in terms of physical and mental health performance, as determined by their SF-36 scores, all the scores were significantly lower for those with chronic pain. This indicates that chronic musculoskeletal pain has a large effect not only on an individual’s physical condition and ability to function but also on his or her mental health and activities in daily life. Consistent with these findings, the effect of chronic musculoskeletal pain on working can be seen in that the incidence of job loss, leaving school, absences from school or work, and job change were significantly greater in persons with chronic pain than in those without it. When those with and without chronic musculoskeletal pain were compared in the areas of basic ADL and IADL, the effect of chronic pain was noted for basic ADL in men and for IADL in women. These results show that chronic musculoskeletal pain has a large effect on the social and daily life activities of symptomatic individuals, and that their increased need for assistance in daily living also greatly affects the social and daily lives of the people around them. On the basis of the results of this survey, the therapeutic system and treatment procedures for chronic musculoskeletal pain should be reviewed promptly.
Acknowledgments
This study was carried out as a 2010 multidisciplinary research project for measures to help the handicapped (survey study of chronic musculoskeletal pain), supported by a Grant-in-Aid for Scientific Research from the Ministry of Health, Labour, and Welfare.
Conflict of interest
The authors declare no conflict of interest.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
References
- 1.Annual Statistical Report of National Health Conditions. 2010/2011 pp 72–3, Health and Welfare Statistics Association (Japanese).
- 2.National Institutes of Health (Internet). NIH guide: new directions in pain research: I. Bethesda, MD: National Institutes of Health. 1998.
- 3.Breivik H, Collett B, Ventafridda V, Cohen R, Gallacher D. Survey of chronic pain in Europe: prevalence, impact on daily life, and treatment. Eur J Pain. 2006;10:287–333. doi: 10.1016/j.ejpain.2005.06.009. [DOI] [PubMed] [Google Scholar]
- 4.Eriksen J, Jensen MK, Sjøgren P, Ekholm O, Rasmussen NK. Epidemiology of chronic non-malignant pain in Denmark. Pain. 2003;106:221–228. doi: 10.1016/S0304-3959(03)00225-2. [DOI] [PubMed] [Google Scholar]
- 5.Rustøen T, Wahl AK, Hanestad BR, Lerdal A, Paul S, Miaskowski C. Prevalence and characteristics of chronic pain in the general Norwegian population. Eur J Pain. 2004;8:555–565. doi: 10.1016/j.ejpain.2004.02.002. [DOI] [PubMed] [Google Scholar]
- 6.Ng KF, Tsui SL, Chan WS. Prevalence of common chronic pain in Hong Kong adults. Clin J Pain. 2002;18:275–281. doi: 10.1097/00002508-200209000-00001. [DOI] [PubMed] [Google Scholar]
- 7.Yeo SN, Tay KH. Pain prevalence in Singapore. Ann Acad Med Singapore. 2009;38:937–942. [PubMed] [Google Scholar]
- 8.Hattori S, Takeshima N, Kimura N, Yamamoto K, Mizutani A, Noguchi T. The clinical perspective on chronic pain management in Japan. Pain Clinic 2004;25:1541–51 (Japanese).