

Abstract
Background:
Post operative analgesia in patients undergoing lower limb surgery is very essential for immediate postoperative pain relief which can be provided by oral or parentral medication, epidural analgesia, local blocks etc.The study was designed to evaluate the efficacy of epidural butorphanol and tramadol for postoperative pain relief.
Patients & Methods:
This was randomized, prospective, double blind study was conducted on 60 patients, ASA grade I&II, age 18-60 undergoing lower limb surgeries after approval from hospital ethics committee. Group allocation - Group I I (n=30) received 2 mg butorphanol as bolus epidurally, 1 mg for top up dose. Group II (n=30) received 100mg tramadol as bolus, 50 mg for top up. All the drugs were diluted to 10 ml normal saline & the observer was blinded to the drugs given. Postoperatively VAS, sedation score, vitals & side effects were observed. Top ups were given on achieving VAS>4. Diclofenac 75mg was given as rescue analgesia.
Results:
Duration of analgesia was 5.35±0.29 hr and 6.25±1.58 hrs in Butorphanol and Tramadol groups respectively and the difference was found to be statistically significant. Pain scores were also significantly lower statistically in Group I as compared to Group II. Sedation scores were significantly higher in butorphanol group, whereas nausea vomiting was seen in tramadol group only (4 patients).No other side effects were observed.
Conclusions:
Both butorphanol and tramadol were effective for relieving postoperative pain, however quality of analgesia & patient satisfaction was more with butorphanol.
Keywords: Epidural, Tramadol, Butorphanol, Post-operative Pain
Postoperative pain gives rise to various physiological and psychological phenomenon and effective pain control is vital for early mobilization and postoperative discharge.1 Epidural analgesia using local anesthetic agent is popular simple, effective and economical way of providing postoperative analgesia. Due to short duration of local anesthetic, opioids have been added, so that even small doses can provide profound analgesia of good duration with few side effects. Both butorphanol, a mixed agonist-antagonist opioid and tramadol hydrochloride a moderately potent opioid agonist have been used for this purpose separately in few studies.2,3 We carried a study to compare the effectiveness of butorphanol and tramadol as postoperative analgesics when given epidurally.
PATIENTS AND METHODS
The present study was conducted on 60 patients of age 18-60 years of ASA grade I and II undergoing lower limb surgeries after attaining approval from hospital ethics committee. Patients with neurological disorders, bleeding tendency, sepsis, spinal deformity, suffering from asthma, cardiac, respiratory, renal, hepatic and CNS diseases and hypersensitivity to local anesthetics or study drugs were excluded from the study.
After taking informed consent, patients were randomly allocated to one of the two groups of 30 patients each. The study was done in double blind manner by making 60 coded slips. The person performing the procedure and carrying out the observation was blinded to drug solution injected. The drug solution was prepared in two separate syringes of 10 ml and 20 ml. Detailed preanaesthetic checkup was done a day prior to surgery and patient kept fasting for 6-8 hours. Patients were explained about linear visual analogue score (VAS) using a 11 centimeter line, where 0 denoted “no pain” while 10 “worst pain imaginable”. On day of surgery tablet alprazolam 0.25 mg orally was given 2 hours prior to surgery and patients were reassessed in the preanaesthetic room.
In operation theatre intravenous line with ringer's s lactate was started and all the patients were preloaded at rate of 10 ml per kg over 15-20 minutes. Readings of heart rate (HR), blood pressure (BP) and peripheral arterial oxygen saturation (SpO2) were taken as baseline.
After positioning the patients and taking all aseptic precautions epidural needle was introduced and space identified using loss of resistance to air technique. Epidural catheter was inserted. All patients were given spinal anaesthesia for the surgical procedure one space lower than the insertion site of epidural catheter using 25G spinal needle and 2.5-3ml of heavy bupivacaine 0.5% was given. Sensory and motor effect was checked.
At the end of surgical procedure sensory level and motor effects were determined. When VAS for pain reached 4, then bolus from 10 ml syringe was given to all the patients depending upon groups. Patients in Group I (n=30) received 2 mg of inj. butorphanol dissolved in 9 ml of normal saline (total volume 10 ml) epidurally. For top up 2 mg inj. butorphanol was dissolved in 19 ml of normal saline (total volume 20 ml) and 10 ml of this solution was given for each top up. Patients of Group II (n=30) were given 100 mg of inj. tramadol dissolved in 8 ml of normal saline (total volume 10 ml) epidurally. For top up 100 mg of inj. tramadol was dissolved in 18 ml of normal saline (total volume 20ml) and 10 ml of this solution was given as top up.
For the rest of postoperative period, patients were given top up doses from 20 ml syringe on having pain of VAS>4. In case more doses were required the supervisor provided additional doses filled in 20 ml syringe according to the group.
Patients were assessed at half-hourly intervals for first two hours then at 4, 8, 12, 24 hours after giving first dose of epidural opioid for the following variables A. Visual analogue scale (VAS) 0-no pain, 1-3-mild pain, 4-7-moderate pain, 8-10-severe pain. B. Sedation score'0 = Fully awake, 1 = Slightly drowsy, 2 = Asleep but easily arousable, 3 = Fully asleep but arousable, 4 = Fully asleep and not arousable. C. HR and BP. D. Monitoring of respiratory rate (RR) and SpO2. E. Side effects such as nausea, vomiting, retention of urine, pruritis and respiratory depression.
Timing of incremental doses, interval between injections and total dose given in 24 hours were recorded. If analgesia was found inadequate even after two consecutive epidural doses given 20-30 minutes apart, patients were given diclofenac sodium 75 mg intramuscularly as rescue analgesia.
At the end of the study decoding of groups was done and all values expressed as mean+standard deviation (SD) range ; a p value of <0.05 was considered statistically significant. The results were analyzed using SPSS11.5 software. The student's t-test was used for testing the significance of hemodynamic variables, post operative pain score and duration of analgesia between the groups. The chi-square test was used to test the demographic variables, number of epidural dosages required over 24 hrs and the post operative side effects.
RESULTS
The two groups were comparable with regards to age, sex, sensory level achieved during spinal anaesthesia and du-ration of surgery (Table 1). Preoperative readings of heart rate, blood pressure and peripheral arterial oxygen satura-tion measured were comparable. Among postoperative pa-rameters mean pulse rate, systolic and diastolic blood pressure decreased significantly (p<0.05) when compared with the 0 hour at all the time intervals during the 24 hour period in both the groups, but on intergroup comparison the difference in mean pulse rate, systolic and diastolic blood pressure was not found statistically significant (p>0.05).Mean duration of analgesia (taken from bolus in-jection given epidurally to the requirement of 1st top up) was significantly higher (p<0.05) in group II when compared with 2mg butorphanol (Table 2).
Table 1.
Demographic profile
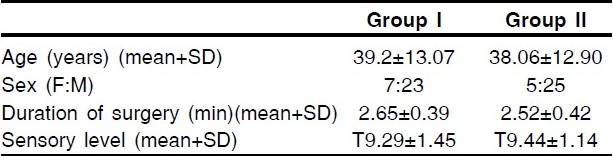
Table 2.
Duration of Analgesia

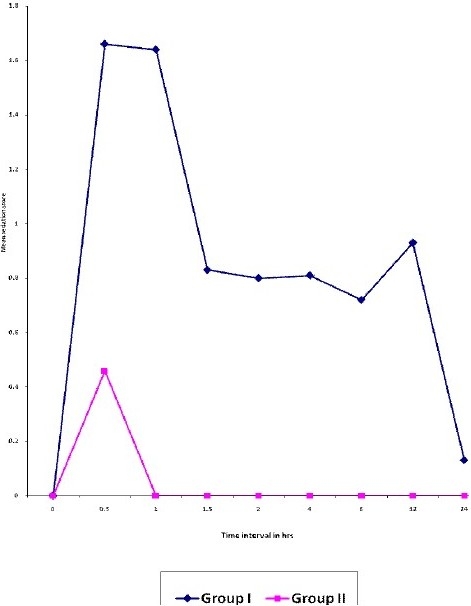
The mean VAS score between the groups was highly significant (p<0.001) at 0.5, 1, 1.5, 2 hrs; significant (p<0.05) from 4 to 8 hours and at 12, 24 hours it was insignificant statistically (p>0.05) (Fig I). The mean time of 1st, 2nd and 3rd epidural top ups of tramadol was much longer com-pared to butorphanol.
Figure 1.
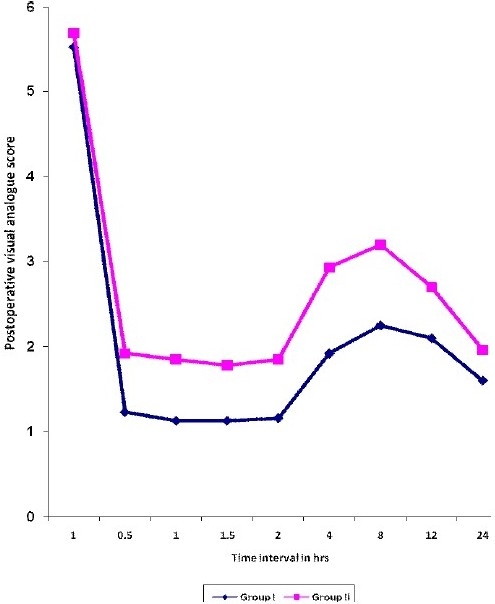
Mean VAS scores at various time intervals
In group I (butrophanol), majority of the patients re-quired 4 dosages while in group II (tramadol) 3 dosages were required (Table 3) for pain relief, and this difference was highly significant statistically.(p<0.001) No patient in group I (butorphanol) required rescue analgesia whereas 2 patients in group II (tramadol) required rescue analgesia.(Table 4).
Table 3.
Comparison of Number of Epidural Dosages Required To Produce Analgesia Over 24 Hours
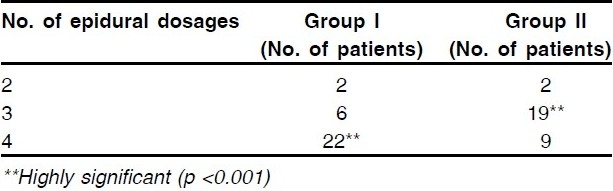
Table 4.
Rescue Analgesia

Nausea and vomiting was seen in group II in 4 out of 30 patients each, which was found significant statistically from group I i.e. butorphanol group, where no patient had such problem. No other complication was observed in either group. Sedation was seen in 28 out of 30 patients of group I (butorphanol) whereas 14 out of 30 patients had sedation in group II (tramadol) which was highly significant (p<0.001) (Table 5). Sedation score between the groups was found to be highly significant statistically (p <0.001) (Fig II.
Table 5.
Postoperative Side Effects
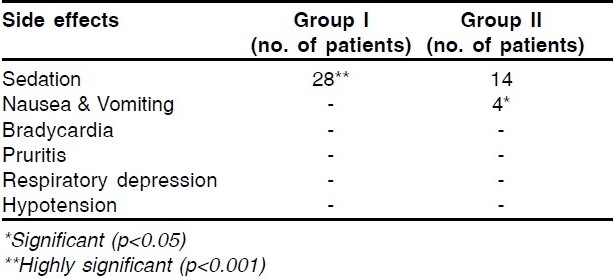
Figure 2.
Mean sedation scores at various time intervals
DISCUSSION
Effective pain control is essential and has been recognized as a prime concern for anaesthesiologists.4 Epidural route is used extensively for postoperative pain control. Combined spinal epidural anaesthesia finds a common place for perioperative management of orthopaedic surgery. It combines the advantages of both spinal and epidural technique by initially providing an intense sensory and motor block of rapid onset. After the surgical procedure and regression of spinal analgesia, the epidural catheter can be used to provide post operative pain relief.4
Opioids acting on spinal cord receptors provide distinct advantage over its systemic administration for better quality of analgesia, lower sedation scores, preservation of physiological function and improved outcome.1
Our study shows that tramadol had a longer duration of analgesia when compared to butorphanol for postoperative epidural analgesia. Abboud TK et al5 and Dhimar A et al1 found an analgesia lasting 5.53+0.86 hours and 8 hours respectively with epidural butorphanol. Sayyid S et al6 and Rathie P et al7 in their study on epidural tramadol (100 mg) for postoperative pain relief found the duration of analgesia to be 4.5±3.1 hours and 10.26+2.73 hours respectively. These results were different from our study may be because of the difference in the type of surgery or may be due to addition of local anaesthetic agents to the study drug.
The significant decrease observed in mean pulse rates, systolic and diastolic blood pressure from the baseline readings seen in both the groups which could be due to increased initial values because of pain (VAS -4) and reduced significantly after effective analgesic action of the drugs.
Comparison of VAS scores at various time interval in both the groups showed that butorphanol was able to relieve pain in much better way than tramadol upto 8 hours after which pain releif was similar. Palacios Q et al8 found decreased VAS with epidural butorphanol similar to ours, whereas Rawal H et al9 had decreased VAS scores with epidural tramadol 100 mg compared to our study.
Main side effects seen during the study were nausea, vomiting with tramadol and mild sedation in butorphanol group which was considered desirable rather than a side effect in our patients.
Thus we conclude that both butorphanol and tramadol were effective for postoperative analgesia when used epidurally in patients undergoing lower limb surgery. Butorphanol although has shorter duration of analgesia but better pain relief compared to tramadol. It also caused less nausea and vomiting and slight sedation which was rather desirable. Whereas with tramadol longer duration of analgesia with no sedation, more nausea and vomiting was observed. Authors suggest that more prospective studies are required to in order to recommend any drug as useful adjunct for enhancing post operative analgesia.
REFERENCES
- 1.Dhimar AA, Patel MG, Swadia VN, Desai DJ. Epidural butorphanol: Comparison of two different doses for lower limb orthopaedic surgery. J Anaesth Clin Pharmacol. 2006;22(1):47–52. [Google Scholar]
- 2.Malik P, Manchanda C, Malhotra N. Comparative evaluation of epidural fentanyl and butorphanol for postoperative analgesia. J Anaesth Clin Pharmacol. 2006;22(4):377–82. [Google Scholar]
- 3.Lakhotiya R, Tanwar GL, Jain S, Vyas KP. Epidural tramadol for postoperative pain relief. Indian J Anaesth. 1998;42(1):38–42. [Google Scholar]
- 4.Wu CL. Anesthesia. 6th ed. Pennsylvania: Churchill Livingstone; 2005. Acute postoperative pain; pp. 2764–5. [Google Scholar]
- 5.Abboud TK, Moore M, Zhu J, Murakawa K, Minehart M, Longhitano M, et al. Epidural butorphanol or morphine for the relief of post-cesarean section pain: ventilatory responses to carbon dioxide. Anesth Analg. 1987;66:887–93. [PubMed] [Google Scholar]
- 6.Sayyid SS, Maroun MA, Sleiman D, Sfeir M, Baraka A. Epidural tramadol for postoperative pain after cesarean section. Can J Anesth. 1999;46(8):731–5. doi: 10.1007/BF03013907. [DOI] [PubMed] [Google Scholar]
- 7.Rathie P, Verma RS, Jatav TS, Kabra A. Postoperative pain relief by epidural tramadol. Indian J Anaesth. 1998;42:26–31. [Google Scholar]
- 8.Palacios TQ, Jones MM, Hawkins JL, Adenwala JN, Longmire S, Hess KR, et al. Post- Cesarean section analgesia: A comparison of epidural butorphanol and morphine. Can J Anaesth. 1991;38:24–30. doi: 10.1007/BF03009159. [DOI] [PubMed] [Google Scholar]
- 9.Rawal HH, Swadia VN, Patel HJ. Epidural tramadol bolus and continuous infusion. Indian J Anaesth. 1995;43:193–7. [Google Scholar]