

Abstract
Objective:
To determine the effectiveness of rugby headgear and the effect of impact site and headgear type on attenuating repetitive linear impact forces.
Design and Setting:
We obtained 10 headgear of 2 different types (n = 20) from 2 popular manufacturers: type I was Honeycomb headgear and type II was Vanguard headgear. Both headgear types were approved by the International Rugby Board. Headgear were tested according to National Operating Committee on Standards for Athletic Equipment protocols with one modification. The headgear were dropped from a height of 30 cm according to the International Rugby Board standards. Headgear were tested at a National Athletic Equipment Reconditioners Association facility.
Measurements:
We recorded peak acceleration of gravity (g) and Gadd Severity Index readings for each impact. The design of the study was 4 one-way, within-subjects, repeated-measures analyses of variance with alpha = .05. Descriptive statistics were calculated for all categoric variables.
Results:
Peak g and Gadd Severity Index increased with repetitive impacts, resulting in a headgear's decreased ability to attenuate linear impact forces. Attenuation differed significantly between headgear type I and type II at both impact sites and between the parietal-lateral and occipital impact sites for both headgear types.
Conclusions:
The headgear initially attenuated impact forces from a drop height of 30 cm. However, over 10 drops, both headgear decreased in their ability to attenuate repetitive linear impact forces. Decreased attenuation in the occipital region as well as significant differences in attenuation abilities between headgear types support the need for further investigation to examine the efficacy of rugby headgear.
Keywords: concussion, protective equipment, Gadd Severity Index, peak g
An estimated 300 000 sport-related traumatic brain injuries (TBIs) occur each year. The concussion, a type of mild TBI, is defined as an alteration in mental status caused by biomechanical forces that may or may not produce unconsciousness.1,2 More than 800 sport-related concussions occur each day in the United States, making concussion the most common acute brain injury in sports.1,2 A single concussion and the cumulative effects of repeated concussions both present serious risks to athletes participating in collision sports.1
Rugby is a collision sport in which repetitive impacts between players and with the playing surface occur throughout the game.3 Rugby is physical in nature, and injury is an inevitable aspect of the game.4–7 Up to 72% of rugby players experience at least 1 injury related to rugby during a competitive season5 and 82% within a 1-year period.8 Injury incidence rates vary greatly from 114.37 to 490.29 per 1000 player-position game hours, with an increased rate of injury to forwards compared with backs.4,7 Concussions alone account for up to 25% of all rugby injuries.5,8,10,11
Because of the high incidence of collisions and resultant concussions suffered by rugby athletes, we need to determine ways to reduce the risk of head injury during participation. In the past, rugby was typically played without the use of any protective equipment. However, advancements in protective padding, including headgear, have led to a recent increase in use among participants. In 1999, 60%10 to 79%12 of youth (<15 years old) rugby union players in Australia used protective headgear. Headgear usage has become mandatory in Japan.13 Many of these youth athletes wear headgear with confidence that it protects them from head injury.10,13 Although the use of protective headgear in the prevention of lacerations and abrasions that may occur to the head region is supported by research,13–15 findings thus far do not support the use of protective headgear in reducing the risk of concussions.3,12,15 However, manufacturers market headgear for “shock absorption” and “impact resistance.”16
McIntosh et al3,12 reported the parietal-temporal region as the most common impact site resulting in concussion, followed by the occipital region, 86% and 10%, respectively.3 Rugby headgear is traditionally designed so that a laced-up tie is located in the occipital region (Figure 1). This design raises concern about the attenuation capabilities of this region, but researchers examining rugby headgear to date have not addressed impacts to the occipital region of the head. Another issue regarding rugby headgear is that the soft, closed-cell foam material used to manufacture headgear may possess a “memory effect,”12 such that the foam does not return to its original thickness after impact. This is a concern because repetitive impacts to the headgear may reduce its ability to attenuate forces and lessen its effectiveness over time.12
Figure 1.

Posterior view of headgear type I (left) and type II (right).
Research focusing on rugby headgear has been especially limited in the United States despite the sport's growing popularity. Our purpose was to determine if rugby headgear attenuate repetitive linear impact forces and to examine the effects of headgear type and impact site on rugby headgear performance. The National Operating Committee on Standards for Athletic Equipment (NOCSAE), the primary United States governing body responsible for determining the approval criteria for protective sporting equipment, currently has no impact-testing standards for rugby headgear. We adapted the NOCSAE drop-testing protocol and applied it to rugby headgear with a single modification to the drop height. In addition, we also examined the occipital impact site and decreased time between impact tests, which are variables previously unstudied in the literature.
METHODS
Headgear
We used 2 styles of rugby headgear approved by the International Rugby Board (IRB, Dublin, Ireland): type I was Honeycomb headgear (Canterbury of New Zealand, Porirua, New Zealand) and type II was Vanguard headgear (James Gilbert Ltd, Rugby, England) (Figure 2). The IRB approval standards are soft-foam thickness of no more than 1 cm, density of foam no more than 45 kg/m3, and headgear meeting the criteria for impact testing. The IRB criterion for acceptable impact-testing performance is limited to peak g of no less than 200g, not to exceed 550g at a drop height of 30 cm.17 A sample (n = 20) of medium-sized headgear was selected. Both types were from reputable rugby supply companies popular among rugby players. Type I (n = 10) consists of small, individual hexagonal and pentagonal sections of padding made of a high-density, closed-cell foam. The thickness of these padded areas is 1.0 cm, and the length of each padded area ranges from 2.60 cm to 3.30 cm, depending on shape. The average weight of headgear type I was 96.39 g. Type II (n = 10) consists of continuous sections of padding made of Triflex foam (Triflex Industries, Alpena, MI), which is similar in construction to the type I headgear. The thickness of the padded areas is 0.70 cm at the parietal-lateral region and 0.80 cm at the occipital region. The average weight of headgear type II was 73.71 g. The parietal-lateral aspect of the headgear is projected outward to allow space for the ear. This study was approved by the university's institutional review board.
Figure 2.

Parietal-lateral view of headgear type I (left) and type II (right).
Instrumentation
The equipment we used included a Hybrid III headform, a triaxial accelerometer, a mechanical drop-testing carriage assembly, a Modular Elastometer Programmer (MEP) pad (all from Southern Impact Research Center, Knoxville, TN), and a Severity Index Computer System KME Series 200 (KME Series 200 Data Analyzer, KME Co, Troy, MI).18 The Hybrid III headform possesses a high degree of biofidelity, accurately simulating the human head's response to impact accelerations.19,20 The medium-sized headform measures 575 mm in circumference and weighs 4.8 kg, including the neck. It incorporates a polychlorinated biphenyl 3-dimensional piezoelectric accelerometer (model 354MO3; PCB Piezotronics, Inc, Depew, NY), mounted internally at the center of gravity and glycerin sealed in the cranium. The triaxial accelerometer is designed to measure the peak acceleration of gravity in 3 orthogonal directions: the x axis (anterior-posterior), the y axis (superior-inferior), and the z axis (left to right).18,20–25 The peak acceleration of gravity occurs at the headform's moment of impact.
Calibration
Before data collection, the carriage assembly was checked for any imperfections.26,27 The headform and triaxial accelerometer located at the headform's center of gravity were then calibrated according to NOCSAE protocol.26,27 The headform was released from 3 specified heights onto an anvil padded with a 7.6 × 15.2-cm-diameter MEP pad molded from polyurethane thermoplastic elastomer.27
We turned the computer on for 45 minutes before testing and allowed it to stabilize at the proper temperature of 22°C ± 2°C.26,27 Calibration began with a drop to the front of the headform from a height of 144.78 cm, followed by a drop to the side from 132.08 cm, and finally a drop to the crown from 111.76 cm. The resulting Gadd Severity Index (GSI) levels were within normal limits (1200 GSI ± 2%).27
Measurements
Impact attenuation was determined for all headgear by measuring the headform's peak instantaneous acceleration on contacting the MEP pad. Results for each of the 3 orthogonal axes were recorded by the headform's internally mounted triaxial accelerometer. The NOCSAE-recommended Severity Index computer recorded impulse signals from the triaxial accelerometer using a 4-pole, 1650-Hz filter and computed the GSI using an integration equation (Figure 3).26,28–30
Figure 3.

Formula for calculating Gadd Severity Index. A is the instantaneous resultant acceleration expressed as a multiple of g or acceleration of gravity; dt are the time increments in seconds; and the integration is carried out over the essential duration (T) of the acceleration pulse.18.
Testing Procedures
Testing was conducted at an approved National Athletic Equipment Reconditioners Association testing center. All drop-testing procedures were performed according to NOCSAE protocols with a modified drop height according to the IRB standard for this sport-specific headgear.17,18,22–29 Standards for protective helmets in the United States used in collision sports such as football, lacrosse, and baseball are regulated by NOCSAE. The IRB regulates all the laws and standards for the sport of rugby worldwide. The NOCSAE protocols require air and helmet temperature to be maintained at 22°C ± 2°C. All headgear were properly applied to the headform according to the manufacturer's specifications.16 The headgear was placed on the headform with the anterior portion aligned 1–2 cm above the brow line. The chinstrap was then adjusted and secured. A gap in the headgear was present where the right and left posterior sections laced together. This gap was measured with a vernier caliper to ensure an approximately equal fit between the headgear. This distance was approximately 1.7 cm for type I headgear and 2.0 cm for type II headgear. Discrepancies in fit were attributed to differences in design between the models. The samples of type I (n = 10) and type II (n = 10) headgear were randomly numbered 1 through 10. Each headgear was then assigned to one of 2 treatment groups. Group A consisted of headgear numbered 1 through 5 from types I and II. Group B consisted of headgear numbered 6 through 10 from types I and II. We randomized drop-site order to control for any effect on impact attenuation.
The headgear was raised using the carriage assembly to a height of 30 cm, as specified by IRB standards. The headgear was then released in a gravity-induced free fall. Two wires guided the headgear onto a rigid anvil, padded with a 1.3 × 15.2-cm-diameter, 45-durometer hardness-testing MEP pad that is designed to simulate the playing surface.18,22–26,28,29 After each impact, the equipment was reset, and the same headgear testing process was repeated a total of 10 times, with 30 seconds between impacts. Group B was first tested at the occipital impact site, or rear, as termed by NOCSAE.18 Once we tested these 10 headgear, we adjusted the testing apparatus to the parietal-lateral, or lateral, position as termed by NOCSAE (Figure 4).18 Group A was tested at the parietal-lateral impact site. Group B was then also tested at this site. Once this testing was completed, we again adjusted the testing apparatus to the occipital site, where group A was then tested.
Figure 4.
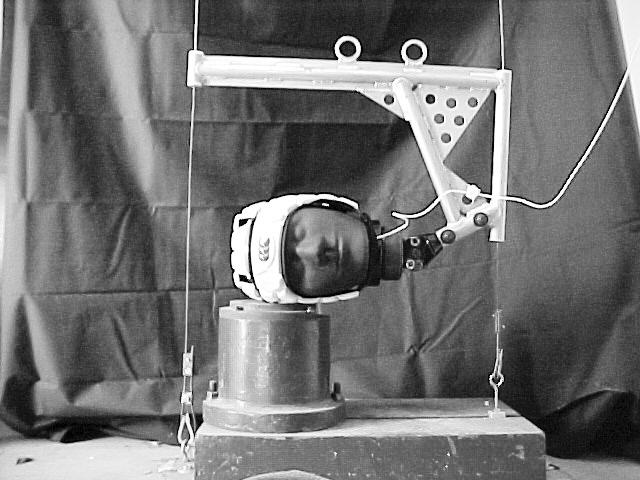
Impact at the parietal-lateral site.
Data Analysis
The Severity Index Computer Series recorded data on peak g and GSI. We entered the data into the Statistical Package for Social Sciences (version 11.0; SPSS Inc, Chicago, IL). Descriptive statistics were calculated for all categoric variables. The interaction between impact site and headgear type was not of primary interest. Therefore, we chose a research design that allowed headgear to be analyzed, controlling for site, and site to be analyzed, controlling for headgear type. The research design was 4 one-way, within-subjects, repeated-measures analyses of variance (ANOVAs) with alpha = .05.
RESULTS
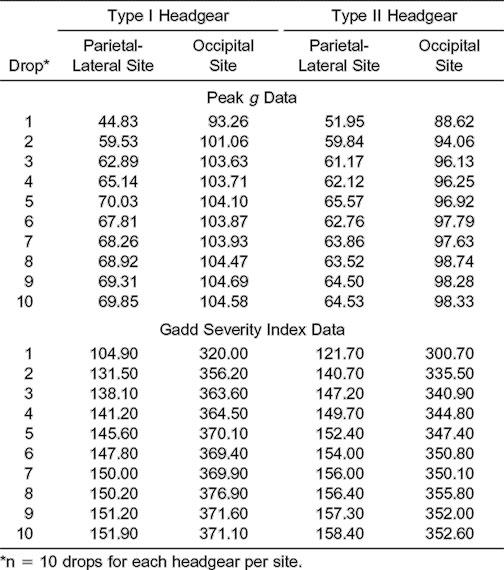
Peak g served as the dependent variable for two 2 (type) × 10 (drops) ANOVAs with repeated measures and two 2 (site) × 10 (drops) ANOVAs with repeated measures (Table 1). The drops were the within-subjects measure, and type and site were the between-subjects measures. All results are presented in peak g to allow for comparison with previous research examining rugby headgear using the IRB protocol (Table 2).
Table 1.
Gadd Severity Index Results
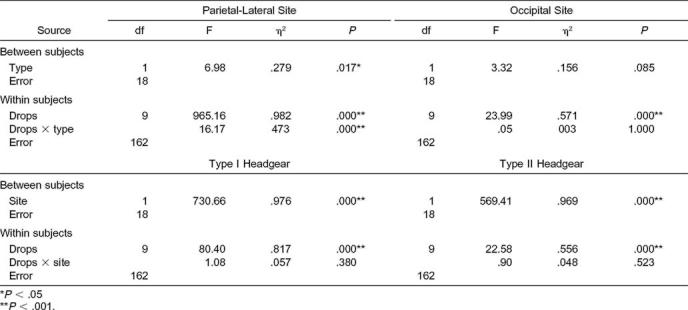
Table 2.
Mean g and Gadd Severity Index Values For Each Drop
Headgear Type Results
The linear combination of dependent variables was affected by helmet type for the parietal-lateral site (F1,18 = 4.51, P < .05) and for the occipital site (F1,18 = 6.14, P < .05). The results reflected a moderate association between helmet type and the combined dependent variables at each impact site, with partial η2 = .20 and .25, respectively. Helmet type II recorded significantly lower peak g recordings at both impact sites (Figures 5 and 6). For both analyses, the within-subjects main effect was significant (F9,162 = 48.61, P < .001, η2 = .73 and F9,162 = 64.36, P < .001, η2 = .78). Results of the GSI further supported a difference between headgear types for the parietal-lateral site but not for the occipital site (see Table 1).
Figure 5.

Mean peak g for headgear type I at the parietal-lateral (P-L) and occipital (OCC) sites.
Figure 6.

Mean peak g for headgear type II at the parietal-lateral (P-L) and occipital (OCC) site.
Impact-Site Results
The linear combination of dependent variables was also affected by impact site for headgear types I (F1,18 = 324.43, P < .001) and II (F1,18 = 280.25, P < .001). A strong association was noted between impact site and the combined dependent variables of each headgear type, with partial η2 = .95 and .94, respectively. Significantly higher peak g values were recorded at the occipital impact site for both headgear (Figures 7 and 8). For both analyses, the within-subjects main effect was significant (F9,162 = 67.13, P < .001, η2 = .79 and F9,162 = 31.28, P < .001, η2 = .64). The GSI results further supported impact-site differences (see Table 1).
Figure 7.

Mean peak g for headgear types I and II at the parietal-lateral site.
Figure 8.

Mean peak g for headgear types I and II at the occipital site.
Percentage Differences
The overall means of the first drops for each headgear were compared with impacts to the headform without headgear in GSI. For the parietal-lateral site, type I and type II headgear demonstrated significant, 269% and 219% increases, respectively, in attenuation ability (F2,27 = 10429.49, P < .001, η2 = .99). For the occipital site, type I and type II headgear produced 52% and 63% increases, respectively, in attenuation ability (F2,27 = 65.97, P < .001, η2 = .83) (Figure 9).
Figure 9.

Mean Gadd Severity Index values among headgear conditions for the first drop at the 2 sites.
DISCUSSION
Rugby headgear attenuate linear impact forces at a drop height of 30 cm. Impact testing did not result in any measure exceeding the IRB standard of 550g. However, all of the measures were less than the IRB minimum standard of 200g. The peak g and GSI measures were below the threshold criterion established by the IRB and NOCSAE to result in a high probability of a head injury. These standards are limited to no less than 200g and not exceeding 550g (IRB) and 1200 GSI (NOCSAE).12,17 According to the IRB (unpublished data, June 2003), the reason for the lower limit (200g) is because headgear that perform under this threshold could cause players to use their heads more, risking cervical spine injury. The upper limit (550g) is the result of history, and the IRB is currently investigating the possibility of its removal.
Our highest peak g recording of any drop was only 115.7g, which was on the occipital impact site. Our highest GSI recording of any test drop was 419.0 GSI, also on the occipital impact site. One possible explanation for these results is the low drop height (30 cm) recommended by the IRB. This drop height does not accurately represent the closing speed of impacts produced in game situations. The impact velocity at 30 cm is 2.4 m/s. At normal closing speeds, impacts occur at a mean of 7 m/s and as high as 13.8 m/s during a typical game of rugby.3 A second explanation of the low recordings could be the use of a Hybrid III headform. This headform was chosen because of its ability to closely mimic the human head's response to impact. This headform, according to McIntosh and McCrory,12 results in lower peak g and GSI measures when compared with the standard rigid headform used by the IRB for impact testing.
Our results concerning repetitive impacts are consistent with previous research.12,31 McIntosh and McCrory12 found that impact attenuation of rugby headgear decreased over time, thus decreasing its effectiveness in protecting against head injury. However, their study consisted of only 5 drops, with an extended period of time between impacts. They attributed the decrease in attenuation with repetitive impacts to a foam “memory effect” and postulated that, with repetitive impacts, the foam does not return to its original thickness after deformation caused by impact.12 This is an important hypothesis because rugby is a game in which impacts between players and the playing surface occur throughout the game. Additionally, rugby headgear are often worn for an entire season and even for consecutive seasons. Therefore, prolonged use raises questions regarding the effectiveness of the headgear over time.
Differences between headgear types were significant. At the parietal-lateral impact site, headgear type II attenuated more impact forces overall than type I. However, headgear type I attenuated more impact forces at drop 1 for this impact site. At the occipital site, headgear type II produced lower peak g recordings than type II for drops 1 through 10. This difference may be attributed to the design differences between the models. Headgear type I is constructed of closed-cell polyethylene foam of individualized hexagonal and pentagonal sections rather than the larger continuous sections of Triflex foam padding that constitute type II. We postulate that the continuous padding of type II may allow forces to be dispersed more effectively upon impact.
Differences between the impact sites were significant. The occipital impact site demonstrated higher peak g and GSI in comparison with the parietal-lateral impact site. This finding is consistent with our expectations and is an important finding because posterior impacts with the playing surface are common, often resulting in concussion.3 Our results indicated that the posterior lace-up design of the headgear may not provide adequate protection for the occipital region. In addition, IRB standards do not include the occipital region as a required zone of coverage. The IRB mandates that padding in the occipital region not exceed 0.5 cm but requires a thickness of 1 cm for all other zones of coverage.17 The headgear was open between 1.7 cm and 2.0 cm when laced up properly, depending on the model. Our results support the need to modify the design of headgear to improve protection in the occipital region.
CONCLUSIONS
Rugby is a rapidly growing sport in the United States. Currently, 1656 rugby clubs with more than 52 000 participants are registered with the national governing body of the United States, USA Rugby. These clubs include men's and women's youth, collegiate, and club-level teams.32 Rugby is a collision sport with an associated high risk of injury, comparable with football. The combination of these factors may mean that more certified athletic trainers will provide medical coverage for rugby as it gains popularity. Athletic trainers play an important role in the prevention of injuries in athletes. Our results indicate that athletic trainers working with rugby players should educate themselves and their athletes concerning the effectiveness and purposes of protective headgear used in rugby.
This study represented a first attempt to incorporate the recommended IRB drop height with NOCSAE protocol. Future investigations should address impacts from a greater drop height and continue to use the Hybrid III headform. These procedures may allow researchers to better mimic collisions experienced during actual rugby play and the human head's response to impact accelerations.19,20 Continued research needs to be conducted to examine the efficacy of rugby headgear.
REFERENCES
- 1.Kelly JP. Concussion in sports and recreation. Semin Neurol. 2000;20:165–171. doi: 10.1055/s-2000-9835. [DOI] [PubMed] [Google Scholar]
- 2.Powell JW. Cerebral concussion: causes, effects, and risks in sports. J Athl Train. 2001;36:307–311. [PMC free article] [PubMed] [Google Scholar]
- 3.McIntosh AS, McCrory P, Comerford J. The dynamics of concussive head impacts in rugby and Australian rules football. Med Sci Sports Exerc. 2000;32:1980–1984. doi: 10.1097/00005768-200012000-00002. [DOI] [PubMed] [Google Scholar]
- 4.Gabbett TJ. Incidence, site, and nature of injuries in amateur rugby league over three consecutive seasons. Br J Sports Med. 2000;34:98–103. doi: 10.1136/bjsm.34.2.98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bird YN, Waller AE, Marshall SW, Alsop JC, Chalmers DJ, Gerrard DF. The New Zealand Rugby Injury and Performance Project, V: epidemiology of a season of rugby injury. Br J Sports Med. 1998;32:319–325. doi: 10.1136/bjsm.32.4.319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Wekesa M, Asembo JM, Njororai WWS. Injury surveillance in a rugby tournament. Br J Sports Med. 1996;30:61–63. doi: 10.1136/bjsm.30.1.61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Gissane C, Jennings DC, Cumine AJ, Stephenson SE, White JA. Differences in the incidence of injury between rugby league forwards and backs. Aust J Sci Med Sports. 1997;29:91–94. [PubMed] [Google Scholar]
- 8.Gerrard DF, Waller AE, Bird YN. The New Zealand Rugby Injury and Performance Project, II: previous injury experience of a rugby-playing cohort. Br J Sports Med. 1994;28:229–233. doi: 10.1136/bjsm.28.4.229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Phillips LH, Standen PJ, Batt ME. Effects of seasonal change in rugby league on incidence of injury. Br J Sports Med. 1998;32:144–148. doi: 10.1136/bjsm.32.2.144. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Finch CF, McIntosh AS, McCrory P. What do under 15 year old schoolboy rugby union players think about protective headgear? Br J Sports Med. 2001;35:89–94. doi: 10.1136/bjsm.35.2.89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Marshall SW, Spencer RJ. Concussion in rugby: the hidden epidemic. J Athl Train. 2001;36:334–338. [PMC free article] [PubMed] [Google Scholar]
- 12.McIntosh AS, McCrory P. Impact energy attenuation on performance of football headgear. Br J Sports Med. 2000;34:337–341. doi: 10.1136/bjsm.34.5.337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Wilson BD. Protective headgear in rugby union. Sports Med. 1998;25:333–337. doi: 10.2165/00007256-199825050-00005. [DOI] [PubMed] [Google Scholar]
- 14.Finch C, McIntosh A, McCrory P. What is the evidence base for the use of protective headgear and mouthguards in Australian Football? Sport Health. 2000;3:35–37. [Google Scholar]
- 15.McIntosh AS, McCrory P. Effectiveness of headgear in a pilot study of under 15 rugby union football. Br J Sports Med. 2001;35:167–169. doi: 10.1136/bjsm.35.3.167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bellevue, WA: Canterbury of New Zealand; 2001. Hardgear [package insert] [Google Scholar]
- 17.Standard Performance Specification for Specific Items of Players' Clothing. Dublin, Ireland: International Rugby Board; 1998. IRB Law 4M-98g. [Google Scholar]
- 18.Football Helmet Standards for Newly Manufactured and Recertified Helmets. Overland Park, KS: National Operating Committee on Standards of Athletic Equipment; 1998. Standard drop test method and equipment used in evaluating the performance characteristics of protective headgear; pp. 1–18. NOCSAE 001-98. [Google Scholar]
- 19.Hodgson VR. Impact standards for protective equipment. In: Torg J, editor. Athletic Injuries to the Head, Neck, and Face. 2nd ed. Baltimore, MD: Mosby; 1991. pp. 28–41. [Google Scholar]
- 20.Calvano NJ, Berger RE. Effects of selected test variables on the evaluation of football helmet performance. Med Sci Sports. 1979;11:293–301. [PubMed] [Google Scholar]
- 21.Bishop PJ, Norman RW, Kozey JW. An evaluation of football helmets under impact conditions. Am J Sports Med. 1984;12:233–236. doi: 10.1177/036354658401200313. [DOI] [PubMed] [Google Scholar]
- 22.Football Helmet Standards for Recertified Helmets. Overland Park, KS: National Operating Committee on Standards for Athletic Equipment; 1996. Standard performance specification for recertified football helmets; pp. 1–2. NOCSAE 004-96. [Google Scholar]
- 23.Football Helmet Standards for Newly Manufactured and Recertified Helmets. Overland Park, KS: National Operating Committee on Standards for Athletic Equipment; 1996. Standard performance specification for newly manufactured football helmets; pp. 3–6. NOCSAE 002-96. [Google Scholar]
- 24.Football Helmet Standards for Newly Manufactured and Recertified Helmets. Overland Park, KS: National Operating Committee on Standards for Athletic Equipment; 1996. Standard performance specification for recertified football helmets; pp. 1–2. NOCSAE 004-96. [Google Scholar]
- 25.Football Helmet Standards for Recertified Helmets. Overland Park, KS: National Operating Committee on Standards for Athletic Equipment; 1996. Standard drop test method and equipment used in evaluationg the performance characteristics of protective headgear; pp. 1–19. NOCSAE 001-96. [Google Scholar]
- 26.Football Helmet Standards for Newly Manufactured and Recertified Helmets. Overland Park, KS: National Operating Committee for Standards of Athletic Equipment; 1997. Troubleshooting guide for testing equipment and impact testing; pp. 1–5. NOSCAE 100-96. [Google Scholar]
- 27.Football Helmet Standards for Newly and Recertified Helmets. Overland Park, KS: National Operating Committee for Standards of Athletic Equipment; 1998. Equipment calibration procedures; pp. 1–9. NOSCAE 101-96. [Google Scholar]
- 28.Football Helmet Standards for Newly Manufactured And Recertified Helmets. Overland Park, KS: National Operating Committee on Standards for Athletic Equipment; 1996. Laboratory procedural guide for certifying newly manufactured football helmets; pp. 2–4. NOCSAE 003-96. [Google Scholar]
- 29.Football Helmet Standards for Recertified Helmets. Overland Park, KS: National Operating Committee on Standards for Athletic Equipment; 1996. Laboratory procedural guide for recertifying football helmets; pp. 1–3. NOCSAE 005-96. [Google Scholar]
- 30.Gennarelli TA, Thibault LE, Ommaya AK. Pathophysiologic responses to rotational and translational accelerations of the head. In: Backaitis SH, editor. Biomechanics of Impact Injury and Injury Tolerances of the Neck Complex. Warrendale, PA: Society of Automotive Engineers Inc; 1993. pp. 411–423. [Google Scholar]
- 31.Caswell SV, Deivert RG. Lacrosse helmet designs and the effects of impact forces. J Athl Train. 2002;37:164–171. [PMC free article] [PubMed] [Google Scholar]
- 32.USA Rugby. USA Rugby all clubs membership page. Available at: http://www.usarugby.org/membership/php/usacippprocess.php?usacippvar=All+USA&usachoice=usacomply. Accessed December 9, 2002.