

Abstract
Cement extrusion into the pelvis with subsequent palsy of the obturator and femoral nerves is a rare entity after hip replacement surgery. Cemented fixation of the acetabular cup has been considered as a safe and reliable standard procedure with very good long term results. We present a case of fifty year old female patient after hip arthroplasty procedure which suffered an obturator and femoral nerve palsy caused by extrusion of bone cement into the pelvis. Postoperative X-rays and CT-scan of the pelvis demonstrated a huge mass consisted of bone cement in close proximity of femoral and obturator nerves. The surgery charts reported shallow and weak bony substance in postero-superior aspect of the acetabulum. This weak bony acetabular substance may have caused extrusion of bone cement during press-fitting of the polyethylene cup into the acetabulum, and the following damage of the both nerves produced by polymerization of bone cement. The bone cement fragment has been surgically removed 3 weeks after arthroplasty. The female patient underwent intensive postoperative physical therapy and electro stimulation which resulted in full recovery of the patient to daily routine and almost normal electromyography results.
Key words: arthroplasty, femoral nerve palsy, cement extrusion.
Introduction
Sacral plexus, femoral and obturator nerves are very well protected by surrounding structures; pelvic bone and muscles. The overall incidence of neurologic complications related to hip arthroplasty ranges between 0.6–2.2%.1,2 These complications occur mostly after hip replacement procedures in patients with pre-existing acetabular defects; hip dysplasia or previous hip replacement.3,4 The typical mechanism of the injury includes prosthetic device displacement, hematoma, lengthening of the leg, and iatrogenic partial transaction of the nerves.5–7 Cement extrusion during implantation of the prosthetic device into the acetabulum thought acetabular bony defects should be avoided. In many cases, the extrusion of the bone cement is not evident until postoperative x-rays are taken. Many patients after hip replacement with extruded bone cement into pelvis does not report any complaint and most surgeons accept this situation.8 But in some cases the extruded bone cement during polymerization can cause heat related damages of the neighboring nerves.9
Case Report
A 50-year-old female has been admitted to our department with weakness of the right psoas muscle and numbness of the medial aspect of the right thigh after a hip replacement surgery in October 2009. The patient had the surgery performed for degenerative joint disease. The surgeon used the standard anterolateral approach (Watson Jones). The acetabulum was packed with one mix (20 g) of Palacos cement and pressurized by hand then followed the insertion of the Pinnacle® Acetabular Cup (DePuy Orthopaedics). After Total hip arthroplasty (THA) she complained of the pain in the right groin and she had some problems to stabilize her hip during walking. The performed postoperative X-rays showed well-positioned components with cement mass extruding from right acetabulum into pelvis (Figure 1). The orthopedic surgeon decided to proceed with physical rehabilitation. Six month after surgery, the patient presented in our outpatient clinic for a follow-up. She complained of persistent pain in her right groin and weakness of the right hip flexors (Medical Research Council grade 3 out of 5) and adductor muscles (Medical Research Council 4 out of 5) with decreased sensation of the right medial thigh. Performed X-rays showed no evidence of implant loosening. Clinical examination showed atrophy of the quadriceps and adductor muscles. We performed the electromyography (EMG) which demonstrated decreased activity of the psoas major muscle and adductor muscle group. Nerve conduction velocity demonstrated decreased activity of the femoral and obturator nerves. The patient has been admitted to our department for surgical removal of the cement mass. Prior to surgery has been performed a CT-guided injection of the tissue around the cement mass with bupivacaine and triamcinolone. The diagnostic injection decreased immediately the patient's pain. This confirmed our primary suspicion that the cement was the source of the pain and atrophy of the flexor and adductor muscle groups. CT scans revealed atrophy of the adductor muscle and the cement mass lying in the superior aspect of the obturator foramen (Figure 2a and b). Three days after CT- injection we performed removal of the extruded cement mass using ilioinguinal approach. The cement mass has been removed with care from superior border of the obturator foramen (Figure 3). Postoperatively, patient's pain resolved complitelly. Moreover, 4 weeks after surgery, patient's sensation and muscle strength of the adductor and flexor group significantly improved and the patient was transferred to physical therapy department for further intensive rehabilitation.
Figure 1.

Postoperative anteroposterior X-ray demonstrates cement extrusion after total hip arthroplasty into the pelvis.
Figure 2.
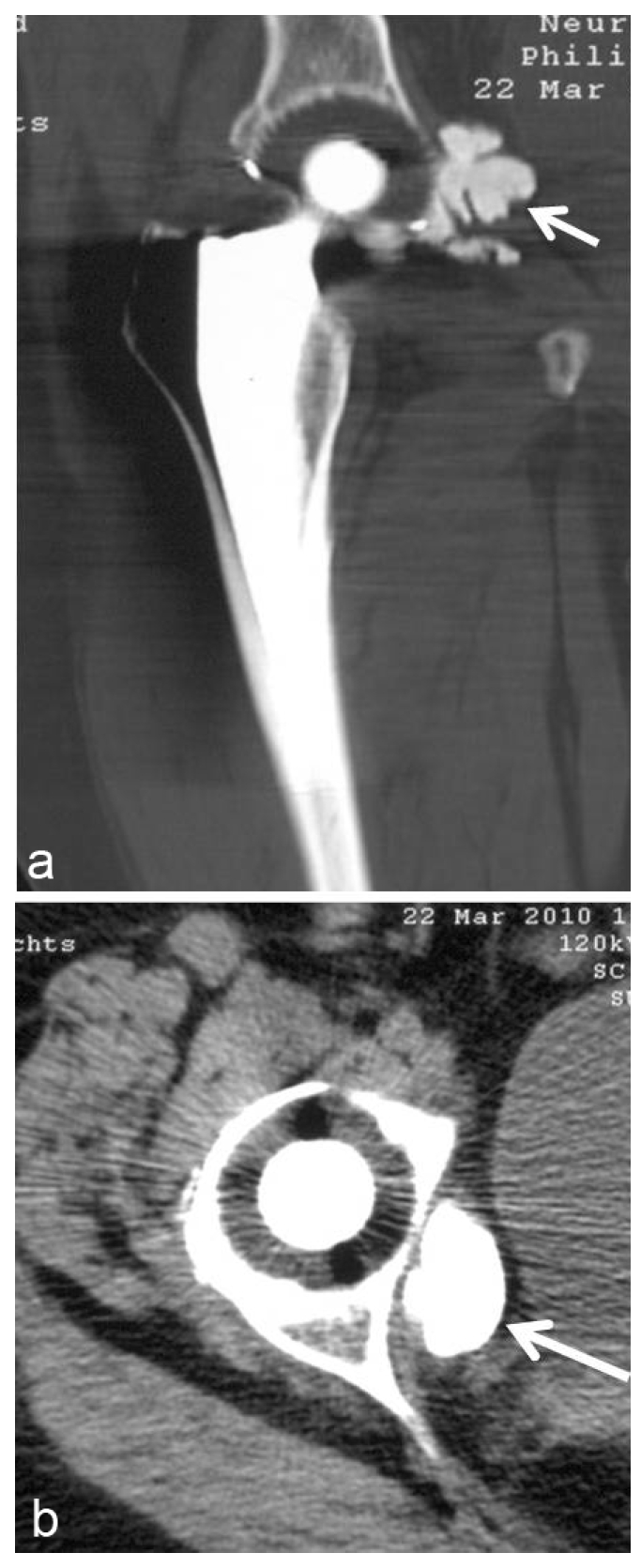
(a and b) Computed tomographic scans show the cement fragment in anteroinferior aspect of the right acetabulum.
Figure 3.

Postoperative X-ray taken after removal of the cement fragment.
Discussion
Cement extrusion after total hip arthroplasty (THA) is a common complication.10,11 However, many patients with extruded bone cement are asymptomatic.5 In addition, there is no clinical data demonstrating the correlation between volume of the cement mass, location in the pelvis and complications rate. It is of great importance to take intraoperative x-rays to avoid some cement spilling for example through transverse acetabular ligament.8,12 In addition, after reaming of the acetabulum for implantation of the acetabular cup, it is important to directly visualize the bony structure of the acetabulum and consider bone grafting of the acetabulum.13 In any patient with documented extrusion of cement, we recommend clinical evaluation, neurological exam with some imaging (i.e., CT-Scan). Patients with pain and symptomatic neurologic deficits should be considered as candidates for diagnostic and sometimes therapeutic CT-guided injection of anesthetic and steroids into tissue surrounding the extruded cement. CT-guided injections may be an alternative treatment for patients with high preoperative risk. In symptomatic patients who experienced significantly improved pain and neurologic symptoms after CT-guided injection we recommend surgical removal of the cement. This approach allows patient early and full recovery and prevents permanent damage of the obturator and femoral nerves.
References
- 1.Oldenburg M, Muller RT. The frequency, prognosis and significance of nerve injuries in total hip arthroplasty. Int Orthop. 1997;21:1–3. doi: 10.1007/s002640050107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Siliski JM, Scott RD. Obturator-nerve palsy resulting from intrapelvic extrusion of cement during total hip replacement. Report of four cases. J Bone Joint Surg Am. 1985;67:1225–8. [PubMed] [Google Scholar]
- 3.Oleksak M, Edge AJ. Compression of the sciatic nerve by methylmethacrylate cement after total hip replacement. J Bone Joint Surg Br. 1992;74:729–30. doi: 10.1302/0301-620X.74B5.1527123. [DOI] [PubMed] [Google Scholar]
- 4.Weber ER, Daube JR, et al. Peripheral neuropathies associated with total hip arthroplasty. J Bone Joint Surg Am. 1976;58:66–9. [PubMed] [Google Scholar]
- 5.Pekkarinen J, Alho A, et al. Recovery of sciatic nerve injuries in association with total hip arthroplasty in 27 patients. J Arthroplasty. 1999;14:305–11. doi: 10.1016/s0883-5403(99)90056-6. [DOI] [PubMed] [Google Scholar]
- 6.Johanson NA, Pellicci PM, et al. Nerve injury in total hip arthroplasty. Clin Orthop Relat Res. 1983:214–22. [PubMed] [Google Scholar]
- 7.Knight JL, Coglon T, et al. Posterior distal cement extrusion during primary total hip arthroplasty: a cause for concern? J Arthroplasty. 1999;14:832–9. doi: 10.1016/s0883-5403(99)90034-7. [DOI] [PubMed] [Google Scholar]
- 8.Ahlgren SA, Elmqvist D, et al. Nerve lesions after total hip replacement. Acta Orthop Scand. 1984;55:152–5. doi: 10.3109/17453678408992327. [DOI] [PubMed] [Google Scholar]
- 9.Schmalzried TP, Amstutz HC, et al. Nerve palsy associated with total hip replacement. Risk factors and prognosis. J Bone Joint Surg Am. 1991;73:1074–80. [PubMed] [Google Scholar]
- 10.Unwin A, Scott J. Nerve palsy after hip replacement: medico-legal implications. Int Orthop. 1999;23:133–7. doi: 10.1007/s002640050329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Melamed NB, Satya-Murti S. Obturator neuropathy after total hip replacement. Ann Neurol. 1983;13:578–9. doi: 10.1002/ana.410130519. [DOI] [PubMed] [Google Scholar]
- 12.Pecina M, Lucijanic I, et al. Surgical treatment of obturator nerve palsy resulting from extrapelvic extrusion of cement during total hip arthroplasty. J Arthroplasty. 2001;16:515–7. doi: 10.1054/arth.2001.22395. [DOI] [PubMed] [Google Scholar]
- 13.Fabre T, Bernez J, et al. Complete femoral nerve division at total hip arthroplasty. J Bone Joint Surg Br. 1996;78:148–9. [PubMed] [Google Scholar]