

Abstract
Inflammatory breast cancer is a rare but highly aggressive form of locally advanced breast cancer. Historically, this disease was uniformly fatal; however, with the advent of induction chemotherapy and carefully coordinated multimodality treatment, the prognosis of these patients has improved. This article reviews the clinical characteristics of inflammatory breast cancer and the recent advances in therapy.
Keywords: breast cancer, inflammatory, locally advanced
Introduction
Inflammatory breast cancer is a rare but aggressive subtype of breast cancer, which historically was considered uniformly fatal. Treatment with local therapy, with surgery, with radiation therapy, or with both resulted in few long-term survivors. However, the advent of combined modality therapy has resulted in a marked improvement in prognosis. With current therapy, approximately one-third of women diagnosed with inflammatory breast cancer will become long-term survivors. This article reviews the clinical characteristics of inflammatory carcinoma of the breast and the clinical progress that has been made in the treatment of this disease.
Inflammatory breast cancer accounts for about 5% of all cases of breast cancer [1]. In general, women with inflammatory breast cancer present at a younger age, are more likely to have metastatic disease at diagnosis, and have shorter survival than women with non-inflammatory breast cancer [1]. According to the latest revision of the American Joint Committee on Cancer staging guidelines, inflammatory carcinoma is classified at T4d, which makes all patients with inflammatory carcinoma stage IIIB, IIIC, or IV depending on the nodal status and presence of distant metastases [2].
Clinical and pathological characteristics
Clinically, inflammatory breast cancer is characterized by the rapid onset of breast warmth, erythema, and edema (peau d'orange) often without a well-defined mass. Along with extensive breast involvement, women with inflammatory carcinoma often have early involvement of the axillary lymph nodes. Taylor and Meltzer provided a classic description of inflammatory breast cancer in their 1938 paper: "The redness, which may vary from a faint blush to a flaming red, spreads diffusely over the breast, which becomes hot, pitted, and edematous, presenting an 'orange-skin' appearance. Meanwhile the cancer spreads rapidly throughout the entire breast in the form of a diffuse ill-defined induration. The breast may swell to two or three times its original volume within a few weeks" [3]. The rapidity of growth can be used to distinguish true 'primary' inflammatory carcinoma from neglected locally advanced breast tumors that have developed inflammatory features ('secondary' inflammatory carcinomas) [3]. The mammographic appearance of inflammatory breast cancer differs from other breast tumors because less than half will show a discrete mass [4,5]. However, other abnormal findings such as skin thickening, trabecular thickening, and axillary adenopathy are present in the majority of patients [5]. Figure 1 shows the typical clinical and radiographic appearance of inflammatory breast carcinoma.
Figure 1.
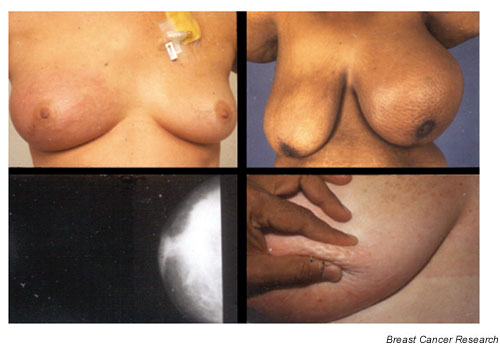
Inflammatory breast cancer.
Inflammatory breast carcinoma is not associated with a particular histologic subtype and can occur in association with infiltrating ductal or lobular, small cell, medullary, and large cell carcinomas [6]. The characteristic pathologic finding is dermal lymphatic invasion by carcinoma, which can lead to obstruction of the lymphatic drainage causing the clinical picture of erythema and edema. However, the diagnosis of inflammatory carcinoma is made on clinical grounds, and the absence of dermal lymphatic invasion does not exclude the diagnosis. Patients with the clinical features of inflammatory carcinoma should be treated aggressively even if they do not have pathologic evidence of dermal lymphatic invasion.
The most significant prognostic factor for women with inflammatory breast cancer is the presence of lymph node involvement. Patients with lymph node involvement have shorter disease-free and overall survival than patients with node-negative disease [7,8]. Extensive erythema, the absence of estrogen receptor, and the presence of mutations in the p53 gene have also been associated with poorer outcomes in patients with inflammatory carcinoma of the breast [7-9]. Because most women with inflammatory carcinoma do not have discrete masses, tumor size does not have the same prognostic value as in women with non-inflammatory carcinoma.
Inflammatory carcinoma of the breast has distinct biological characteristics that differentiate it from non-inflammatory carcinoma. These tumors more often have a high S-phase fraction, are high-grade, are aneuploid, and lack hormone receptor expression [6,10,11]. Paradiso and colleagues found that 44% of inflammatory breast cancers were estrogen-receptor-positive and 30% were progesterone-receptor-positive compared with 64% and 51%, respectively, in patients with locally advanced, non-inflammatory breast cancer [10]. In addition, inflammatory carcinomas are more likely to have mutations in p53. In a study of prognostic markers in inflammatory breast cancer, Aziz and colleagues compared 40 cases of inflammatory breast cancer with 80 controls matched by patient age and tumor grade, and showed that inflammatory breast cancers were more likely to overexpress p53 (69% versus 48%) [11]. The normal function of p53 can be altered by two distinct mechanisms in inflammatory breast cancer: direct mutation (30%) or by cytoplasmic sequestration of the protein (37%) [12]. The data regarding the role of c-erbB-2 overexpression in inflammatory breast cancer have been more variable, but most studies have found no difference in the rates of c-erbB-2 overexpression between inflammatory and non-inflammatory carcinomas of the breast [11,13]. Similarly, no difference has been seen in the frequency of expression of EGFR and cathepsin D between inflammatory and non-inflammatory cancers [11].
In addition to having different rates of expression of many standard prognostic markers, inflammatory breast cancers can also be differentiated by their highly angiogenic and vascular characteristics. In a study of 67 tumor specimens, McCarthy and colleagues reported that inflammatory breast cancers have significantly higher microvessel density [14]. Merajver and colleagues have found that inflammatory carcinoma cells are more likely to have high levels of vascular endothelial growth factor (VEGF) and basic fibroblast growth factor (bFGF) [15]. The authors propose that the high levels of members of the VEGF family might account for tumor neovascularization and the lymphotactic process in inflammatory breast cancer. Inflammatory breast cancers might also be more likely to express E-cadherin, a trans-membrane glycoprotein that mediates cell-cell adhesion, and may contribute to the aggressive lymphovascular invasion seen in inflammatory cancers [16]. Kleer and colleagues reported that 100% (20 of 20) inflammatory carcinomas expressed E-cadherin, compared with 68% (15 of 22) of non-inflammatory breast tumors [17]. Alpaugh and colleagues developed a human xenograft model of inflammatory breast cancer (MARY-X), and the investigators detected a 10–20-fold overexpression of E-cadherin in the xenograft [18]. Another human inflammatory breast cancer xenograft (WIBC-9) was developed by Shirakawa and colleagues [19]. This xenograft showed overexpression of angiogenic factors, including VEGF, bFGF, and Flt-1, which could be potential therapeutic targets [19].
Several genes have been identified that might contribute to the aggressive clinical behavior of inflammatory breast cancer. Van Golen and colleagues reported that the overexpression of RhoC GTPase and the loss of expression of LIBC (lost in inflammatory breast cancer) were highly correlated with an inflammatory carcinoma phenotype [20]. LIBC, a novel gene, was lost in 80% of inflammatory specimens in comparison with 21% of noninflammatory tumors. RhoC GTPase, a gene involved in cytoskeletal reorganization, was overexpressed in 90% of inflammatory tumors in comparison with 38% of non-inflammatory cancers. Furthermore, when a stable RhoC transfectant cell line was created, RhoC behaved as a transforming oncogene conferring a highly invasive phenotype similar to that seen in inflammatory breast cancer [21]. These genes remain a promising avenue for future investigation.
Therapy
Historically, patients with inflammatory breast carcinoma who were treated with surgery alone have had very poor outcomes, and most surgeons have considered the diagnosis a contraindication to surgery. Similarly, local therapy with radiation or with a combination of radiation and surgery resulted in virtually no long-term survivors [6]. However, the development of active chemotherapy regimens, used in combination with local therapy, has resulted in a marked improvement in prognosis for patients with this aggressive form of breast cancer. Our first report demonstrated that two-thirds of patients with inflammatory breast cancer responded to induction FAC (5-fluorouracil, doxoru-bicin, and cyclophosphamide), and 50% and 31% of those treated with FAC, radiotherapy, and then adjuvant chemotherapy remained relapse-free 2 and 5 years after diagnosis, respectively [22]. Most series have reported that at least one-third of patients treated with combined modality therapy are alive at 5 years [6].
An update of experience at the MD Anderson Cancer Center with inflammatory breast cancer over the past 20 years was published by Ueno and colleagues [4]. A total of 178 patients were treated with combined modality therapy, which consisted of doxorubicin-based induction chemotherapy, local therapy with radiotherapy with or without mastectomy, and adjuvant chemotherapy. In this series, 28% of patients were alive and without evidence of disease beyond 15 years. Overall survival was 40% at 5 years and 33% at 10 years, with a median survival of 37 months. Other large series of patients with inflammatory breast cancer treated with combined modality therapy have reported similar survival rates, demonstrating the change in natural history of inflammatory breast cancer since the advent of induction chemotherapy [23,24].
The treatment of inflammatory breast cancer requires careful coordination of care between the medical, surgical, and radiation oncologists because most patients will be treated with a combination of these therapeutic modalities. The initial component of therapy should be induction chemotherapy (Fig. 2). Many different regimens have been used, most of which are anthracycline-based. Ueno and colleagues found that 71% of all patients had a response to anthracycline-based induction chemotherapy, with 12% of patients achieving a complete response [4]. In addition, initial response to induction chemotherapy was an important predictor of survival; disease-free survival at 15 years was 44% in patients who had a complete response to induction chemotherapy, 31% in those who had a partial response, and 7% in patients who did not respond to therapy. A study from the Centre H Becquerel showed that dose-intense therapy resulted in higher response rates, but these high response rates did not translate into improved survival [25].
Figure 2.
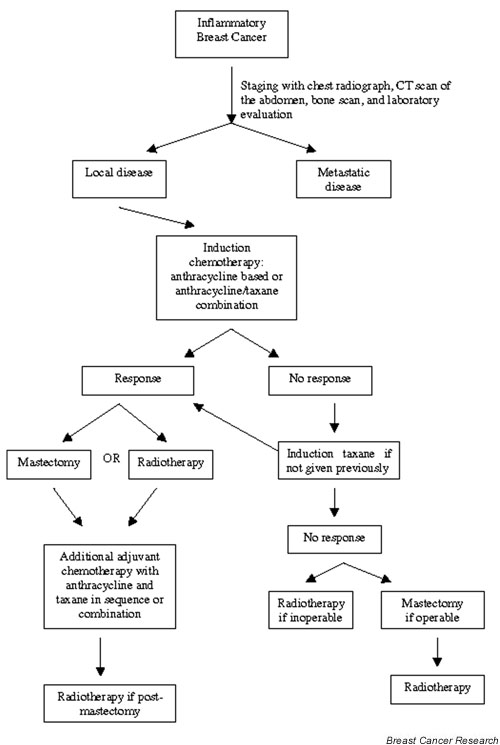
Treatment algorithm for inflammatory breast cancer.
After induction chemotherapy, patients should proceed with definitive local therapy with radiation, surgery, or both. Considerable controversy still exists as to the optimal local treatment. This disease was traditionally considered inoperable because of the uniformly poor prognosis; however, survival has improved with the use of chemotherapy, and the role of surgery has been reexamined. Unfortunately, many of the studies that have examined the role of mastectomy after induction chemotherapy have been difficult to interpret because patients who have more limited disease and those who have responses to therapy have been more likely to have mastectomies. In addition, the rarity of this disease precludes large randomized trials. The data regarding mastectomy in inflammatory breast cancer are conflicting: several trials have shown a benefit [26,27] but others suggest that mastectomy offers no survival advantage [28,29]. Fleming and colleagues reviewed the experience with mastectomy in 178 patients treated at the MD Anderson Cancer Center [26]. The authors found that patients who had a response to induction chemotherapy benefited from the addition of mastectomy to chemotherapy and radiation. These patients had significantly lower rates of local recurrence and improved disease-specific survival than patients who responded to induction chemotherapy but did not undergo mastectomy.
A study by Curcio and colleagues of 90 patients with inflammatory breast cancer reported a striking increase in overall survival and decrease in local recurrence in patients who had a mastectomy and were able to achieve negative surgical margins [27]. This report suggests that if negative surgical margins are obtainable, mastectomy could be of benefit in patients with inflammatory breast carcinoma. However, other studies have found survival to be similar in patients who underwent mastectomy with adjuvant radiation and in those who had radiation alone [28,29]. Because the existing published data are conflicting, radiation alone and mastectomy followed by radiation remain reasonable treatment alternatives for local therapy.
For patients who are treated with mastectomy, the data suggest that sentinel lymphadenectomy (SL) is not reliable in predicting axillary staging. Stearns and colleagues reported on the accuracy of sentinel lymph node biopsy after neoadjuvant chemotherapy in a cohort that included eight patients with inflammatory breast cancer [30]. Of the eight patients with inflammatory breast cancer, three had positive nodes on both axillary lymph node dissection (ALND) and SL, one had negative nodes on both ALND and SL, two had positive nodes on ALND that were missed by SL, and two patients had non-identifiable sentinel nodes. This study suggests that patients with inflammatory carcinoma who are being treated with mastectomy should have standard ALND and not SL. However, the limited experience with this diagnostic approach indicates that additional evaluation is required.
Even after induction chemotherapy and local therapy, the rates of relapse remain very high. Thus, we would recommend further adjuvant chemotherapy with either an anthracycline or a taxane after local treatment. Finally, patients with estrogen or progesterone receptor-positive tumours should receive 5 years of adjuvant hormonal therapy with either tamoxifen or anastrazole. The role of high-dose chemotherapy followed by autologous stem cell transplantation remains experimental. Some studies have shown encouraging results, but the patient populations were highly selected and further trials are clearly needed before transplantation can be recommended outside the context of a clinical trial.
Conclusion
Despite the significant progress that has been made in the treatment of this aggressive form of breast cancer, most women with inflammatory breast cancer will relapse and succumb to this disease. Clearly, further advances are needed to improve the prognoses of women with inflammatory carcinoma. Current research on the biologic characteristics of inflammatory carcinoma has made significant strides in the understanding of the aggressive behavior of this tumor, and future research will be vital in developing targeted therapies. RhoC is a promising target for therapy; recent reports have shown that farnesyl transferase inhibitors have activity in reversing the invasive phenotype of RhoC-overexpressing cell lines [31]. Other potential targets for therapy include angiogenic factors, such as VEGF, bFGF, or Flt-1, and overexpressed E-cadherin. As our knowledge of the biology of inflammatory breast cancer grows, other potential targets will emerge; these scientific discoveries must be explored through ongoing innovative clinical trials. Only through continued research will we make progress in the treatment of this deadly form of breast cancer.
Competing interests
None declared.
Note
This article is the third in a review series on Inflammatory breast cancer, edited by Sofia Merajver. Other articles in the series can be found at http://breast-cancer-research.com/articles/series.asp?rqs=merajver
Abbreviations
ALND = axillary lymph node dissection; bFGF = basic fibroblast growth factor; FAC = 5-fluorouracil, doxorubicin, and cyclophosphamide; SL = sentinel lymphadenectomy; VEGF = vascular endothelial growth factor.
References
- Levine PH, Steinhorn SC, Ries LG, Aron JL. Inflammatory breast cancer: the experience of the surveillance, epidemiology, and end results (SEER) program. J Natl Cancer Inst. 1985;74:291–297. [PubMed] [Google Scholar]
- Singletary SE, Allred C, Ashley P, Bassett LW, Berry D, Bland KI, Borgen PI, Clark G, Edge SB, Hayes DF, Hughes LL, Hutter RVP, Morrow M, Page DL, Recht A, Theriault RL, Thor A, Weaver DL, Wieand HS, Green FL. Revision of the American Joint Committee on Cancer staging system for breast cancer. J Clin Oncol. 2002;20:3628–3636. doi: 10.1200/JCO.2002.02.026. [DOI] [PubMed] [Google Scholar]
- Taylor G, Meltzer A. Inflammatory carcinoma of the breast. Am J Cancer. 1938;33:33–49. [Google Scholar]
- Ueno NT, Buzdar AU, Singletary SE, Ames FC, McNeese MD, Holmes FA, Theriault RL, Strom EA, Wasaff BJ, Asmar L, Frye D, Hortobagyi GN. Combined-modality treatment of inflammatory breast carcinoma: twenty years of experience at M. D. Anderson Cancer Center. Cancer Chemother Pharmacol. 1997;40:321–329. doi: 10.1007/s002800050664. [DOI] [PubMed] [Google Scholar]
- Kushwaha AC, Whitman GJ, Stelling CB, Cristofanilli M, Buzdar AU. Primary inflammatory carcinoma of the breast: retrospective review of mammographic findings. AJR Am J Roentgenol. 2000;174:535–538. doi: 10.2214/ajr.174.2.1740535. [DOI] [PubMed] [Google Scholar]
- Jaiyesimi IA, Buzdar AU, Hortobagyi G. Inflammatory breast cancer: a review. J Clin Oncol. 1992;10:1014–1024. doi: 10.1200/JCO.1992.10.6.1014. [DOI] [PubMed] [Google Scholar]
- Palangie T, Mosseri V, Mihura J, Campana F, Beuzeboc P, Dorval T, Garcia-Giralt E, Jouve M, Scholl S, Asselain B, Pouillart P. Prognostic factors in inflammatory breast cancer and therapeutic implications. Eur J Cancer. 1994;7:921–927. doi: 10.1016/0959-8049(94)90115-5. [DOI] [PubMed] [Google Scholar]
- Chevallier B, Asselain B, Kunlin A, Veyret C, Bastit P, Graic Y. Inflammatory breast cancer. Determination of prognostic factors by univariate and multivariate analysis. Cancer. 1987;60:897–902. doi: 10.1002/1097-0142(19870815)60:4<897::aid-cncr2820600430>3.0.co;2-s. [DOI] [PubMed] [Google Scholar]
- Riou G, Le MG, Travagli JP, Levine AJ, Moll UM. Poor prognosis of p53 gene mutation and nuclear overexpression of p53 protein in inflammatory breast carcinoma. J Natl Cancer Inst. 1993;85:1765–1767. doi: 10.1093/jnci/85.21.1765. [DOI] [PubMed] [Google Scholar]
- Paradiso A, Tommasi S, Brandi M, Marzullo F, Simone G, Lorusso V, Mangia A, De Lena M. Cell kinetics and hormonal receptor status in inflammatory breast carcinoma: comparison with locally advanced disease. Cancer. 1989;64:1922–1927. doi: 10.1002/1097-0142(19891101)64:9<1922::aid-cncr2820640927>3.0.co;2-i. [DOI] [PubMed] [Google Scholar]
- Aziz SA, Pervez S, Khan S, Kayani N, Azam SI, Rahbar MH. Case control study of prognostic markers and disease outcome in inflammatory carcinoma breast: a unique clinical experience. Breast J. 2001;7:398–404. doi: 10.1046/j.1524-4741.2001.07604.x. [DOI] [PubMed] [Google Scholar]
- Moll UM, Riou G, Levine AJ. Two distinct mechanisms alter p53 in breast cancer: mutation and nuclear exclusion. Proc Natl Acad Sci USA. 1992;89:7262–7266. doi: 10.1073/pnas.89.15.7262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Prost S, Le MG, Douc-Rasy S, Ahomadegbe JC, Spielmann M, Guerin M, Riou G. Association of c-erbB2-gene amplification with poor prognosis in non-inflammatory breast carcinomas but not in carcinomas of the inflammatory type. Int J Cancer. 1994;58:763–768. doi: 10.1002/ijc.2910580602. [DOI] [PubMed] [Google Scholar]
- McCarthy NJ, Yang X, Linnoila IR, Merino MJ, Hewitt SM, Parr AL, Paik S, Steinberg SM, Hartmann DP, Mourali N, Levine PH, Swain SM. Microvessel density, expression of estrogen receptor alpha, MIB-1, p53, and c-erbB-2 in inflammatory breast cancer. Clin Cancer Res. 2002;8:3857–3862. [PubMed] [Google Scholar]
- Kleer CG, van Golen KL, Merajver SD. Molecular biology of breast cancer metastasis. Inflammatory breast cancer: clinical syndrome and molecular determinants. Breast Cancer Res. 2000;2:423–429. doi: 10.1186/bcr89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tomlinson JS, Alpaugh ML, Barsky SH. An intact overexpressed E-cadherin/alpha,beta-catenin axis characterizes the lympho-vascular emboli of inflammatory breast carcinoma. Cancer Res. 2001;61:5231–5241. [PubMed] [Google Scholar]
- Kleer CG, van Golen KL, Braun T, Merajver SD. Persistent E-cadherin expression in inflammatory breast cancer. Mod Pathol. 2001;14:458–464. doi: 10.1038/modpathol.3880334. [DOI] [PubMed] [Google Scholar]
- Alpaugh ML, Tomlinson JS, Shao ZM, Barsky SH. A novel human xenograft model of inflammatory breast cancer. Cancer Res. 1999;59:5079–5084. [PubMed] [Google Scholar]
- Shirakawa K, Tsuda H, Heike Y, Kato K, Asada R, Inomata M, Sasaki H, Kasumi F, Yoshimoto M, Iwanaga T, Konishi F, Terada M, Wakasugi H. Absence of endothelial cells, central necrosis, and fibrosis are associated with aggressive inflammatory breast cancer. Cancer Res. 2001;61:445–451. [PubMed] [Google Scholar]
- van Golen KL, Davies S, Wu ZF, Wang Y, Bucana CD, Root H, Chandrasekharappa S, Strawderman M, Ethier SP, Merajver SD. A novel putative low-affinity insulin-like growth factor-binding protein, LIBC (lost in inflammatory breast cancer), and RhoC GTPase correlate with the inflammatory breast cancer phenotype. Clin Cancer Res. 1999;5:2511–2519. [PubMed] [Google Scholar]
- van Golen KL, Wu ZF, Qiao XT, Bao LW, Merajver SD. RhoC GTPase, a novel transforming oncogene for human mammary epithelial cells that partially recapitulates the inflammatory breast cancer phenotype. Cancer Res. 2000;60:5832–5838. [PubMed] [Google Scholar]
- Blumenschein G, Montague ED, Eckles NE, Hortobagyi G, Barker JL. Sequential combined modality therapy for inflammatory breast cancer. Breast. 1976;2:16–20. [Google Scholar]
- Rouesse J, Friedman S, Sarrazin D, Mouriesse H, Le Chevalier T, Arriagada R, Spielmann M, Papacharalambous A, May-Levin F. Primary chemotherapy in the treatment of inflammatory breast carcinoma: a study of 230 cases from the Institut Gustave-Roussy. J Clin Oncol. 1986;4:1765–1771. doi: 10.1200/JCO.1986.4.12.1765. [DOI] [PubMed] [Google Scholar]
- Fields JN, Perez CA, Kuske RR, Fineberg BB, Bartlett N. Inflammatory carcinoma of the breast: treatment results on 107 patients. Int J Radiat Oncol Biol Phys. 1989;17:249–255. doi: 10.1016/0360-3016(89)90436-7. [DOI] [PubMed] [Google Scholar]
- Chevallier B, Bastit P, Graic Y, Menard JF, Dauce JP, Julien JP, Clavier B, Kunlin A, D'Anjou J. The Centre H. Becquerel studies in inflammatory non metastatic breast cancer: combined modality approach in 178 patients. Br J Cancer. 1993;67:594–601. doi: 10.1038/bjc.1993.109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fleming RY, Asmar L, Buzdar AU, McNeese MD, Ames FC, Ross MI, Singletary SE. Effectiveness of mastectomy by response to induction chemotherapy for control in inflammatory breast carcinoma. Ann Surg Oncol. 1997;4:452–461. doi: 10.1007/BF02303668. [DOI] [PubMed] [Google Scholar]
- Curcio LD, Rupp E, Williams WL, Chu DZ, Clarke K, Odom-Maryon T, Ellenhorn JD, Somlo G, Wagman LD. Beyond palliative mastectomy in inflammatory breast cancer – a reassessment of margin status. Ann Surg Oncol. 1999;6:249–254. doi: 10.1007/s10434-999-0249-3. [DOI] [PubMed] [Google Scholar]
- Mourali N, Tabbane F, Muenz LR, Behi J, Ben Moussa F, Jaziri M, Levine PH. Ten-year results utilizing chemotherapy as primary treatment in nonmetastatic, rapidly progressing breast cancer. Cancer Invest. 1993;11:363–370. doi: 10.3109/07357909309018867. [DOI] [PubMed] [Google Scholar]
- De Boer RH, Allum WH, Ebbs SR, Gui GP, Johnston SR, Sacks NP, Walsh G, Ashley S, Smith IE. Multimodality therapy in inflammatory breast cancer: is there a place for surgery? Ann Oncol. 2000;11:1147–1153. doi: 10.1023/A:1008374931854. [DOI] [PubMed] [Google Scholar]
- Stearns V, Ewing CA, Slack R, Penannen MF, Hayes DF, Tsangaris TN. Sentinel lymphadenectomy after neoadjuvant chemotherapy for breast cancer may reliably represent the axilla except for inflammatory breast cancer. Ann Surg Oncol. 2002;9:235–242. doi: 10.1245/aso.2002.9.3.235. [DOI] [PubMed] [Google Scholar]
- van Golen KL, Bao L, DiVito MM, Wu Z, Prendergast GC, Merajver SD. Reversion of RhoC GTPase-induced inflammatory breast cancer phenotype by treatment with a farnesyl trans-ferase inhibitor. Mol Cancer Therapeut. 2002;1:575–583. [PubMed] [Google Scholar]