

Abstract
Treatment of dentin hypersensitivity with oxalates is common, but oxalate efficacy remains unclear. Our objective was to systematically review clinical trials reporting an oxalate treatment compared with no treatment or placebo with a dentin hypersensitivity outcome. Risk-of-bias assessment and data extraction were performed independently by two reviewers. Standardized mean differences (SMD) were estimated by random-effects meta-analysis. Of 677 unique citations, 12 studies with high risk-of-bias were included. The summary SMD for 3% monohydrogen-monopotassium oxalate (n = 8 studies) was -0.71 [95% Confidence Interval: -1.48, 0.06]. Other treatments, including 30% dipotassium oxalate (n = 1), 30% dipotassium oxalate plus 3% monohydrogen monopotassium oxalate (n = 3), 6% monohydrogen monopotassium oxalate (n = 1), 6.8% ferric oxalate (n = 1), and oxalate-containing resin (n = 1), also were not statistically significantly different from placebo treatments. With the possible exception of 3% monohydrogen monopotassium oxalate, available evidence currently does not support the recommendation of dentin hypersensitivity treatment with oxalates.
Keywords: dentin sensitivity, oxalates, systematic review, meta-analysis
Introduction
Dentin hypersensitivity (DH) is defined as brief, sharp pain elicited when dentin is exposed to thermal, tactile, osmotic, chemical, or evaporative stimuli (Canadian Advisory Board on Dentin Hypersensitivity, 2003). To date, analysis of most data supports a theory that these stimuli induce fluid flow within dental tubules, which triggers baroreceptors near the pulp, leading to pain (Pashley, 1994). This so-called hydrodynamic theory of pain generation assumes an exposed dentin surface and patent tubules that allow fluid flow to reach the pulp where the baroreceptors reside (Brannström et al., 1967). Up to 40 million American adults report DH symptoms each year (Addy, 1990), but reported prevalence rates range widely. Some research has placed the incidence as high as 74%, but in most populations, it appears to range between 10 and 30%, depending on the population studied, study setting, and study design (Rees and Addy, 2004).
A panoply of current diagnostic and treatment strategies for DH suggests considerable uncertainty among dental practitioners about how to manage this condition (Cunha-Cruz et al., 2010). The diagnosis of DH remains by exclusion of other dental and periodontal conditions that might cause pain (Holland et al., 1997), and no fewer than a dozen methods are currently used for diagnosis (Cunha-Cruz et al., 2010). Most contemporary treatments seek to occlude the exposed dentin with restorative materials, laser treatment, resin-based sealants, or pharmacological agents. Among the latter group, oxalates have a particularly long history of use and acceptance by practitioners. For example, a recent survey of practicing dentists suggests that 40% use oxalates to treat DH (Cunha-Cruz et al., 2010).
Oxalates were introduced as agents to treat DH in the late 1970s to mid-1980s, based on work done primarily in vitro. Several studies reported significant decreases in hydraulic conductance across dentin disks treated with oxalates, suggesting that oxalates limit fluid flow in exposed dentin in vivo, thereby reducing pain (Pashley et al., 1978, 1984; Greenhill and Pashley, 1981; Pashley and Galloway, 1985). Subsequent work showed that oxalates formed precipitates within dentin tubules that blocked dentinal fluid flow (Cuenin et al., 1991). Oxalates reportedly have the added advantage of relative insolubility in acid, making them resistant to dissolution after treatment (Pereira et al., 2005).
In spite of the compelling in vitro work supporting the use of oxalates and relatively wide acceptance by practitioners, few controlled studies have shown their efficacy clinically, and a rigorous systematic evaluation of existing studies has not been reported. Yet, controlled data on the efficacy of oxalate treatment are essential to guide both dental practice and further research in the treatment of DH. Thus, our objective was to perform a systematic review of controlled trials on humans with DH, comparing an oxalate intervention with a placebo or no-treatment group to reduce DH.
Methods
Study Selection Criteria
Participants: Humans with DH. Post-restorative hypersensitivity studies were excluded.
Intervention: Oxalates.
Comparison: Placebo or no treatment.
Outcomes: DH pain response to routine activities, thermal, tactile, evaporative, or electrical stimuli. Because of the heterogeneity of methods used to assess DH, no a priori outcome measure was required.
Studies: randomized controlled trial (RCT) or clinical controlled trial (CCT).
Search Methods to Identify Studies
After the development of a protocol, article citations were obtained through an electronic search of databases (to July 2009) and hand-searching of bibliographic reference listings of published primary and review studies (for a complete list of databases, see Appendix 1). The MEDLINE and CENTRAL search strategy included the terms “dentin sensitivity” [MeSH Term] OR “dentin hypersensitivity”. Additional electronic searches were performed by two students using the terms “dentin hypersensitivity” OR “dentin sensitivity”. The Cochrane highly sensitive search strategy for identifying randomized trials (revision 2008) (Higgins and Green, 2009) was applied to restrict studies to clinical trials in MEDLINE; no language restrictions were imposed. Reports identified through electronic searches of MEDLINE and CENTRAL were coded according to participants and interventions by two independent reviewers, and agreement was calculated with the Kappa statistic.
Study Description and Risk-of-Bias Assessment
Two reviewers independently performed study description and risk-of-bias assessments; disagreements were resolved by discussion among the two reviewers and a third reviewer. Where needed, authors of studies were contacted for additional information to resolve ambiguities, and their responses were accepted until April 20, 2010. Risk-of-bias was assessed by the Cochrane Collaboration tool (Higgins and Green, 2009) (for a detailed description, see Appendix 2).
Synthesis of Results
Three reviewers performed data extraction. The number of participants, means and standard deviations were extracted from the reports (for a detailed description, see Appendix 2). Based on random-effects models (DerSimonian and Laird, 1986), standardized weighted-mean differences (SMD), reported in units of standard deviation, were calculated for each oxalate treatment after calculation of the SMD of all outcomes for each study. For split-mouth trials, the reviewers assumed a within-patient correlation coefficient equal to 0. Heterogeneity between studies, quantified with the I2-statistic (Higgins and Thompson, 2002), was considered high if statistical heterogeneity levels were higher than 70%. Data were analyzed with RevMan 4.2.7.
Results
Study Selection
Electronic searches from all sources retrieved 677 unique citations (Fig. 1). Using titles and abstracts to screen content, we excluded 503 citations because they were not clinical studies of DH in humans, or were reviews or opinion papers. Agreement between reviewers was good (Kappa = 0.79). We pared the remaining 174 citations to 15 by evaluating full article content with information provided by correspondence with authors as needed. Four articles not previously found through electronic search were discovered in the references of citations. Of the 19 human clinical trials on oxalates, 4 did not meet the inclusion criteria, and 3 were previous reports of included studies (see Appendix 3 for list of excluded trials and reasons). The remaining 12 reports (Hansson, 1987; Cooley and Sandoval, 1989; Muzzin and Johnson, 1989; Cuenin et al., 1991; Holborow, 1994; Gillam et al., 1997, 2004; Morris et al., 1999; Pereira et al., 2001; Camps and Pashley, 2003; Pillon et al., 2004; Pamir et al., 2007) were subjected to detailed analysis (Table 1).
Figure 1.
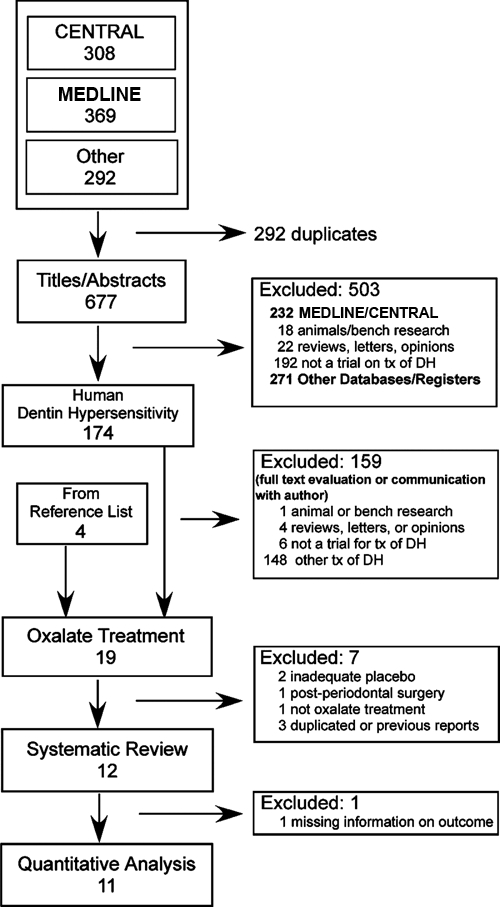
Flow-chart of the selection of studies for the systematic review of the effects of oxalates on dentin hypersensitivity.
Table 1.
Characteristics of the Studies Included in the Systematic Review of the Effects of Oxalates on Dentin Hypersensitivity
| Design | Country | Setting | N of Observations by Group | Age (yrs) | Experimental Intervention | Pain Stimuli | |
|---|---|---|---|---|---|---|---|
| Pamir et al., 2007 | RCT | Turkey | University | 15 / 15 | 18–57 | 3% monohydrogen-monopotassium oxalate gel | Thermal, evaporative |
| Gillam et al., 2004 | RCT, split-mouth | United Kingdom | University | 13 / 13 | Mean 46.2 | 6.8% ferric oxalate | Thermal, tactile, evaporative |
| Pillon et al., 2004 | RCT, split-mouth | Brazil | University | 15 / 15 | NR | 3% monohydrogen-monopotassium oxalate gel | Routine activities of eating, drinking, and tooth cleaning |
| Camps and Pashley, 2003 | RCT, split-mouth | France | University | 87 / 87 | 17–52 | 3% monohydrogen-monopotassium oxalate gel | Tactile, evaporative |
| Pereira et al., 2001 | RCT, split-mouth | Brazil | University | 23 / 21 / 24 / 14 | 21–45 | 3% monohydrogen-monopotassium oxalate gel, pH 2.5 and pH 4change/6% monohydrogen-monopotassium oxalate gel | Tactile, evaporative |
| Morris et al., 1999 | RCT, split-mouth | United States | Military | 10 / 10 | 21–43 | Oxalate-containing pre-polymerized resin solution | Tactile, evaporative |
| Gillam et al., 1997 | RCT, split-mouth | United Kingdom | University | 11 / 33 | Mean 45.1 | 3% monohydrogen-monopotassium oxalate | Thermal, tactile, evaporative |
| Holborow, 1994 | RCT, split-mouth | New Zealand | NR | 30 / 30 | NR | 3% monohydrogen-monopotassium oxalate | Thermal, tactile |
| Cuenin et al., 1991 | RCT | United States | Military | 6 / 7 | 29–68 | 3% monohydrogen-monopotassium oxalate | Evaporative |
| Cooley and Sandoval, 1989 | RCT, split-mouth | United States | University | 28 / 28 | NR | 30% dipotassium oxalate + 3% monohydrogen-monopotassium oxalate | Thermal |
| Muzzin and Johnson, 1989 | RCT, split-mouth | United States | University | 17 / 17 / 17 / 17 | 23–68 | 30% dipotassium oxalatechange/3% monohydrogen-monopotassium oxalatechange/30% dipotassium oxalate + 3% monohydrogen-monopotassium oxalate | Thermal |
| Hansson, 1987 | RCT | United States | University | 14 / 14 | 23–63 | 30% dipotassium oxalate + 3% monohydrogen-monopotassium oxalate | Thermal, routine stimuli |
RCT, randomized controlled trial; NR, not reported.
Study Description
Studies included in the systematic review were diverse (Table 1 and Appendix 4), with 5 conducted in the United States, 2 each in Brazil and the United Kingdom, and 1 each in Turkey, France, and New Zealand. Nine of the studies were conducted in university settings, 2 at military installations, and 1 study did not report a location. Four of the studies were funded by university or government grants, 3 were funded by product manufacturers, 2 were without external funding, and 3 did not report a funding source. All studies were full reports published in English between 1987 and 2007, except one that was a short communication (Holborow, 1994).
Nine of the 12 studies were split-mouth trials that took various approaches to the assessment of oxalate efficacy (Table 1 and Appendix 4). Eight of the 12 studies evaluated some form of monohydrogen-monopotassium oxalate. Other studies included ferric oxalate, di-potassium oxalate, or oxalate-containing pre-polymerized resin; 2 of the studies used combinations of monohydrogen-monopotassium and di-potassium oxalate. The placebo groups were diverse as well. Several studies used distilled water, some with dyes for blinding purposes. Two studies used the thickeners carboxymethyl cellulose or carbopol for blinding; 1 of these used a dye. Other studies used 4% glucose or 3% sodium chloride as placebo solutions. One study used no treatment, and 1 did not disclose the placebo procedure. Even more diverse were the follow-up intervals, which ranged from immediate to 1 yr; 4 wks was the most common follow-up time (5 studies).
DH pain was elicited by tactile, evaporative, or thermal stimuli (11 of 12 studies), although 2 studies used reported pain elicited by routine activities (Table 1 and Appendix 4). Eight of the 12 studies used more than one stimulator to elicit pain. DH was commonly quantified by a pain scale, with either verbal or numeric descriptors; 10 of 12 studies used at least this method to quantify DH. Other outcome measures included the force of tactile pressure or temperature of applied liquid that elicited pain. Adverse events during the studies were not observed; 2 studies did not report information about adverse events, and author follow-up was not successful.
Risk-of-Bias Assessment
Most studies reported use of random assignment of interventions. However, close scrutiny and author follow-up revealed that only 4 of the 12 studies had followed procedures to ensure random sequence generation and concealed allocation strategy (Table 2). Four studies did not report sufficient information to assess these factors. Only 5 of the 12 studies took measures to ensure blinding of participants, care providers, and assessors. Most studies reported blinding participants (10 of 12). The information published or provided via author communication was not sufficient to determine blinding in 2 studies.
Table 2.
Assessment of Risk-of-Bias of the Studies Included in the Systematic Review of the Effects of Oxalates on Dentin Hypersensitivity
| First Author, Year of
Publication |
|||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Domain | Pamir 2007 | Gillam 2004 | Pillon 2004 | Camps 2003 | Pereira 2001 | Morris 1999 | Gillam 1997 | Holborow 1994 | Cuenin 1991 | Cooley 1989 | Muzzin 1989 | Hansson 1987 | |
| Sequence generation | Assignment really random | Yes | Yes | Yes | No | No | Unclear | Unclear | Unclear | No | Unclear | Yes | No |
| Allocation concealment | Allocation concealed | Yes | Yes | Yes | No | No | Unclear | No | No | Yes | No | Yes | No |
| Blinding of participants, care providers, and outcome assessors | Patient blinded | Yes | Yes | Yes | Yes | Yes | Unclear | No | Yes | Yes | Yes | Yes | Yes |
| Care provider blinded | No | Yes | Yes | No | No | No | No | Unclear | Yes | No | Yes | Yes | |
| Outcome assessor blinded | Yes | Yes | Yes | Yes | No | No | Yes | Unclear | Yes | No | Yes | Yes | |
| Incomplete outcome data | Point estimate and measure of variability presented | Yes | Yes | Yes | Yes | No | Yes | No | No | Yes | No | Yes | Yes |
| Intention-to-treat analysis | NA | Unclear | NA | NA | No | Unclear | NA | Unclear | NA | Unclear | NA | NA | |
| Selective outcome reporting | Free of selective outcome reporting | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Unclear | Yes | Yes | Yes |
| Other sources of bias | Eligibility criteria specified | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes |
| Groups similar at baseline | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | |
| Split-mouth (crossover design) appropriate | NA | Unclear | Yes | No | Yes | No | No | No | NA | Yes | Yes | NA | |
NA, not applicable.
Other factors increased the risk-of-bias. Four studies did not report point estimates, number of observations, or variability measures (Table 2). One study had a risk-of-bias via selective reporting, and in another, selective reporting was unclear. One study did not specify eligibility criteria; another reported a non-equivalence of treatment and placebo groups at baseline. Four of the 9 split mouth studies tried to limit cross-over effects by enrolling teeth from different areas of the mouth or isolating teeth with cotton rolls or a rubber dam.
Synthesis of Results
Treatment with 3% monohydrogen-monopotassium oxalate resulted in less DH as measured by thermal stimuli, tactile stimuli, (applied force), and routine activities; the most favorable results were obtained when routine activities were used as a measure. For other outcomes, interventions with 3% monohydrogen-monopotassium oxalate produced no change or made DH worse (for results by outcome, see Appendix 2). Data were not available for 2 outcomes of one study (Gillam et al., 1997), and 1 outcome of another study (Holborow, 1994). Based on 187 and 179 units (patients or teeth) in the intervention and placebo groups from 7 studies, the summary SMD for 3% monohydrogen-monopotassium oxalate was -0.71 [95% Confidence Interval (CI): -1.48, 0.06], with high statistical heterogeneity (88%) (Fig. 2).
Figure 2.
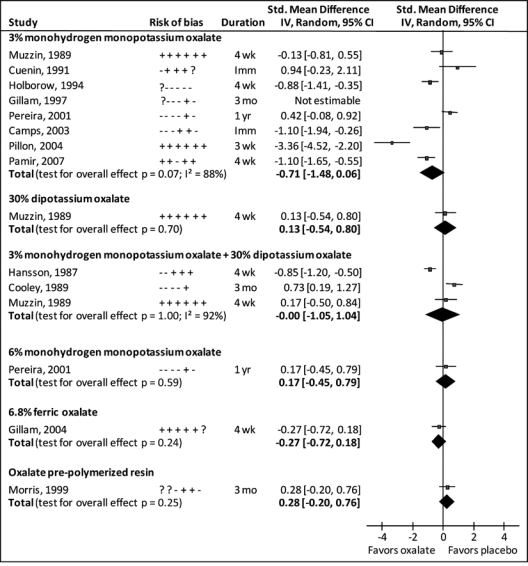
Forest plot of standardized mean differences between oxalate and placebo treatments for dentin hypersensitivity. Risk-of-bias indicates criteria met (+), not met (-), or unclear (?) in: sequence generation; allocation concealment; blinding of participants, care providers, and outcome assessors; completeness of outcome data; selective outcome reporting; and cross-over effects (for split-mouth trials only). Duration Imm, wk, mo, yr indicate Immediate assessment, weeks, months, and years, respectively.
A combination of 3% monohydrogen monopotassium oxalate and 30% dipotassium oxalate was the second most common intervention, and 3 studies evaluated its efficacy (Fig. 2). When daily activities were used as an outcome, this intervention reduced DH. However, when thermal stimuli were used, the DH was either similar to or higher than that of the placebo group (Appendix 2). Based on 59 units in the intervention and placebo groups from 3 studies, the summary SMD for 30% dipotassium oxalate followed by 3% monohydrogen-monopotassium oxalate was 0.00 (95%CI: -1.05, 1.04), with high statistical heterogeneity (92%) (Fig. 2).
Other interventions were evaluated only by single studies (Fig. 2). SMD ranged from −0.27 to +0.28, but results were not statistically significant.
Discussion
This systematic review suggests no benefit from treating DH with oxalates beyond a placebo effect. DH has an intermittent nature, and strong placebo effects have been observed which makes definitive demonstration of clinical efficacy of any treatment difficult (Pashley et al., 2008). Yet, analysis of the data suggested that 3% monohydrogen-monopotassium oxalate may have some beneficial effect; this treatment appears to be a rational first line of oxalate treatment. Analysis of the current data, taken together, cannot determine whether a lack of effect was from a truly ineffective treatment or study design limitations.
A combination of 3% monohydrogen-monopotassium oxalate and 30% dipotassium oxalate was the second-most common DH treatment assessed by clinical studies, yet its efficacy relied heavily on the outcome measure examined. This lack of significant effect was curious considering the more favorable results observed for 3% monohydrogen-monopotassium oxalate contained in the treatment regimen, and the lack of effect observed for 30% dipotassium oxalate alone. This paradox suggests some sort of interference or competition between these treatments, or important and as-yet-unidentified factors in how the two treatments are applied. At present, there appears to be little motivation to use this more complex treatment regimen clinically.
The studies included in this systematic review had several design limitations. With the exception of 3% monohydrogen-monopotassium oxalate, most of the treatments were evaluated by only one study. Additionally, most studies involved small sample sizes (range, 6–87 units). Further, the extent to which studies used strict randomization, concealment, and blinding procedures varied considerably. For split-mouth trials, we considered use of isolation during product placement as a reasonable strategy to avoid cross-over effects. However, patient response to pain on different teeth is not necessarily independent, and the outcome assessment may be confounded by pain response in adjoining or distant teeth.
Lack of standardization in the measurement of pain and poor diagnostic criteria are difficulties facing research in the area of DH (Markowitz and Pashley, 2008). Studies in this review used different stimuli to elicit pain, and treatments decreased DH pain for some stimuli, but not others (see Appendix 2). In addition, numerical and verbal rating scales, 10-cm visual analog scales, and pain threshold tasks were used to measure pain intensity. Utility of pain scales depends on patients understanding the correct way to use the scales, and can be affected by the use of instruction sets (Dixon et al., 2004). In all, the effect of DH treatments remains unclear because of the diverse and sometimes lax methods that have been used to assess efficacy until now.
Taking the lack of standardized measures into account, we completed a meta-analysis using the standardized mean difference (SMD) across studies evaluating the same interventions. Whereas this method of analysis provides a clear way of assessing one overall outcome per study, the statistical heterogeneity across studies suggests that clinical and design differences among the studies were present, and summary estimates may not have been presented. For instance, number of outcomes assessed, follow-up length, and criteria met on the risk of bias assessment differed among the studies. In addition, due to poor reporting of the results in the included studies, assumptions were made to extract the data. Finally, no adjustment was made for within-study correlation. How liberal or conservative the overall analysis is depends on whether this correlation is negative or positive, respectively, but we could not reliably estimate or find such a correlation published in other clinical trials of DH.
In conclusion, available evidence suggests that oxalates are not effective in decreasing DH when compared with placebo, with a possible exception of 3% monohydrogen-monopotassium oxalate. These data should be considered in the treatment of DH until further evidence is available. The great variability observed across clinical trials illuminated the need for strict study protocols, including appropriate randomization and allocation concealment. Standardized use of pain stimuli and scales, both across and within studies, also would aid meta-analysis.
Supplementary Material
Acknowledgments
We thank the authors of the studies included in this systematic review who answered our requests for additional information, Dr. Lei Li for translation of an article in Chinese, and Dr. D.J. Olson for helping with the electronic searches. This work was supported by the National Institute of Dental and Craniofacial Research (grant numbers DE016750, DE016752, DE018436, and DE019202).
Footnotes
A supplemental appendix to this article is published electronically only at http://jdr.sagepub.com/supplemental.
References
- Addy M. (1990). Etiology and clinical implications of dentine hypersensitivity. Dent Clin North Am 34:503-514 [PubMed] [Google Scholar]
- Brannström M, Linden LA, Åström A. (1967). The hydrodynamics of the dental tubule and of pulp fluid. A discussion of its significance in relation to dentinal sensitivity. Caries Res 1:310-317 [DOI] [PubMed] [Google Scholar]
- Camps J, Pashley D. (2003). In vivo sensitivity of human root dentin to air blast and scratching. J Periodontol 74:1589-1594 [DOI] [PubMed] [Google Scholar]
- Canadian Advisory Board on Dentin Hypersensitivity (2003). Consensus-based recommendations for the diagnosis and management of dentin hypersensitivity. J Can Dent Assoc 69:221-226 [PubMed] [Google Scholar]
- Cooley RL, Sandoval VA. (1989). Effectiveness of potassium oxalate treatment on dentin hypersensitivity. Gen Dent 37:330-333 [PubMed] [Google Scholar]
- Cuenin MF, Scheidt MJ, O’Neal RB, Strong SL, Pashley DH, Horner JA, et al. (1991). An in vivo study of dentin sensitivity: the relation of dentin sensitivity and the patency of dentin tubules. J Periodontol 62:668-673 [DOI] [PubMed] [Google Scholar]
- Cunha-Cruz J, Wataha J, Zhou L, Manning W, Trantow M, Bettendorf MM, et al. (2010). Dentin hypersensitivity: choice of treatments by dentists of the Northwest PRECEDENT network. J Am Dent Assoc 141:1097-1105 [DOI] [PMC free article] [PubMed] [Google Scholar]
- DerSimonian R, Laird N. (1986). Meta-analysis in clinical trials. Control Clin Trials 7:177-188 [DOI] [PubMed] [Google Scholar]
- Dixon KE, Thorn BE, Ward LC. (2004). An evaluation of sex differences in psychological and physiological responses to experimentally-induced pain: a path analytic description. Pain 112:188-196; erratum in Pain 115:222, 2005 [DOI] [PubMed] [Google Scholar]
- Gillam DG, Coventry JF, Manning RH, Newman HN, Bulman JS. (1997). Comparison of two desensitizing agents for the treatment of cervical dentine sensitivity. Endod Dent Traumatol 13:36-39 [DOI] [PubMed] [Google Scholar]
- Gillam DG, Newman HN, Davies EH, Bulman JS, Troullos ES, Curro FA. (2004). Clinical evaluation of ferric oxalate in relieving dentine hypersensitivity. J Oral Rehabil 31:245-250 [DOI] [PubMed] [Google Scholar]
- Greenhill JD, Pashley DH. (1981). The effects of desensitizing agents on the hydraulic conductance of human dentin in vitro. J Dent Res 60:686-698 [DOI] [PubMed] [Google Scholar]
- Hansson RE. (1987). The assessment of the subjective nature of pain associated with cervical root dentin hypersensitivity and the evaluation of the effectiveness of dipotassium oxalate in the reduction of cervical root dentin hypersensitivity [thesis]. Ann Arbor, MI: University of Michigan; Available at: http://mirlyn.lib.umich.edu/Record/003907815 (URL accessed 10/12/2010). [Google Scholar]
- Higgins JP, Thompson SG. (2002). Quantifying heterogeneity in a meta-analysis. Stat Med 21:1539-1558 [DOI] [PubMed] [Google Scholar]
- Higgins JPT, Green S, editors (2009). Cochrane handbook for systematic reviews of interventions. Chichester, UK: The Cochrane Collaboration/John Wiley & Sons [Google Scholar]
- Holborow DW. (1994). A clinical trial of a potassium oxalate system in the treatment of sensitive root surfaces. Arch Oral Biol 39(Suppl 1):134 [Google Scholar]
- Holland GR, Närhi MN, Addy M, Gangarosa L, Orchardson R. (1997). Guidelines for the design and conduct of clinical trials on dentine hypersensitivity. J Clin Periodon-tol 24:808-813 [DOI] [PubMed] [Google Scholar]
- Markowitz K, Pashley DH. (2008). Discovering new treatments for sensitive teeth: the long path from biology to therapy. J Oral Rehabil 35:300-315 [DOI] [PubMed] [Google Scholar]
- Morris MF, Davis RD, Richardson BW. (1999). Clinical efficacy of two dentin desensitizing agents. Am J Dent 12:72-76 [PubMed] [Google Scholar]
- Muzzin KB, Johnson R. (1989). Effects of potassium oxalate on dentin hypersensitivity in vivo. J Periodontol 60:151-158 [DOI] [PubMed] [Google Scholar]
- Pamir T, Dalgar H, Onal B. (2007). Clinical evaluation of three desensitizing agents in relieving dentin hypersensitivity. Oper Dent 32:544-548 [DOI] [PubMed] [Google Scholar]
- Pashley DH. (1994). Dentine permeability and its role in the pathobiology of dentine sensitivity. Arch Oral Biol 39(Suppl):73S-80S [DOI] [PubMed] [Google Scholar]
- Pashley DH, Galloway SE. (1985). The effects of oxalate treatment on the smear layer of ground surfaces of human dentine. Arch Oral Biol 30:731-737 [DOI] [PubMed] [Google Scholar]
- Pashley DH, Livingston MJ, Reeder OW, Horner J. (1978). Effects of the degree of tubule occlusion on the permeability of human dentine in vivo. Arch Oral Biol 23:1127-1133 [DOI] [PubMed] [Google Scholar]
- Pashley DH, O’Meara JA, Kepler EE, Galloway SE, Thompson SM, Stewart FP. (1984). Dentin permeability. Effects of desensitizing dentifrices in vivo. J Periodontol 55:522-555 [DOI] [PubMed] [Google Scholar]
- Pashley D, Tay FR, Haywood VB, Collins MA, Drisko CL. (2008). Consensus-based recommendations for the diagnosis and management of dentin hypersensitivity. Comp Contin Educ Dent 29(8 Suppl):1S-35S [Google Scholar]
- Pereira JC, Martineli ACBF, Santiago SL. (2001). Tratamento da hipersensibilidade dentinária com três diferentes formulações à base de oxalato de potássio: estudo clínico [Treating hypersensitive dentin with three different potassium oxalate-based gel formulations: a clinical study]. Rev Fac Odontol Bauru 9:7 [article in Portuguese]. [Google Scholar]
- Pereira JC, Segala AD, Gillam DG. (2005). Effect of desensitizing agents on the hydraulic conductance of human dentin subjected to different surface pre-treatments—an in vitro study. Dent Mater 21:129-138 [DOI] [PubMed] [Google Scholar]
- Pillon FL, Romani IG, Schmidt ER. (2004). Effect of a 3% potassium oxalate topical application on dentinal hypersensitivity after subgingival scaling and root planing. J Periodontol 75:1461-1464 [DOI] [PubMed] [Google Scholar]
- Rees JS, Addy M. (2004). A cross-sectional study of buccal cervical sensitivity in UK general dental practice and a summary review of prevalence studies. Int J Dent Hyg 2:64-69 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.