

Abstract
Enterolith is a rare clinical entity that may be found on imaging or at surgery. We report an unusual case of intestinal obstruction caused by a large uric acid containing enterolith which was formed in the absence of any bowel inflammation, stricture or diverticulum.
Keywords: Intestinal obstruction, Enterolith, Uric acid
Introduction
An enterolith is a mineral concretion or calculus formed anywhere in the gastrointestinal system. Enteroliths usually form inside a diverticulum. Few cases of eneterolithiasis within jejunal, ileal or Meckel’s diverticulum have been reported in literature [1–4]. We report an unusual case of intestinal obstruction caused by a large uric acid containing enterolith in a 55 year old female, who had no evidence of stasis, stricture, inflammation or intestinal diverticulum.
Case Report
A 55 year old women presented at the emergency complaining of vomiting, abdominal pain and distension. She had a history of intermittent abdominal pain, diarrhoea and constipation for the past one year. Her past medical history was not suggestive of any associated illness. She had no history of ingestion of any foreign body. The abdomen was hugely distended. Bowel sounds were sluggish. Abdominal X ray revealed air - fluid levels within dilated loops of small bowel, consistent with intestinal obstruction. A 4 × 4 cm radiopaque shadow was seen in the right lower quadrant (Fig. 1). With the provisional diagnosis of intestinal obstruction, decision was taken to subject the patient to exploratory laparotomy.
Fig. 1.
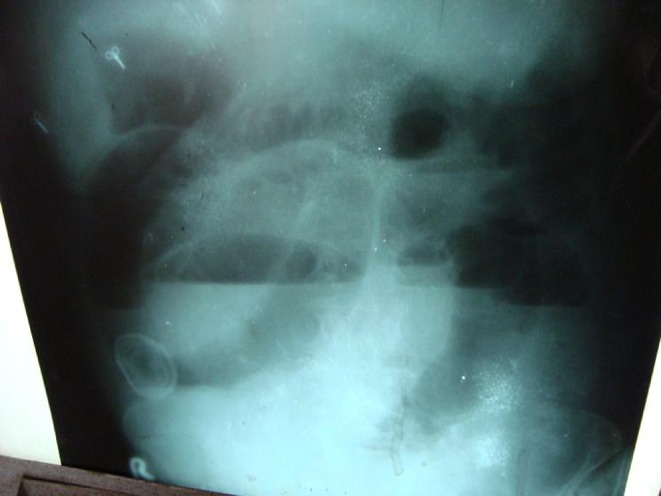
Abdominal X ray showing radio opaque shadow
On exploratory laparotomy there were grossly dilated loops of small bowel. A very hard intraluminal mass was identified in the distal ileum 30 cm proximal to the ileocaecal valve, which was the point of obstruction. There was no evidence of a Meckel’s diverticulum. The gall bladder was normal in appearance. There were no palpable gall stones and there were no adhesions with the surrounding structures. There were no evidence of any bowel inflammation, stricture or diverticulum.
The palpable hard mass was extracted out through an enterotomy (Fig. 2). It was 4.5 × 4 cm in size and brown in colour (Fig. 3). A tube drain was inserted and the abdomen was closed in layers. Except for a minor wound infection, postoperative recovery was uneventful. The patient was discharged home on the 14th post operative day.
Fig. 2.
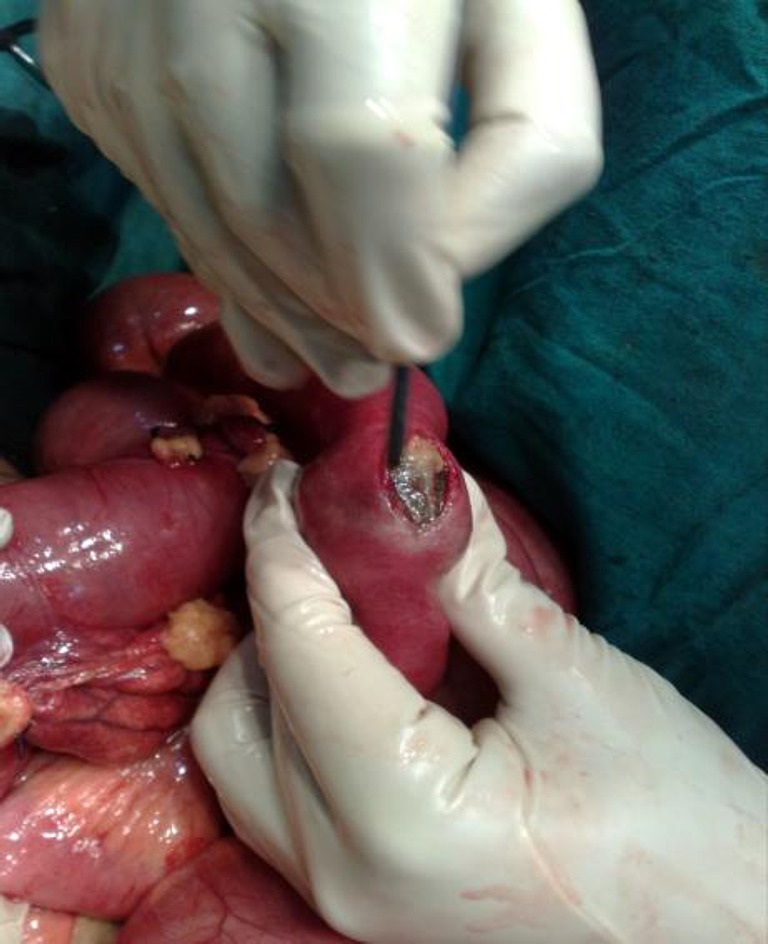
Enterotomy being done
Fig. 3.

The enterolith after extraction
The stone weighed 23.38 gms. Biochemical analysis of the enterolith showed the presence of calcium dihydrate oxalate (80%) and uric acid (20%). Postoperative investigation revealed normal serum calcium and uric acid levels. Renal function tests were normal.
Discussion
Enterolithiasis is a rare disorder most often affecting middle aged females [5]. Statis of the intestinal contents is the underlying cause of stone formation [6]. They have been found in association with tuberculosis, crohn’s disease, blind loop syndrome, congenital or acquired diverticula of the small bowel and intestinal strictures [7]. Enterolithiasis may be symptomatic or asymptomatic. Symptoms include abdominal pain, bleeding, diverticulitis or intestinal obstruction. Most patients have no previous abdominal complaints. A distinction is made between complicated and uncomplicated enterolith ileus. If there are signs of bowel ischaemia, other enteroliths, inflammation of the bowel or if there are signs of a (sealed) perforation, the case is considered a complicated enterolith ileus. If none of these signs are present, then it is an uncomplicated enterolith ileus [3].
Enteroliths may be subdivided into false (which are inspissated intestinal contents) and true [7]. The true enteroliths have been further classified, according to their origin and biochemical components, into two groups by Atwell and Pollock [8]. The first, and commonest type, are formed high in the small bowel where a less alkaline medium allows deposition of choleic and cholic acids. The second type is rarer and arises in the more alkaline distal small bowel as a result of precipitation of minerals salts, predominantly calcium and to a lesser extent magnesium and barium. Many enteroliths are thought to form around a nidus, usually plant material especially fruit skins and stones [5].
The chemical composition of enteroliths are diverse. They include struvite (ammonium magnesium phosphate), calcium phosphate, calcium carbonate, choleic acid, deoxycholic acid and cholic acid.
The differential diagnosis of enterolithiasis should take gall stone ileus and ingestion of foreign body into consideration [9]. The right upper quadrant should always be examined for biliary pathology. A differential diagnosis of an enterolith requires the enterolith, a normal gall bladder and a diverticulum. A chemical analysis is required to rule out gall stones.
The least invasive step in the therapeutic approach is to crush and milk the obstructing enterolith down to the colon. If this fails an enterotomy should be tried, if possible proximal or distal from the obstruction side, in order to make an incision in a less oedematous area. If the first two strategies fail, or if complicated enterolith ileus is present, resection of the involved segment should be considered [3].
This case is unusual because uric acid was one of the components. Veryfew cases have been reported. A duodenal duplication cyst containing uric acid enteroliths has been reported by Bar-Ziv J et al [10]. Secondly this enterolith was not associated with any stricture, inflammation or diverticulum. This is an unusual finding.
To conclude eneterolithiasis must be considered as a potential cause of intestinal obstruction. The differential diagnosis should take gall stones ileus and ingestion of a foreign body into consideration. Management involves crushing and milking of the enterolith, enterotomy and removal or resection of the involved segment as the situation demands.
References
- 1.Vasquez JC, Lee SH, Coimbra R, Hoyt DB. Small Bowel Obstruction Caused By A Meckel’s Diverticulum Enterolith. The Internet Journal of Surgery 2002; Vol. 3, No. 2
- 2.Wroblewski RL, Sticca RP. Primary small bowel enterolithiasis. N England J Med. 2008;359(12):1271. doi: 10.1056/NEJMicm073403. [DOI] [PubMed] [Google Scholar]
- 3.Steenvoorde P, Schaardenburgh P, Viersma JH. Enterolith ileus as a complication of jejunal diverticulosis. Two case reports and a review of the literature. Dig Surg. 2003;20:57–60. doi: 10.1159/000068852. [DOI] [PubMed] [Google Scholar]
- 4.Eyvazzadeh DJ, Karvic SM, Phelan MW, Battafarano RJ. Massive Meckel’s enterolith mimicking urachal carcinoma. Am J Surg Vol. 197, Issue 1 (January 2009) [DOI] [PubMed]
- 5.Gardiner KR, Maxwell EJ. Incidental enterolithiasis. Ulster Med J. 1989;58(2):196–197. [PMC free article] [PubMed] [Google Scholar]
- 6.EL-Tinay OE, Guraya SY, Noreldin O. Enterolithiasis. Saudi J Gastroenterol. 2004;10:96–98. [PubMed] [Google Scholar]
- 7.Javors BR, Bryk D. Enterolithiasis. A report of four cases. Gastrointest Radiol. 1983;8:359–362. doi: 10.1007/BF01948151. [DOI] [PubMed] [Google Scholar]
- 8.Atwell JD, Pollock AV. Intestinal calculi. Br J Surg. 1960;47:367–374. doi: 10.1002/bjs.18004720405. [DOI] [PubMed] [Google Scholar]
- 9.Korniprat P, Langner C, Mischinger HJ. Enterolithiasis in jejunal diverticulosis, a rare cause of obstruction of the small intestine : a case report. Wien Klin Wochenschr. 2005;117(7–8):297–299. doi: 10.1007/s00508-004-0277-8. [DOI] [PubMed] [Google Scholar]
- 10.Bar-Ziv J, Katz R, Nobel M, Antebi E. Duodenal duplication cyst with enteroliths: computed tomography and ultrasound diagnosis. Abdom Imaging. 1989;14(1):220–222. doi: 10.1007/BF01889201. [DOI] [PubMed] [Google Scholar]