

Abstract
Background:
Double-injection models of subarachnoid hemorrhage (SAH) in rats are the most effective in producing vasospasm, delayed neurological deficits and infarctions. However, they require two large surgeries to expose the femoral artery and the atlanto-occipital membrane. We have developed a minimally-invasive modification that prevents confounding effects of surgical procedures, leakage of blood from the subarachnoid space and minimizes risk of infection.
Methods:
Rats are anesthetized and the ventral tail artery is exposed through a small (5 mm), midline incision, 0.2 mL of blood is taken from the artery and gentle pressure is applied for hemostasis. The rat is flipped prone, and with the head flexed to 90 degrees in a stereotactic frame, a 27G angiocath is advanced in a vertical trajectory, level with the external auditory canals. Upon puncturing the atlanto-occipital membrane, the needle is slowly advanced and observed for cerebrospinal fluid (CSF). A syringe withdraws 0.1 mL of CSF and the blood is injected into the subarachnoid space. The procedure is repeated 24 hours later by re-opening the tail incision. At 8 days, the rats are euthanized and their brains harvested, sectioned, and incubated with triphenyltetrazolium chloride (TTC).
Results:
Rats develop neurological deficits consistent with vasospasm and infarction as previously described in double-injection models. Cortical and deep infarctions were demonstrated by TTC staining and on histopathology.
Conclusions:
A minimally invasive, double-injection rat model of SAH and vasospasm is feasible and produces neurological deficits and infarction. This model can be used to study neuroprotective treatments for vasospasm and delayed neurological deficits following SAH, reducing the confounding effects of surgical interventions.
Keywords: Delayed ischemic deficit, double-injection model, rat, subarachnoid hemorrhage, vasospasm
INTRODUCTION
Several methods have been proposed for the experimental modeling of subarachnoid hemorrhage (SAH) and resulting vasospasm and delayed neurological deficits.[20] Most have major shortcomings either in that they do not closely recreate the conditions of human SAH, are overly invasive, are not consistently reproducible, are not cost-effective and/or have a high mortality rate, precluding further studies of outcome.[20] In particular, with regards to vasospasm, many models have not been able to produce consistent vasospasm with resulting neurological deficits as are seen in clinical SAH. Those rat models have been able to produce these phenomenon are inconsistent and plagued by a very high mortality rate (close to 50% in the case of the endovascular puncture model).[12]
The double-injection rat model was first presented by Solomon et al.[19] It has been further refined and described by subsequent authors.[11,15,17,21,22] This method, which involves two temporally distinct injections of arterial blood into the subarachnoid space, has been demonstrated to be effective in producing vasospasm, delayed neurological deficits, and cerebral infarctions in the experimental animals with a relatively low mortality rate.[8,22] However, the method requires two invasive surgeries. One, open exposure of the femoral artery, is required to obtain adequate arterial blood. The second is a suboccipital exposure of the atlanto-occipital membrane for the subarachnoid injection of the blood into the cisterna magna. Leakage of blood from the injection site and wound infections during the survival period are other potential problems, which have been discussed by previous authors.[15,21,22]
We have developed a minimally invasive modification that maintains the reproducibility and effect of the double-injection SAH model while preventing the potentially confounding effects of the surgical procedures, avoiding leakage of blood from the subarachnoid space after injection and minimizing the risk of wound infection.
MATERIALS AND METHODS
Male adult Sprague-Dawley rats are anesthetized on Day 1 of the experimental protocol by intraperitoneal injection of midazolam (1 mg/kg) and ketamine (100 mg/kg). This anesthesia is commonly used in rat SAH models, its safety has been proven for imaging procedures in neurologically impaired rats and it has not been shown to cause significant changes in cerebral blood flow.[5,13,22]
The anesthetized rats are placed supine on a heating plate to maintain body temperature at 37°C. Under the microscope, the ventral tail artery is exposed through a small (5 mm), midline incision. Using a 27-gauge needle and heparinized syringe, 0.2 mL of arterial blood is taken from the artery and gentle pressure is applied for hemostasis. The tail incision is then closed.
The rats are then flipped prone and the head is fixed in a stereotactic frame. The head is flexed to 90 degrees to horizontal and secured in this position. A 27-gauge angiocath is secured to a vertically oriented microdrive and is aligned horizontally with the external auditory canals [Figure 1]. The needle is advanced in a vertical trajectory until it punctures the atlanto-occipital membrane. The needle is slowly advanced and the microcatheter is observed for a cerebrospinal fluid column. A syringe is then attached and 0.1 mL of cerebrospinal fluid is withdrawn. The arterial blood obtained in the first step (0.2 mL) is then injected into the subarachnoid space of the cisterna magna over a period of 60 seconds, as has been described for the double-injection model previously. The catheter is withdrawn and the rat is kept in a head-down position while awakening from anesthesia to ensure adequate subarachnoid distribution of the injected blood.
Figure 1.
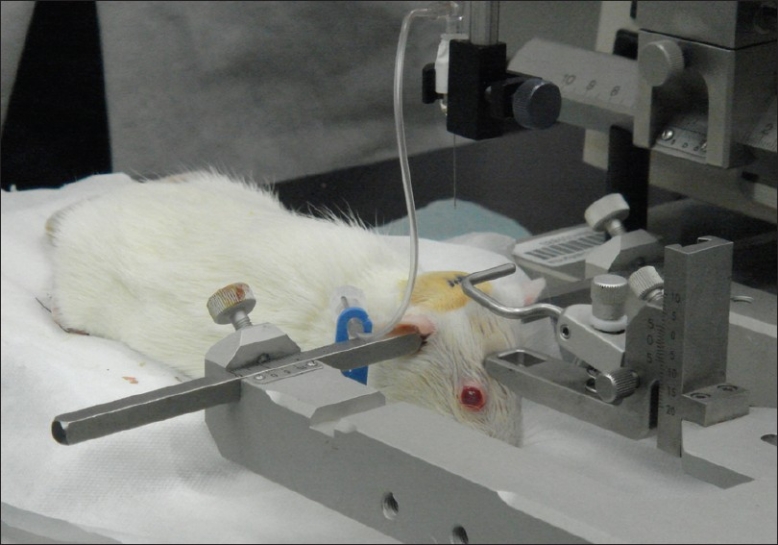
Cisternal Injection Procedure - Once the rat is in the stereotactic frame with head positioned at 90 degrees to horizontal, the cisterna magna is aligned with the intermeatal line (external auditory canal)
This same procedure is repeated 24 hours later (Day 2) by re-opening the tail incision. If need be, the artery can be exposed more proximally to obtain this blood sample. The rats are evaluated daily thereafter and scored on a standard neurological behavioral score.[3]
On Day 8, the rats are euthanized and their brains immediately harvested. The brains are sectioned coronally into 2 mm slices. These slices are then incubated at 37°C with 2% triphenyltetrazolium chloride (TTC) for 20 minutes for identification of infarcted brain.[3,9,14] The brain tissue is then post-fixed for 2 hours in 4% paraformaldehyde. The stained sections are assessed and photographed grossly for areas consistent with infarction (areas unstained by TTC). The samples are then cryoprotected for 2 days in 30% sucrose, frozen, and sectioned in a cryostat at 50 μm for standard histopathology by a neuropathologist. The cerebral arteries were not isolated separately from the brain.
Our Institution's Animal Care Committee approved this protocol.
DISCUSSION
Results of our initial experience
To date we have performed this technique on two rats. Using the method of evaluation first proposed by Bederson et al.,[3] the following deficits, as previously described in double-injection models and consistent with vasospasm and cerebral infarction, were observed: asymmetrical extension of forelimbs toward the floor when held by the tail, including abnormal flexion; asymmetrical grasping with the forelimb when the forelimb is place on a surface and the rat is slid laterally; and a gait preference that producing circling behavior toward a paretic or plegic side. These deficits were observed starting on Day 3 and progressing through Day 5. Their neurological score was 3 for Days 3 through 8.
Gross inspection of the harvested brains shows diffuse SAH in the basal cisterns [Figure 2a], confirming the adequate subarachnoid distribution of blood from the cisterna magna injection site. Inspection and sectioning of the brain did not reveal any intraparenchymal needle injury or hematoma. Additionally, the triphenyltetrazolium chloride staining identifies areas of infarcted brain that were seen grossly. Following experimental SAH, TTC demonstrates numerous cortical and deep nuclei infarctions in the sectioned brain [Figure 2b]. TTC findings correlated with findings on histopathology, which demonstrated focal chronic necrosis in the brain, consistent with recent infarction [Figure 3].
Figure 2.
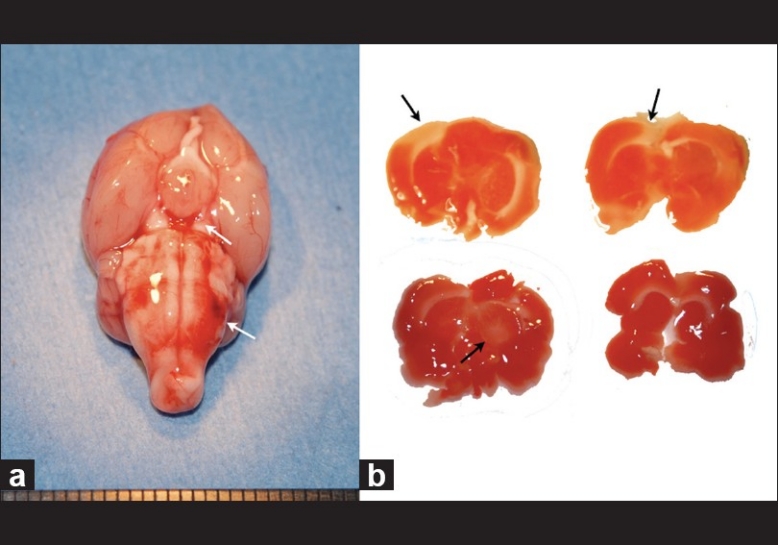
(a) Gross pathology of harvested brain on Day 8. Note that the cisternal injection produced accumulation of blood in the prepontine and interpeduncular cisterns (white arrows). (b) Triphenyltetrazolium chloride staining reveals numerous cortical and deep infarctions in the sectioned brain. These infarctions correlated with the neurological deficits observed in the rat prior to euthanasia
Figure 3.
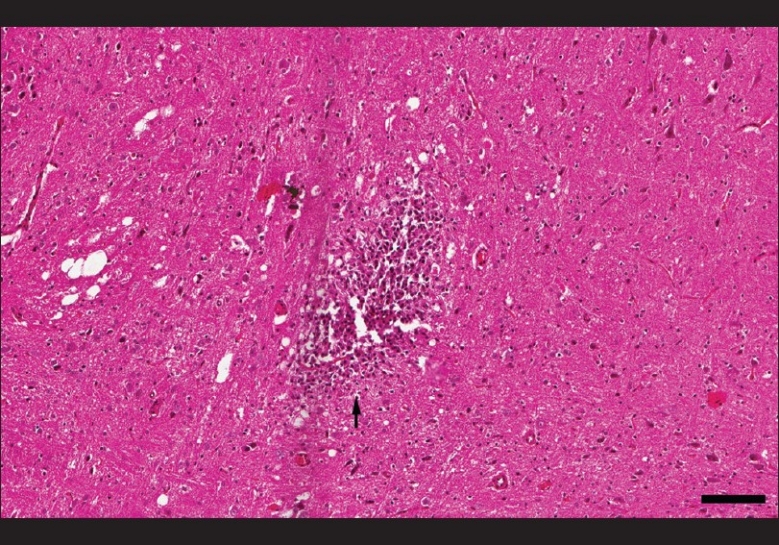
Histopathology of rat brain, demonstrating a focus of chronic necrosis consistent with recent infarction (black arrow, scale bar 100 μm)
Impact and comparison to previous models
Spontaneous SAH from rupture of a cerebral aneurysm is a major health problem.[2] In addition to the initial hemorrhagic ictus, one of the major causes of the morbidity and mortality associated with SAH is the resulting vasospasm and delayed neurological deficits, causing clinical neurological deterioration in almost a third of all patients.[10,23] Despite the advances in the understanding of SAH and vasospasm, the underlying pathophysiology is incompletely understood. Additionally, while treatment to prevent re-rupture of aneurysm has progressed considerably in the last two decades, little has been achieved towards preventing delayed deficits. Despite triple-H therapy, calcium channel blockers, and endovascular treatments, vasospasm and delayed deficits still impact many patients after SAH.
A consistently reproducible, easy-to-perform, and cost-effective experimental model to simulate aneurysm rupture and delayed neurological deterioration is invaluable to future investigations into both the pathophysiology of SAH as well as neuroprotective treatments that aim to reduce morbidity and mortality following SAH.[20] Some previous models have proven ineffective in producing vasospasm and/or delayed neurological deficits as are seen frequently in human SAH (such as rat vessel puncture and single-injection models). Other models are more effective in modeling human SAH but suffer from various drawbacks. For example, large animal models (dogs and non-human primates) are much more difficult and expensive to perform. Some models require very traumatic techniques to create the SAH, such as a craniotomy or orbital exenteration. Intracranial vessel puncture techniques are both invasive as well as inconsistent in terms of the degree of SAH that results and therefore the resulting clinical manifestations and mortality. While promising in terms of the severity of deficits, cerebral injury and similarity to human disease, endovascular puncture models in rats carry an unacceptably high mortality rate (close to 50%).[12]
The one model that has been shown to both consistently produce vasospasm, delayed neurological deficits, and infarction and to be relatively cost-effective, is easy to perform (compared to large animal models) and has a low mortality rate is the rat cisternal double-injection model, which utilizes two injections of arterial blood into the cisterna magna spaced 24 hours apart.[8,15,19,21,22] This technique produces reliable vasospasm, infarction and delayed deficits with relatively low mortality (4-9%). However, there are still some disadvantages to the model. While it is less invasive than some models, it still requires two large incisions to expose both the femoral artery (to obtain arterial blood) and the atlanto-occipital membrane (for puncture of the cisterna magna and blood injection). These large incisions put stress on the animal and are potential sources for infection. Previous authors have also described a problem with leakage of blood from the injection site, requiring the use of hemostypticum patches and cotton.
Among the multiple mechanisms involved, it has been suggested that an inflammatory response and the associated leukocyte–endothelial cell interactions play a significant role in the pathophysiology of cerebral vasospasm.[4,7,16] Therefore, we feel that invasive and stressful procedures, which produce inflammation in the experimental animal, should be kept to a minimum to avoid confounding the study of cerebral vasospasm and its effects. A model that minimizes additional sources of inflammation appears to be ideal. For this reason, we set out to refine the double-injection model of SAH and vasospasm. By using a percutaneous, stereotactic injection technique, eliminating the suboccipital incision and dissection and moving the arterial access point to the ventral tail artery, we feel that the model is significantly streamlined while reducing surgical trauma and risk for infection. The percutaneous injection technique also eliminates significant leakage of blood from the subarachnoid space, obviating the need for foreign body implants (hemostypticum and cotton), which could contribute to further inflammation. While percutaneous puncture of the rats cisterna magna has been previously described for CSF sampling purposes, to our knowledge it has not been used for SAH double-injection models.[6,18] Likewise, while tail artery blood collection has been used in other studies, including in one study that used a single injection of blood into the pre-chiasmatic cistern through a craniotomy, it has not been used in cisterna magna double-injection SAH models to our knowledge.[1] Our initial experience suggests that these modifications do not sacrifice efficacy, as the expected presence of delayed neurological deficits and cerebral infarction have been observed. This minimally-invasive, double-injection model of SAH and vasospasm appears to be an excellent platform for future laboratory investigations of the pathophysiology of SAH and delayed neurological deficits as well as for testing of neuroprotective treatments for this devastating disease.
In conclusion, a minimally invasive, double-injection rat model of SAH and vasospasm is feasible and produces neurological deficits and infarction as has been previously demonstrated with similar models. This model may be used to study neuroprotective treatments for vasospasm and delayed neurological deficits following SAH, reducing the confounding effects of surgical interventions inherent to most other models.
Acknowledgments
The authors wish to acknowledge Harry Vinters, MD, for the processing and analysis of the pathological specimens.
Footnotes
Available FREE in open access from: http://www.surgicalneurologyint.com/text.asp?2011/2/1/99/83023
Contributor Information
Joshua R. Dusick, Email: jdusick@mednet.ucla.edu.
Brandon C. Evans, Email: bcevans@mednet.ucla.edu.
Azim Laiwalla, Email: azim@ucla.edu.
Scott Krahl, Email: scott.krahl@va.gov.
Nestor R. Gonzalez, Email: ngonzalez@mednet.ucla.edu.
REFERENCES
- 1.Ansar S, Edvinsson L. Equal contribution of increased intracranial pressure and subarachnoid blood to cerebral blood flow reduction and receptor upregulation after subarachnoid hemorrhage. Laboratory investigation. J Neurosurg. 2009;111:978–87. doi: 10.3171/2007.3.16738. [DOI] [PubMed] [Google Scholar]
- 2.Becker KJ. Epidemiology and clinical presentation of aneurysmal subarachnoid hemorrhage. Neurosurg Clin N Am. 1998;9:435–44. [PubMed] [Google Scholar]
- 3.Bederson JB, Pitts LH, Tsuji M, Nishimura MC, Davis RL, Bartkowski H. Rat middle cerebral artery occlusion: Evaluation of the model and development of a neurologic examination. Stroke. 1986;17:472–6. doi: 10.1161/01.str.17.3.472. [DOI] [PubMed] [Google Scholar]
- 4.Chaichana KL, Pradilla G, Huang J, Tamargo RJ. Role of inflammation (leukocyte-endothelial cell interactions) in vasospasm after subarachnoid hemorrhage. Surg Neurol. 2009 doi: 10.1016/j.surneu.2009.05.027. [In press] [DOI] [PubMed] [Google Scholar]
- 5.Dittmar MS, Fehm NP, Vatankhah B, Horn M. Ketamine/xylazine anesthesia for radiologic imaging of neurologically impaired rats: Dose response, respiratory depression, and management of complications. Comp Med. 2004;54:652–5. [PubMed] [Google Scholar]
- 6.Frankmann SP. A technique for repeated sample of CSF from the anesthetized rat. Physiol Behav. 1986;37:489–93. doi: 10.1016/0031-9384(86)90211-8. [DOI] [PubMed] [Google Scholar]
- 7.Gallia GL, Tamargo RJ. Leukocyte-endothelial cell interactions in chronic vasospasm after subarachnoid hemorrhage. Neurol Res. 2006;28:750–8. doi: 10.1179/016164106X152025. [DOI] [PubMed] [Google Scholar]
- 8.Guresir E, Raabe A, Jaiimsin A, Dias S, Raab P, Seifert V, et al. Histological evidence of delayed ischemic brain tissue damage in the rat double-hemorrhage model. J Neurol Sci. 2010;293:18–22. doi: 10.1016/j.jns.2010.03.023. [DOI] [PubMed] [Google Scholar]
- 9.Isayama K, Pitts LH, Nishimura MC. Evaluation of 2,3,5-triphenyltetrazolium chloride staining to delineate rat brain infarcts. Stroke. 1991;22:1394–8. doi: 10.1161/01.str.22.11.1394. [DOI] [PubMed] [Google Scholar]
- 10.Kassell NF, Torner JC, Haley EC, Jr, Jane JA, Adams HP, Kongable GL. The International Cooperative Study on the Timing of Aneurysm Surgery. Part 1: Overall management results. J Neurosurg. 1990;73:18–36. doi: 10.3171/jns.1990.73.1.0018. [DOI] [PubMed] [Google Scholar]
- 11.Lee JY, Huang DL, Keep R, Sagher O. Characterization of an improved double hemorrhage rat model for the study of delayed cerebral vasospasm. J Neurosci Methods. 2008;168:358–66. doi: 10.1016/j.jneumeth.2007.10.029. [DOI] [PubMed] [Google Scholar]
- 12.Lee JY, Sagher O, Keep R, Hua Y, Xi G. Comparison of experimental rat models of early brain injury after subarachnoid hemorrhage. Neurosurgery. 2009;65:331–43. doi: 10.1227/01.NEU.0000345649.78556.26. [DOI] [PubMed] [Google Scholar]
- 13.Lei H, Grinberg O, Nwaigwe CI, Hou HG, Williams H, Swartz HM, et al. The effects of ketamine-xylazine anesthesia on cerebral blood flow and oxygenation observed using nuclear magnetic resonance perfusion imaging and electron paramagnetic resonance oximetry. Brain Res. 2001;913:174–9. doi: 10.1016/s0006-8993(01)02786-x. [DOI] [PubMed] [Google Scholar]
- 14.Li F, Irie K, Anwer MS, Fisher M. Delayed triphenyltetrazolium chloride staining remains useful for evaluating cerebral infarct volume in a rat stroke model. J Cereb Blood Flow Metab. 1997;17:1132–5. doi: 10.1097/00004647-199710000-00016. [DOI] [PubMed] [Google Scholar]
- 15.Meguro T, Clower BR, Carpenter R, Parent AD, Zhang JH. Improved rat model for cerebral vasospasm studies. Neurol Res. 2001;23:761–6. doi: 10.1179/016164101101199144. [DOI] [PubMed] [Google Scholar]
- 16.Pradilla G, Chaichana KL, Hoang S, Huang J, Tamargo RJ. Inflammation and cerebral vasospasm after subarachnoid hemorrhage. Neurosurg Clin N Am. 2010;21:365–79. doi: 10.1016/j.nec.2009.10.008. [DOI] [PubMed] [Google Scholar]
- 17.Prunell GF, Mathiesen T, Diemer NH, Svendgaard NA. Experimental subarachnoid hemorrhage: Subarachnoid blood volume, mortality rate, neuronal death, cerebral blood flow, and perfusion pressure in three different rat models. Neurosurgery. 2003;52:165–75. doi: 10.1097/00006123-200301000-00022. discussion 175-6. [DOI] [PubMed] [Google Scholar]
- 18.Sharma AK, Schultze AE, Cooper DM, Reams RY, Jordan WH, Snyder PW. Development of a percutaneous cerebrospinal fluid collection technique in F-344 rats and evaluation of cell counts and total protein concentrations. Toxicol Pathol. 2006;34:393–5. doi: 10.1080/01926230600798609. [DOI] [PubMed] [Google Scholar]
- 19.Solomon RA, Antunes JL, Chen RY, Bland L, Chien S. Decrease in cerebral blood flow in rats after experimental subarachnoid hemorrhage: A new animal model. Stroke. 1985;16:58–64. doi: 10.1161/01.str.16.1.58. [DOI] [PubMed] [Google Scholar]
- 20.Titova E, Ostrowski RP, Zhang JH, Tang J. Experimental models of subarachnoid hemorrhage for studies of cerebral vasospasm. Neurol Res. 2009;31:568–81. doi: 10.1179/174313209X382412. [DOI] [PubMed] [Google Scholar]
- 21.Vatter H, Gueresir E, Seifert V. Blood Injection Subarachnoid Hemorrhage Rat Model. In: Chen J, Xu ZC, Xu XM, Zhang JH, editors. Animal Models of Acute Neurological Injuries. Totowa NJ: Humana Press; 2009. [Google Scholar]
- 22.Vatter H, Weidauer S, Konczalla J, Dettmann E, Zimmermann M, Raabe A, et al. Time course in the development of cerebral vasospasm after experimental subarachnoid hemorrhage: Clinical and neuroradiological assessment of the rat double hemorrhage model. Neurosurgery. 2006;58:1190–7. doi: 10.1227/01.NEU.0000199346.74649.66. [DOI] [PubMed] [Google Scholar]
- 23.Weir B, Grace M, Hansen J, Rothberg C. Time course of vasospasm in man. J Neurosurg. 1978;48:173–8. doi: 10.3171/jns.1978.48.2.0173. [DOI] [PubMed] [Google Scholar]