

Abstract
A rare case of abdominal trauma, a handlebar hernia, is described, as well as a review of the pertinent literature. A 7-year-old boy presented to our emergency room after sustaining blunt force to the abdomen; he fell on the handlebar of his bicycle. Immediately after the accident, a bulge was noticeable at the point of impact. Handlebar hernia is a diagnosis that is easily missed, which can lead to strangulation and incarceration of the bowel. With this case report, we hope to augment the knowledge on traumatic abdominal wall hernia, hopefully leading to early diagnosis and treatment.
Keywords: Traumatic abdominal wall hernia, Blunt trauma, Children, Handlebar hernia
Introduction
Trauma to the abdomen, involving blunt or cavitating force, often results in damage to the intestines. However, when the directed force is too frail to cause intra-abdominal damage and too blunt to penetrate the abdominal wall, there still is a chance of injury: traumatic abdominal wall hernia. Although its pathogenesis remains unclear, it seems to involve a sudden increase in intra-abdominal pressure in combination with tangential shearing stress, leading to interruption of the abdominal muscle and fascia layers. We describe a rare case of traumatic abdominal wall hernia in a 7-year-old boy who endured blunt force to the abdomen. The literature involving handlebar hernia is reviewed.
Case report
A nearly 7-year-old boy, with no relevant past history, visited our emergency department with abdominal pain and swelling after a fall from his bike. Whilst riding his bike, he had fallen and his abdomen had landed on the handlebar. Immediately after the accident, his mother noticed a swelling where the handlebar had hit his abdomen. They visited the general practitioner on call who subsequently sent him to our emergency department. Apart from pain, he had no other complaints. On physical examination, he seemed to be not ill and he was haemodynamically stable. Examination of the abdomen showed a circular contusion of the skin several centimetres below the umbilicus just on the right of the midline (Fig. 1). On palpation, a clear defect of the rectus fascia could be felt. There were no signs of peritonitis suggesting an enteral lesion. He was admitted for observation and discharged the following morning. He was scheduled for surgery 1 week later. During the operation, a skin-line incision was performed over the fascia defect, revealing a rupture of the musculus rectus abdominis, as well as a total rupture of the right rectus fascia (Fig. 2). The rectus sheath was closed with a continuous Vicryl suture. The muscle defect was approximated with interrupted Vicryl sutures. The skin was closed intracutaneously. He was discharged the following day and recovered uneventfully.
Fig. 1.

Circular contusion on the place of impact
Fig. 2.
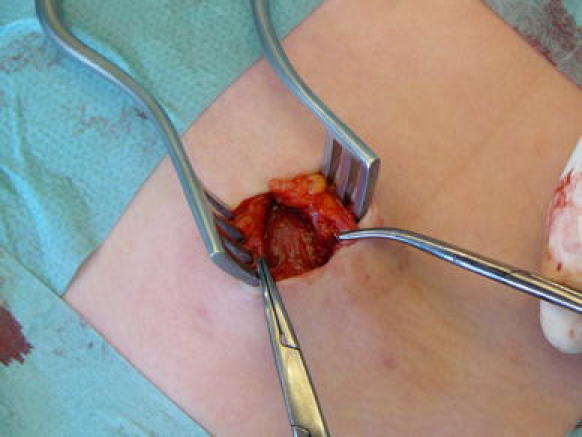
Rupture of the musculus rectus abdominis, as well as a total rupture of the right rectus fascia
Discussion
A traumatic abdominal wall hernia occurs after trauma in which a small focal point, such as a handlebar, seat belt or any other obdurate object, localises blunt force to the abdomen. This force, being blunt in nature, does not penetrate the abdomen; however, due to the aforementioned focal point, the transferred energy dissipates throughout the abdominal wall. In combination with the increased abdominal pressure, due to direct impact, this leads to the shearing of muscle and fascia layers. This shearing is thought to occur at anatomic weak points, such as the inguinal region or the lower abdomen lateral to the rectus muscle. The elastic qualities of the skin keep it from tearing apart, resulting in an abdominal wall hernia [1].
Although there are several classification systems, the one most often used in traumatic abdominal wall hernia is based on the amount of blunt force involved in the accident. This is the main determent used to categorise traumatic abdominal wall hernias. With a large force, such as that caused by a motorcycle accident or resulting from a fall, there tends to be larger and more diffuse defects. Simultaneous rupture of the diaphragm may also occur with this increase in force. When the injury involves decelerating force, as in the case of a car accident involving seat belts, another category can be seen; traumatic abdominal wall hernia involving intra-abdominal bowel herniation. The last category, named handlebar hernia, involves a small force which is localised through an adamant object, such as the handlebar of a bicycle [2, 3].
Traumatic abdominal wall hernia should be considered in any patient who presents to the emergency room after sustaining blunt trauma to the abdomen. The following clinical signs can help establish the diagnosis. On inspection, there may be an imprint present on the abdomen through which the force was channelled. This imprint is usually accompanied by ecchymosis. Around the imprint, a tender mass may be palpated, reminiscent of a normal hernia. Apart from these findings, the abdominal examination is usually normal. In severe cases where the impact has also caused damage to the intestines, there can be signs of peritonitis. All of the above-mentioned symptoms may, however, also be absent, as there are case reports of patients in which symptoms presented 48 h after the accident [4].
Additional research, in the form of an ultrasound, Fig. 3, or computed tomography (CT) scan, Fig. 4, greatly helps to establish the diagnosis [5, 6].
Fig. 3.

Ultrasonography showing abdominal wall hernia after trauma
Fig. 4.

Computed tomography (CT) scan showing abdominal wall hernia after trauma
The differential diagnosis for traumatic abdominal wall hernia includes other causes for bulges in the inguinal or lower abdomen region. After trauma, a haematoma of the rectus sheath may mimic traumatic abdominal wall hernia. While usually seen before the accident by the patient or his family, a pre-existing inguinal hernia should not be ruled out. Although rare, abdominal neoplasms, such as nephroblastoma and lymphoma, are occasionally unveiled for the first time after trauma occurs to the abdomen [7].
The treatment of traumatic abdominal wall hernia consists of surgical exploration with closure of the defect. When the defect is small and localised, which is the case in handlebar hernia, closure can be achieved with non-absorbable suture. However, the condition of the muscle and fascia layer should be taken into account; primary closure of sheared layers should not be considered to be as strong as closure with a prosthetic graft. With larger defects, seen after high-energy impacts, prosthetic materials are often used to achieve closure. Accompanying damage to the intestines requires tailored intervention. If there are signs of intra-abdominal damage on presentation, generalised peritonitis or evidence of perforation on CT, primary surgical intervention should be carried out promptly. Smaller defects, in which intra-abdominal injury is absent, may also be corrected on a delayed basis. A case report with conservative treatment has been described; however, due to the risk of strangulation and incarceration, surgical intervention is favoured [8, 9].
Table 1 lists 23 previously published cases of handlebar hernia, with our case being the 24th. The ages of the patients ranged from 4 to 14 years. The most common traumatising agent was a bicycle handlebar. The location of injuries were equally divided between the right middle and left lower quadrant of the abdomen. In none of the cases were prosthetic materials used; primary closure was achieved through layered closure. In all cases, recovery was uneventful.
Table 1.
Previously published cases on handlebar hernia
| Age/sex | Reference | Traumatising agent | Injury location | Surgical management |
|---|---|---|---|---|
| 14/M | Landry (1956) [10] | Motorcycle handlebar | LLQ | Laparotomy and layered closure |
| 9/M | Roberts (1964) [11] | Bicycle handlebar | LLQ | Layered closure |
| 9/F | Maunola and Kekomaki (1965) [12] | Bicycle handlebar | LLQ | Exploratory laparotomy, repair of muscle and sheath |
| 8/F | Pendl (1970) [13] | Bicycle handlebar | RLQ | Layered closure |
| 7/M | Herbert and Turner (1973) [14] | Bicycle handlebar | LLQ | Layered closure |
| 6/M | Atiemo and Goswami (1974) [15] | Gored by a cow | LLQ | Layered closure |
| 4/F | Hollwarth (1977) [16] | Scooter handlebar | RLQ | Layered closure |
| 6/M | Hollwarth (1977) [16] | Bicycle handlebar | RLQ | Closure |
| 7/M | Hollwarth (1977) [16] | Bicycle handlebar | LUQ | Closure |
| 13/M | Hollwarth (1977) [16] | Bicycle handlebar | Symphysis pubis | Closure |
| 11/M | Dreyfuss et al. (1986) [17] | Bicycle handlebar | Rectus abdominis | Debridement and layered closure |
| 8/M | Schneegans (1988) [18] | Bicycle handlebar | RLQ | Appendectomy, layered closure |
| 7/M | Mitchiner (1990) [19] | Bicycle handlebar | LUQ | Reduction of bowel and layered closure |
| 5/M | Damschen et al. (1994) [20] | Bicycle handlebar | RLQ | Reduction of bowel and layered closure |
| 6/M | Kubalak (1994) [21] | Gored by a cow | RLQ | Closure |
| 8/M | Kubalak (1994) [21] | Bicycle handlebar | RLQ | Layered closure |
| 9/F | Kubalak (1994) [21] | Bicycle handlebar | RLQ | Closure |
| 7/M | Iuchtman et al. (1997) [22] | Bicycle handlebar | RLQ | Closure |
| 11/M | Perez et al. (1998) [23] | Bicycle handlebar | LLQ | Laparotomy and layered closure |
| 9/M | Kubota et al. (1999) [3] | Bicycle handlebar | RLQ | Reduction of bowel and layered closure |
| 11/M | Fraser et al. (2002) [7] | Bicycle handlebar | RLQ | Layered closure |
| 7/M | Mancel and Aslam (2003) [5] | Bicycle handlebar | LLQ | Layered closure |
| 11/M | Goliath et al. (2004) [24] | Bicycle handlebar | RLQ | Layered closure |
| 7/M | van Bemmel et al. (2009) | Bicycle handlebar | Rectus abdominis | Layered closure |
Conclusion
Traumatic abdominal wall hernia is a rare diagnosis. Lack of knowledge and the possibility of the absence of apparent clinical signs on presentation make this an injury which is easily missed. The mechanism of trauma to the abdomen and the recognition of sometimes subtle signs should prompt high suspicion to the presence of a traumatic abdominal wall hernia. When in doubt, additional ultrasound or computed tomography (CT) scanning greatly helps to establish the diagnosis. Early recognition, and treatment when needed, may lead to a significant reduction of morbidity associated with strangulation and incarceration. Although the aetiology of the trauma predisposes to the use of prosthetic materials, in children, primary closure seems to achieve an excellent result [4].
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
References
- 1.Cheng SP, Ko WC, Liu CL. Handlebar hernia: a misleading term. Injury Extra. 2005;36:309–311. doi: 10.1016/j.injury.2004.07.056. [DOI] [Google Scholar]
- 2.Haimovici L, Papafragkou S, Kessler E, Angus G. Handlebar hernia: traumatic abdominal wall hernia with multiple enterotomies. A case report and review of the literature. J Pediatr Surg. 2007;42:567–569. doi: 10.1016/j.jpedsurg.2006.10.092. [DOI] [PubMed] [Google Scholar]
- 3.Kubota A, Shono J, Yonekura T, Hoki M, Asano S, Hirooka S, Kosumi T, Kato M, Oyanagi H. Handlebar hernia: case report and review of pediatric cases. Pediatr Surg Int. 1999;15:411–412. doi: 10.1007/s003830050616. [DOI] [PubMed] [Google Scholar]
- 4.Losanoff JE, Richman BW, Jones JW. Handlebar hernia: ultrasonography-aided diagnosis. Hernia. 2002;6:36–38. doi: 10.1007/s10029-002-0041-9. [DOI] [PubMed] [Google Scholar]
- 5.Mancel B, Aslam A. Traumatic abdominal wall hernia: an unusual bicycle handlebar injury. Pediatr Surg Int. 2003;19:746–747. doi: 10.1007/s00383-003-1064-8. [DOI] [PubMed] [Google Scholar]
- 6.Goh SCJ, Welch C, Houlden CJ, Gosling DC. Traumatic bicycle handlebar hernia. Eur J Emerg Med. 2008;15:179–180. doi: 10.1097/MEJ.0b013e3282c48bef. [DOI] [PubMed] [Google Scholar]
- 7.Fraser N, Milligan S, Arthur RJ, Crabbe DC. Handlebar hernia masquerading as an inguinal haematoma. Hernia. 2002;6:39–41. doi: 10.1007/s10029-002-0051-7. [DOI] [PubMed] [Google Scholar]
- 8.Belgers HJ, Hulsewé KW, Heeren PA, Hoofwijk AG. Traumatic abdominal wall hernia: delayed presentation in two cases and a review of the literature. Hernia. 2005;9:388–391. doi: 10.1007/s10029-005-0338-6. [DOI] [PubMed] [Google Scholar]
- 9.Litton K, Izzidien AY, Hussien O, Vali A. Conservative management of a traumatic abdominal wall hernia after a bicycle handlebar injury (case report and literature review) J Pediatr Surg. 2008;43:e31–e32. doi: 10.1016/j.jpedsurg.2007.12.059. [DOI] [PubMed] [Google Scholar]
- 10.Landry RM. Traumatic hernia. Am J Surg. 1956;91:301–302. doi: 10.1016/0002-9610(56)90427-5. [DOI] [PubMed] [Google Scholar]
- 11.Roberts GR. Traumatic abdominal wall rupture. Br J Surg. 1964;51:153–154. doi: 10.1002/bjs.1800510213. [DOI] [PubMed] [Google Scholar]
- 12.Maunola R, Kekomaki M. Traumatic hernia: two cases of traumatic subcutaneous rupture of the abdominal wall. Acta Chir Scand. 1965;130:256–258. [Google Scholar]
- 13.Pendl G. Traumatische subkutane zerreibung der bauchwand mit intestinalprolaps. Zentralbl Chir. 1970;95:903–904. [PubMed] [Google Scholar]
- 14.Herbert RJ, Turner FW. Traumatic abdominal wall hernia in a 7-year-old child. J Pediatr Surg. 1973;8:975–976. doi: 10.1016/0022-3468(73)90032-8. [DOI] [PubMed] [Google Scholar]
- 15.Atiemo EA, Goswami G. Traumatic ventral hernia. J Trauma. 1974;14:181–182. doi: 10.1097/00005373-197402000-00011. [DOI] [PubMed] [Google Scholar]
- 16.Hollwarth M. Die traumatische bauchwandhernie im kindersalter. Chirurg. 1977;48:592–594. [PubMed] [Google Scholar]
- 17.Dreyfuss DC, Flancbaum L, Krasna IH, Tell B, Trooskin SZ. Acute trans-rectus traumatic hernia. J Trauma. 1986;26:1134–1136. doi: 10.1097/00005373-198612000-00016. [DOI] [PubMed] [Google Scholar]
- 18.Schneegans VHJ. Geschlossene traumatische bauchwandruptur. Zentralbl Chir. 1988;113:544–545. [PubMed] [Google Scholar]
- 19.Mitchiner JC. Handlebar hernia: diagnosis by abdominal computed tomography. Ann Emerg Med. 1990;19:812–813. doi: 10.1016/S0196-0644(05)81709-3. [DOI] [PubMed] [Google Scholar]
- 20.Damschen DD, Landercasper J, Cogbill TH, Stolee RT. Acute traumatic abdominal hernia: case reports. J Trauma. 1994;36:273–276. doi: 10.1097/00005373-199402000-00026. [DOI] [PubMed] [Google Scholar]
- 21.Kubalak G. Handlebar hernia: case report and review of the literature. J Trauma. 1994;36:438–439. doi: 10.1097/00005373-199403000-00036. [DOI] [PubMed] [Google Scholar]
- 22.Iuchtman M, Kessel B, Kirshon M. Trauma-related acute spigelian hernia in a child. Pediatr Emerg Care. 1997;13:404–405. doi: 10.1097/00006565-199712000-00013. [DOI] [PubMed] [Google Scholar]
- 23.Perez VM, McDonald AD, Ghani A, Bleacher JH. Handlebar hernia: a rare traumatic abdominal wall hernia. J Trauma. 1998;44:568. doi: 10.1097/00005373-199803000-00032. [DOI] [PubMed] [Google Scholar]
- 24.Goliath J, Mittal V, McDonough J. Traumatic handlebar hernia: a rare abdominal wall hernia. J Pediatr Surg. 2004;39:e20–e22. doi: 10.1016/j.jpedsurg.2004.06.039. [DOI] [PubMed] [Google Scholar]