

Abstract
Aim:
To compare the difference in microleakage values using conventional and new low-shrink Silorane composites using the dye penetration method.
Background:
With improvement in adhesive technology, problems associated with composites have been largely overcome. However, microleakage due to polymerization shrinkage still remains a challenge. New Silorane-based composites are alleged to have less than 1% polymerization shrinkage, which would potentially decrease the microleakage, and hence, resolve this longstanding issue.
Materials and Methods:
The teeth were randomly divided into three groups (A,B, and C). Group A was restored with conventional composite (Valux™ Plus), with a total-etch protocol, Group B was restored with conventional composite, with a self-etch protocol, and group C were restored with a silorane-based composite (Filtek TMP90). Thermocycling at 200 cycles between 5 and 55°C ± 2°C with a dwell time of 60 seconds was conducted. The teeth were stained with methylene blue dye and then sectioned and viewed under a dissection microscope, afer which the microleakage was evaluated.
Results:
The interexaminer reliability was evaluated using the kappa score, which was acceptable (61 – 78%). The total-etch group performed statistically and significantly better (P < 0.001) at the occlusal margin and was marginally and statistically significant (P = 0.05) at the gingival margin compared to the self-etch conventional and Silorane groups.
Conclusions:
The Silorane composite did not perform better than the conventional composites, however, it may have its uses and requires further research.
Keywords: Class V cavity, dye penetration, microleakage, silorane
INTRODUCTION
Disadvantages associated with using composites are usually a direct or indirect result of polymerization shrinkage. As the polymerization process starts, most of the monomer is converted into polymer and the final bulk of the composite shrinks approximately two-to-three percent in terms of volume.[1] On account of the polymerization shrinkage, stresses are generated within the restoration and at the margins, and if these stresses exceed the bond strength gap formation, microleakage may occur at the tooth restoration interface,[2] which may cause ingress of cariogenic bacteria, postoperative sensitivity, and secondary caries, subsequently leading to a replacement of the restoration or even endodontic therapy.[3]
There are several methods that may be advocated to reduce polymerization shrinkage, which is an area of continuous research. In recent times, several attempts to reduce shrinkage by changing the nature of the resin have demonstrated that bicyclic compounds cured by ring opening polymerization tend to shrink less as they harden.[4]
The earliest attempts at this were made by Bowen. Similarly spiro-orthocarbonates were developed, which underwent ring opening and produced an expansion of about 3.5%, which could offset shrinkage. However, they exhibited incomplete ring opening and minimal copolymerization, which resulted in a minimal reduction of shrinkage.[4]
Of late, 3M ESPE has introduced a newer monomer, which, when activated, undergoes a cationic ring opening. This monomer, ‘Silorane,’ is made up of ‘siloxane’and ‘oxiranes,’ and these materials are claimed to have less then 1% volumetric shrinkage.[5] In addition to the improved marginal integrity at both the enamel and dentin interfaces, the inventors have claimed improved biocompatibility and increased hydrophobicity when compared to methacrylates, as also a decreased mutagenic potential of Silorane when compared to Oxiranes.[6]
The aim of our study was to compare the microleakage scores obtained by the new silorane material compared to the hybrid composites, while using different etching and bonding protocols. We tested the hypothesis that a decrease in polymerization shrinkage of a Silorane composite would lead to lower microleakage scores at the tooth restoration interface.
MATERIALS AND METHODS
Sample size
Sixty-three teeth were divided into groups, with a total of 21 teeth in each group; however, due to procedural error 20 teeth were included in group A, 20 in Group B, and 15 in Group C.
Sampling technique
Random selection: The teeth, after being selected with respect to the inclusion and exclusion criteria, were randomly distributed into three boxes , labeled A, B, and C. The operator blindly picked one tooth from the selected lot each time and put them in each box, respectively.
Random assignment: Each box was assigned one treatment group. Each group (Groups A,B, and C) was assigned one restorative material. This was done by a random draw performed by a colleague, who was not related to the study.
Sample selection
Inclusion criteria:
Noncarious human premolars extracted for orthodontic or periodontal reasons.
Exclusion criteria:
Previously cervically restored teeth.
Teeth with visible cracks.
Data collection procedure
Teeth selection and preparation
Sixty-three teeth, which fitted our inclusion criteria were selected. Teeth with previous cervical restorations or visible cracks were to be excluded, but we did not come across any teeth falling into that category. The teeth were scrubbed and soaked in hypochlorite for disinfection and then stored in distilled water to prevent dehydration.
Cavity preparation
Standardized Class V cavities were prepared on the buccal surface of each tooth at the cementoenamel junction using a tapered fissure carbide burr (FG 700,SS White) in a high speed handpiece, with an air/water spray. The preparation was 4 mm in length, 3 mm wide mesiodistally, and 2 mm deep, with an occlusal margin in enamel and a gingival margin in dentin. The same operator (principal investigator) performed all the cavity preparations and restorations to eliminate interoperator variability.
Groups in study
After cavity preparations, the teeth in each group were assigned numbers and were randomly assigned into three treatment Groups (A, B, and C). Group A received the total-etch protocol and was restored with composite resin. Group B received the self-etch protocol and was restored with composite resin. Group C received the self-etch protocol and was restored with the Silorane composite. Details of the materials used are given in Appendix1.
Appendix 1.

Restoration
All the restorations were placed according to the manufacturers instructions, using the incremental placement technique (increment not more than 2 mm), and were cured using the light-emitting diode (LED) light (EliparTM free light 2, 3M ESPE), output 1000 – 1500 mW/cm2, for 40 seconds. All the restorations were then finished with a graded series of aluminum oxide disks (Sof-Lex TM, 3M ESPE). After restoration, the teeth were sectioned into dental blocks from the crowns of the buccal surface of the tooth, with approximate dimensions of 5 × 5 × 6 mm3, using a slow speed diamond disk (Diamond disk, Microdont).
All the teeth were thermocycled (Eppendorf Mastercycler Gradient). The cycles were set at 200 cycles, between 5 and 55°C ± 2°C, with a dwell time of 60 seconds at each temperature. All the specimens were then sealed with a coating of nail polish (Etude,Shade: coffe brown), except margins of 1 mm around the restorations. and immersed in 2% methylene blue dye for 24 hours. The teeth were then washed under running water and dried.
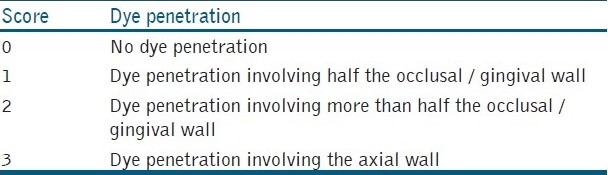
The teeth were mounted on a stone cast in such an orientation that the occlusal surface was visible outside the plaster. The teeth in the mounted cast were sectioned longitudinally in a buccolingual direction through the center of the restoration with a slow speed diamond disk (Diamond disk, Microdont). The cut surfaces were then examined under a dissection microscope (Inverted Microscope)(OLYMPUS SZ×12)at 40 X magnification. The dye penetration in the specimens was evaluated for both the occlusal and gingival surfaces, based on the graded scoring system given in Table 1. Each sample was observed by two examiners and noted separately.
Table 1.
Microleakage scores
RESULTS
All the data were gathered using statistical package for social sciences (SPSS) version 16.0. The interexaminer reliability (as determined by the kappa scores) was acceptable to good (61 –78%, as shown in Table 2).
Table 2.
Interexaminer reliability scores
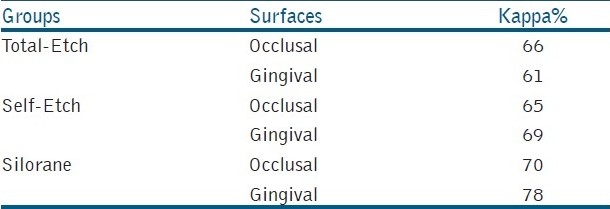
The Kappa statistic was applied at a 0.05 level of significance
For the occlusal surfaces, the conventional total-etch composites demonstrated the least microleakage, while the Silorane and self-etch composites had higher microleakage scores. The difference in microleakage scores among these groups was statistically and highly significant, [Table 3].
The Kruskal-Wallis test was applied to determine the difference between microleakage scores (ordinal data) in the three study groups at a 0.05 level of significance
For the gingival surfaces, the conventional total-etch composites demonstrated the least microleakage, while the Silorane and self-etch composites had relatively higher microleakage scores. The difference in microleakage scores among these groups was statistically and marginally significant, [Table 4].
Table 3.
Microleakage scores observed in occlusal surfaces using the three protocols

Table 4.
Microleakage scores observed in gingival surfaces using the three protocols

The Kruskal-Wallis test was applied to determine the difference between microleakage scores (ordinal data) in the three study groups at a 0.05 level of significance
DISCUSSION
In our study, the class V cavity design was chosen because it had a high C-factor value. It was relatively easy to restore and therefore minimized interoperator variability. It had both enamel and dentinal margins and did not offer any inherent macro-mechanical retention.[7]
The samples were subjected to thermocycling in order to replicate the intraoral environment, because there was a difference in the coefficient of thermal expansion of the restoration and the tooth interface. The resulting mismatch in its value was said to cause fatigue of the bond between the restoration and the tooth, leading to a gap formation, which could lead to microleakage.[8]
The two main established methods that are usually used to study marginal gaps are either dye penetration or scanning electron microscopy (SEM). In dye penetration testing, which is one of the main methods of assessing microleakage, the sample is subjected to a dye marker such as methylene blue, basic fuchsin silver nitrate, and rarely india ink; however, concerns have been raised, especially in the case of dye penetration, as there is lack of evidence supporting any correlation between clinical testing and in vitro dye penetration testing.[9] Similarly, SEM requires that the sample be subjected to extensive chemical preparations before the scanning process and this may lead to alteration or even destruction of the interfacial zones, and even underestimation of the actual thickness of the hybrid layer.[10,11]
As the Silorane-based composites are highly hydrophobic, they are not compatible with the conventional adhesive systems, and require a separate primer and bond. The primer is hydrophilic and the bond consists of a hydrophobic bi-functional monomer, to make it compatible with the hydrophobic silorane. As the primer consists of an etching monomer, which is usually cured before the application of the bond, it may be considered and therefore compared with other one-step adhesive systems. This is the reason we have used a one-step, self-etch adhesive as the control, as well as used the total-etch approach, to make our groups more comparable.[10]
In our study we found that the total-etch and conventional composite groups had less microleakage scores as compared to the self-etch protocol that we used in both the Silorane-based as well as hybrid composites. This could be explained by the hydrophilic nature of the self-etching adhesives,[12] as our samples were subjected to a 24-hour dye penetration challenge. It was hypothesized that this extended dye penetration would have led to increased water as well as dye absorption, resulting in a stained adhesive layer, compared to etching and rinsing with a less hydrophilic adhesive. This could have led to more false negative results in our case, as the stained layer could have been interpreted as gaps causing the microleakage.
To counter this potential challenge it has been recommended that either an adhesive with the same hydrophilicity be compared when performing dye penetration or the dye penetration time be reduced. This short penetration time will decrease the potential of the dye staining the hydrophilic adhesive.[13]
Another possible explanation could be that as the Silorane primer is cured before the application of the bond an oxygen inhibition layer is formed between the primer and the bond interface and is seen in the Micro-Raman Spectroscopy as a zone of circa 1 um. This zone may also be a potential weakness in the bonding of Silorane and warrants further studies.[10]
A study was conducted to compare the Silorane restorative system with the self-etch adhesive in combination with a hybrid composite, and they found poor marginal integrity of the Silorane-based composite in both the enamel and dentinal margins; similar results are seen in our study.[11]
However, Bagis YH , Baltacioglu IH, and Kahvagullaris S[14] compared the effect of different layering methods and different composite materials (nano-hybrid composites and Silorane-based micro-hybrid composites) on the extracted third molars, using the MOD (mesio-occluso-distal) cavity design. The authors did not observe any microleakage. The results were contradictory to our observations in which we observed significant microleakage in our Silorane-based group. These results could be explained by the in vitro study done on maxillary premolars in which the authors tested both cuspal deflection and microleakage on the low-shrink dental composites. The authors concluded that the significant decrease in microleakage observed in the Silorane-based composite was due to the decrease in cuspal deflection, which usually occurred in teeth that had weakened due to extensive MOD cavities, due to polymerization shrinkage stress at the tooth restoration interface. However, as the Class V cavities had not weakened and there was no deflection of the cavity walls, the reduced amount of polymerization of Silorane might have been very modest if there had been any effect in such cavities.[6]
Similarly a randomized clinical trial was carried out, to study the marginal adaptation of Silorane compared to a methacrylate-based composite. The authors did not find any significant difference between the two materials.[15]
To our knowledge, literature is lacking in secondary studies such as systematic reviews, when it comes to low shrink composites, and warrants that one must be done.
No studies known to us have evaluated microleakage using the dye penetration method when studying Silorane composites, as most of the research is targeted at evaluating marginal adaptation. This research will add to the body of knowledge that is already present on Silorane composites. This research also questions the benefit of materials with low volumetric polymerization shrinkage, which should not be considered as the only parameter for decreasing stress, and other factors such as modulus of elasticity must also be kept in mind.
In summary, the results of our study do not indicate that Silorane-based composites are better than the conventional composites in terms of microleakage. We have also found poor sealing ability at the dentin or cementum margins compared to the enamel margins, in all the groups; a finding which is in accordance with other studies.[16,17] The total-etch group has performed better than the self-etch groups in both the enamel and dentin / cementum margins, which is also seen in other studies.[18]
Strengths
The study questions and addresses a very important topic, relevant to everyday practice, as it relates to the longevity of a restoration. The data collection method that has been used is a validated method and the literature is full of studies with similar methodologies.[17]
It is an in vitro clinical trial where intervention is performed on three groups simultaneously, resulting in data that is comparable within the groups. An appropriate statistical test, Kruskall-Wallis, has been applied to determine the microleakage scores, as the data is qualitative and ordinal.
Limitation
The Kappa statistic did not show very good interexaminer reliability, highlighting the subjective nature of evaluation of the microleakage when using the dye penetration method. As it was an in vitro study, its results would not necessarily translate to clinical practice, as the studies have found a very weak correlation between in vitro and clinical trials, and therefore, continuation in the form of clinical trials is required, to make clinically relevant conclusions.[19]
CONCLUSIONS
The Silorane-based composite materials have not shown complete elimination of the microleakage values, although they may have their uses. However, further studies, especially in vivo studies, are required to draw clinically relevant conclusions.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Burke FJ, Shortall AC. Successful restoration of load-bearing cavities in posterior teeth with direct-replacement resin-based composite. (96,98).Dent Update. 2001;28:388–94. doi: 10.12968/denu.2001.28.8.388. [DOI] [PubMed] [Google Scholar]
- 2.De Almeida JB, Platt JA, Oshida Y, Moore BK, Cochran MA, Eckert GJ. Three different methods to evaluate microleakage of packable composites in Class II restorations. Oper Dent. 2003;28:453–60. [PubMed] [Google Scholar]
- 3.Shenoy A. Is it the end of the road for dental amalgam? A critical review. J Conserv Dent. 2008;11:99–107. doi: 10.4103/0972-0707.45247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Malhotra N, Kundabala M, Shashirashmi A. Strategies to overcome polymerization shrinkage--materials and techniques. A review. Dental update. 2010;37:115–8. doi: 10.12968/denu.2010.37.2.115. [DOI] [PubMed] [Google Scholar]
- 5.Weinmann W, Thalacker C, Guggenberger R. Siloranes in dental composites. Dent Mater. 2005;21:68–74. doi: 10.1016/j.dental.2004.10.007. [DOI] [PubMed] [Google Scholar]
- 6.Palin WM, Fleming GJ, Nathwani H, Burke FJ, Randall RC. In vitro cuspal deflection and microleakage of maxillary premolars restored with novel low-shrink dental composites. Dent Mater. 2005;21:324–35. doi: 10.1016/j.dental.2004.05.005. [DOI] [PubMed] [Google Scholar]
- 7.Ritter AV, Swift EJ, Jr, Heymann HO, Sturdevant JR, Wilder AD., Jr An eight-year clinical evaluation of filled and unfilled one-bottle dental adhesives. J Am Dent Assoc. 2009;140:28–37. doi: 10.14219/jada.archive.2009.0015. [DOI] [PubMed] [Google Scholar]
- 8.Wahab FK, Shaini FJ, Morgano SM. The effect of thermocycling on microleakage of several commercially available composite Class V restorations in vitro. J Prosthet Dent. 2003;90:168–74. doi: 10.1016/s0022-3913(03)00300-7. [DOI] [PubMed] [Google Scholar]
- 9.Heintze SD. Systematic reviews: I. The correlation between laboratory tests on marginal quality and bond strength. II. The correlation between marginal quality and clinical outcome. J Adhes Dent. 2007;9:77–106. [PubMed] [Google Scholar]
- 10.Santini A, Miletic V. Comparison of the hybrid layer formed by Silorane adhesive, one-step self-etch and etch and rinse systems using confocal micro-Raman spectroscopy and SEM. J Dent. 2008;36:683–91. doi: 10.1016/j.jdent.2008.04.016. [DOI] [PubMed] [Google Scholar]
- 11.Ernst CP, Galler P, Willershausen B, Haller B. Marginal integrity of class V restorations: SEM versus dye penetration. Dent Mater. 2008;24:319–27. doi: 10.1016/j.dental.2007.06.002. [DOI] [PubMed] [Google Scholar]
- 12.Ito S, Hashimoto M, Wadgaonkar B, Svizero N, Carvalho RM, Yiu C, et al. Effects of resin hydrophilicity on water sorption and changes in modulus of elasticity. Biomaterials. 2005;26:6449–59. doi: 10.1016/j.biomaterials.2005.04.052. [DOI] [PubMed] [Google Scholar]
- 13.Ernsta CP, Kotter T, Victor A, Canbek K, Brandenbusch M, Willershausen B. Marginal integrity of self- and total-etching adhesives in two different application protocols. J Adhes Dent. 2004;6:25–32. [PubMed] [Google Scholar]
- 14.Bagis YH, Baltacioglu IH, Kahyaogullari S. Comparing microleakage and the layering methods of silorane-based resin composite in wide Class II MOD cavities. Oper Dent. 2009;34:578–85. doi: 10.2341/08-073-LR. [DOI] [PubMed] [Google Scholar]
- 15.Schmidt M, Kirkevang LL, Horsted-Bindslev P, Poulsen S. Marginal adaptation of a low-shrinkage silorane-based composite: 1-year randomized clinical trial. Clin Oral Investig. 2010;20 doi: 10.1007/s00784-010-0446-2. [In Press] [DOI] [PubMed] [Google Scholar]
- 16.Castelnuovo J, Tjan AH, Liu P. Microleakage of multi-step and simplified-step bonding systems. Am J Dent. 1996;9:245–8. [PubMed] [Google Scholar]
- 17.Hegde MN, Vyapaka P, Shetty S. A comparative evaluation of microleakage of three different newer direct composite resins using a self etching primer in class V cavities: An in vitro study. J Conserv Dent. 2009;12:160–3. doi: 10.4103/0972-0707.58340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Küçükemen Ç, Sönmez H. Microleakage of Class-V composite restorations with different bonding systems on fluorosed teeth. Eur J Dent. 2008;2:48–58. [PMC free article] [PubMed] [Google Scholar]
- 19.Heintze SD, Blunck U, Göhring TN, Rousson V. Marginal adaptation in vitro and clinical outcome of class V restorations. Dent Mater. 2009;25:605–20. doi: 10.1016/j.dental.2008.11.004. [DOI] [PubMed] [Google Scholar]