

Abstract
Aim:
Light-emitting diode light curing units (LED LCUs) have become more popular than halogen LCUs in routine dental restorative treatment. The aim of the study was to compare the effects of two conventional halogen (Hilux Plus and VIP) and two LED (Elipar FreeLight 2 and Smart Lite) light curing units on the depth of cure and the microhardness of various esthetic restorative materials.
Materials and Methods:
The curing depth and microhardness of a compomer (Dyract Extra), a resin-modified glass ionomer (Vitremer), a packable composite (Sculpt It), an ormocer (Admira), a hybrid composite (Tetric Ceram), two microhybrid composites (Miris and Clearfil Photo Posterior) and, a nanofil composite (Filtek Supreme) were determined using a scraping method and a hardness tester. A total of 320 samples were prepared using the eight different materials (n = 10 samples for each subgroup). The scraping test was based on ISO 4049:2000. Vicker's microhardness testing was carried out using hardness tester (Zwick 3212). Data were analyzed using one-way analysis of variance (ANOVA), Bonferroni and the Kolmogorov–Smirnov tests.
Results:
Best microhardness results were obtained with the LED light curing units and Tetric EvoCeram and Filtek Supreme achieved the highest hardness values. The nanofil composite, Filtek Supreme, showed the best curing depth results in all the tested light curing systems.
Conclusions:
The LEDs were found to be more successful than the halogen units with respect to both curing depth and microhardness properties.
Keywords: Composite, curing depth, halogen light curing, led light curing, microhardness
INTRODUCTION
The use of light-activated resin composites in restorative dentistry has grown dramatically in recent years. There are currently a range of photo-polymerization techniques which have advantages and disadvantages with respect to the properties of the final restoration and of the long-term status of the restored teeth. Inadequate polymerization has been associated with loss of biocompatibility, color change, retention loss, breakage, excessive wear, and restoration softness. Many visible light-activated composite resins use diketone photoinitiators such as camphorquinone.[1] The relationship between the spectral distribution of the output from the light curing sources and the maximum absorption of the photoinitiator is expected to have effects on the physical properties of the cured composite.[2,3]
In addition, some dental composites are not convenient to light-emitting diode (LED) curing technology. The spectra of the LED light curing units (LCUs) differ from those of halogen units. The photoinitiator systems of some composites need to be adjusted to the spectra of these new light sources.[2–4]
Halogen LCUs are currently the most commonly used for curing of dental composites, but this technology has several drawbacks. Halogen bulbs have a limited lifespan, and with passage of time, the bulbs, reflectors and filters degrade due to their high operating temperatures resulting in a reduction of their curing effectiveness. To overcome these shortcomings, LED technology has been proposed for the use of light curing dental materials.[5–7] The spectral output of blue LEDs falls conveniently within the absorption spectrum of the camphorquinone photoinitiator (400–500 nm), and so no filters are required when LED LCUs are used. Furthermore, LED LCUs have an expected lifetime of several thousand hours without significant degradation of light flux.[8] LED units generate minimal heat and so do not require cooling fans which have associated noise and power consumption. The efficiency of conversion of electrical energy to useable curing energy is higher for blue LEDs than for conventional halogen lamps (14% vs. 1%, respectively). In halogen lamps, up to 70% of the input power is converted to heat, with only 10% resulting in visible light. Of this visible light, a further 90% is lost due to the use of cut-off filters. Ultimately, their blue light output makes up only 1% of the total energy input.[9–11]
Hardness evaluation is a widely used test for the investigation of composite curing and of the efficiency of light sources.[2,12–14] Comparative measurements of arrays composed of different LEDs and conventional halogen lamps enable the determination of the operating conditions required for equivalent or superior hardness result.[15–17]
Our first hypothesis was that the two LED LCUs can have a better curing performance than halogen LCUs. Our second hypothesis was that the type of the curing units affects the depth of cure.
The aims of this study were to evaluate the performances of two LED curing lights and to compare them with those of two conventional halogen lights according to determine the microhardness and depth of tooth colored restoratives.
MATERIALS AND METHODS
The restorative materials investigated in this study were a compomer (Dyract Extra; Dentsply DeTrey, Konstanz, Germany), a resin-modified glass ionomer (Vitremer; 3M ESPE, Seefeld, Germany), a packable composite (Sculpt It; Jeneric/Pentron Inc., Wallingford, CT, USA), an ormocer (Admira; VOCO, Cuxhaven, Germany), a hybrid composite (Tetric EvoCeram; Ivoclar Vivadent, Schaan, Liechtenstein), two microhybrid composites (Miris; Coltene/Whaledent, Switzerland, and Clearfil Photo Posterior; Kuraray Medical Inc., Kurashiki, Okuyama, Japan), and a nanofil composite (Filtek Supreme; 3M ESPE St. Paul, MN, USA).
All the samples (N = 320) were prepared in a cylindrical stainless steel mold (Ø 4 mm and H 10 mm) placed on a dark polyvinyl chloride (PVC) background covered with a celluloid matrix strip. The top of the mold was covered with a celluloid matrix strip and the excess material was removed by pressing a glass slide against the strip. Then, the glass plate was removed and the light tip of the curing unit was positioned concentrically within the cavity in the mold, 0.5 mm above the sample. The curing units used in the polymerizations of the restorative materials were two conventional halogen lights (Hilux Plus, Benlioglu Dent., Ankara, Turkey and VIP, BISCO, Inc., Illinois, USA) and two LED LCUs (Elipar FreeLight 2, 3M ESPE, and Smart Lite, DENTSPLY). Each unit was used in continuous cure mode with a full battery charge. For all four units, an irradiation time of 40 s was selected. A2 color shade composite from Vitapan Classical tab was chosen for all the tested materials to standardize the polymerization. Light intensity was checked with a handheld digital radiometer (Dental Hilux Curing Light Meter, Dental Benlioglu, Inc., Ankara, Turkey) before the light curing. The outputs of the curing lights were found to be 450 mW/cm2 (Hilux), 470 mW/cm2 (Elipar FreeLight), 460 mW/cm2 (Smart Lite), and 450 mW/cm2 (VIP). The curing time used for each LED and halogen LCU was 40 s. For each curing unit, 10 samples of each material were tested. The curing depth was determined using a scraping test based on ISO 4049:2000. In the scraping test, each sample was removed from the mold, 1 minute after the end of the irradiation and the soft uncured material at the bottom of the sample was gently scraped off with a plastic spatula. The length of the remaining material was measured with a micrometer (Mitutoyo 551-201-20, Mitutoyo Corp., Kawasaki, Japan) with a reading accuracy of 0.001 mm and the result divided by two. Each material was measured three times and the mean value of these readings was accepted as resulting value of the curing depth.
Measurements of the Vicker's surface microhardness were carried out at the top of the cured samples using Zwick 3212 hardness tester (Zwick, Ulm, Germany). Each specimen was subjected to three indentations under a 50 g load for 30 s at randomly selected locations and the average of these three measurements was calculated. Statistical analysis of the data was performed using one-way analysis of variance (ANOVA) post-hoc pairwise multiple comparisons, Bonferroni test and the Kolmogorov-Smirnov test.
RESULTS
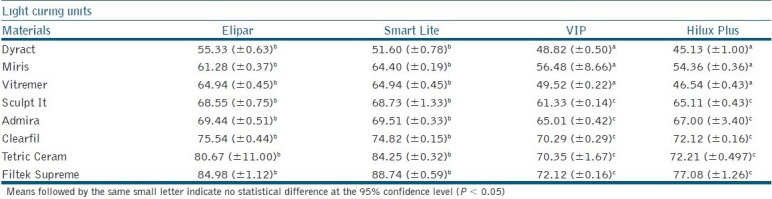
The mean values and standard deviations of the curing depth and microhardness of restorative materials and LCUs are summarized in Tables 1 and 2, respectively. No statistically significant differences were found with the scraping test between the two LED curing units for Dyract Extra, Miris, Sculpt It, and Tetric EvoCeram (P > 0.05). For Elipar and Smart Lite, significantly higher microhardness values were achieved compared to halogen LCUs (P < 0.05). The nanofil composite, Filtek Supreme, showed the best curing depth values with all of the tested light curing systems. When polymerized with the VIP and Hilux light curing units, Dyract Extra, Vitremer, and Miris were found to exhibit significantly lower microhardness than the other materials (P < 0.05). These materials also provided lower values with the LED LCUs. The best microhardness results were obtained with LED light curing units, and Filtek Supreme and Tetric EvoCeram exhibited higher hardness values than the other materials.
Table 1.
Mean curing depth values of restorative materials polymerized with different light curing units (mm)
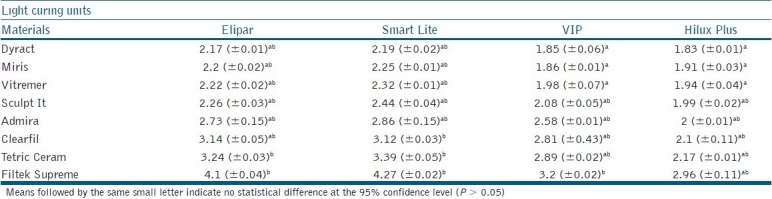
Table 2.
Mean microhardess values of restorative materials for different light curing units (Vicker's hardness, VHN)
DISCUSSION
The depth of cure and microhardness of the resin composite materials were assessed as these are considered to be the essential physical properties. These are relevant to the clinical technique of incremental packing and curing.[13] Microhardness evaluation is widely used for testing the assessment of composite curing, and thus, the efficiency of light sources.[18,19]
Oberholzer reported that the results for the microhardness of restorations are significantly lower for halogen lights than for LED units.[20]
Hubbezoglu examined the surface microhardness of four kinds of resin composites with various fillers and resin matrices of the materials tested. The nanofilled resin composite was found to exhibit the highest microhardness values for each curing regime.[21] Our results coincide with those of the study by Hubbezoglu, which support our findings, and highest microhardness values were obtained with Filtek Supreme. Koupis[22] reported that the reduction of the curing depth for shade A4 compared to A2 depends quantitatively on the formulation of the material. In this study, restorative materials of A2 shade were selected to minimize the effects of colorants on the light polymerization.
Our first hypothesis was that the two LED LCUs can have a better curing performance than halogen LCUs. In this study, the halogen lamps were found to exhibit irradiance near 460 nm and the LED LCUs at approximately 470 nm, which better matches the most efficient wavelength for activation of the camphorquinone present in the resin. These findings confirm our hypothesis. The scraping depth results can be explained by relating the emission wavelengths of the curing source to the absorption spectrum of camphorquinone, which has its peak absorption near 470 nm. The curing depth depends on the penetration of the curing light into the composite.[23] It must be noted that the scraping depth results are dependent on the specific excitation peak of camphorquinone. Composites with initiator systems absorbing light in the visible range have been introduced. In addition to the standard visible light photoinitiator, camphorquinone, some manufacturers use a co-initiator that absorbs light at shorter wavelengths.[24,25]
Our second hypothesis was that the type of the curing units affects the depth of cure. Of all the materials tested, Filtek Supreme produced the greatest values of curing depth, while the highest microhardness values were obtained with Tetric EvoCeram and Filtek Supreme. Filtek Supreme has a high translucent filler content that allows superior transmission of light through the matrix. The findings supported our hypothesis. Increasing the filler eventually leads to increase in the surface microhardness of the composite. Since the compomer and polyacid modified composites have much lower filler contents of a different type, they produce lower surface microhardness after curing. Our results are in accordance with those of other studies.[10,23–25]
CONCLUSIONS
We conclude that LED LCUs are found to be more successful than the halogen units with respect to both curing depth and microhardness properties. LED LCUs could be the best alternative light curing device for microhardness and depth of cure on the dental composite polymerization.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Asmussen E, Peutzfeldt A. Influence of pulse-delay curing on softening of polymer structures. J Dent Res. 2001;80:1570–3. doi: 10.1177/00220345010800061801. [DOI] [PubMed] [Google Scholar]
- 2.Asmussen E, Peutzfeldt A. Light-emitting diode curing: Influence on selected properties of resin composites. Quintessence Int. 2003;34:71–5. [PubMed] [Google Scholar]
- 3.Rueggeberg FA, Caughman WF, Curtis JW, Davis HC. Factors affecting cure at depths within light-activated resin composites. Am J Dent. 1993;6:91–5. [PubMed] [Google Scholar]
- 4.Uhl A, Mills RW, Jandt KD. Polymerization and light-induced heat of dental composites cured with LED and halogen technology. Biomaterials. 2003;24:1809–20. doi: 10.1016/s0142-9612(02)00585-9. [DOI] [PubMed] [Google Scholar]
- 5.Park YJ, Chae KH, Rawls HR. Development of a new photoinitiation system for dental light-cure composite resins. Dent Mater. 1999;15:120–7. doi: 10.1016/s0109-5641(99)00021-4. [DOI] [PubMed] [Google Scholar]
- 6.Rueggeberg FA, Blalock JS, Callan RS. LED curing lights-what's new? (588,580-91).Compend Contin Educ Dent. 2005;26:586. [PubMed] [Google Scholar]
- 7.Tsai PC, Meyers IA, Walsh LJ. Depth of cure and surface microhardness of composite resin cured with blue LED curing lights. Dent Mater. 2004;20:364–9. doi: 10.1016/S0109-5641(03)00130-1. [DOI] [PubMed] [Google Scholar]
- 8.Mills RW, Uhl A, Blackwell G, Jandt KD. High power light emitting (LED) arrays versus halogen light light polymerization of oral biomaterials.Barcol hardness, compressive strength and radiometric properties. Biomaterials. 2002;23:2955–63. doi: 10.1016/s0142-9612(02)00024-8. [DOI] [PubMed] [Google Scholar]
- 9.Price RB, Ehrnford L, Andreou P, Felix CA. Comparison of quartz-tungsten-halogen, light-emitting diode, and plasma arc curing lights. J Adhes Dent. 2003;5:193–7. [PubMed] [Google Scholar]
- 10.Mills RW, Jandt KD, Ashworth SH. Dental composite depth of cure with halogen and blue light emitting diode technology. Br Dent J. 1999;186:388–91. doi: 10.1038/sj.bdj.4800120. [DOI] [PubMed] [Google Scholar]
- 11.Rueggeberg FA, Ergle JW, Mettenburg DJ. Polymerization depths of contemporary light-curing units using microhardness. J Esthet Dent. 2000;12:340–9. doi: 10.1111/j.1708-8240.2000.tb00243.x. [DOI] [PubMed] [Google Scholar]
- 12.Dunn WJ, Bush AC. A comparison of polymerization by light-emitting diode and halogen-based light-curing units. J Am Dent Assoc. 2002;133:335–41. doi: 10.14219/jada.archive.2002.0173. [DOI] [PubMed] [Google Scholar]
- 13.Hansen EK, Asmussen E. Correlation between depth of cure and surface hardness of light-activeted resin. Scand J Dent Res. 1993;101:62–4. doi: 10.1111/j.1600-0722.1993.tb01649.x. [DOI] [PubMed] [Google Scholar]
- 14.Orla C, Ray NJ, Lynch CD, Burke FM, Hannigan A. In vitro study of surface microhardness of a resin composite exposed to a quartz-halogen lamp. Quintessence Int. 2004;35:795–800. [PubMed] [Google Scholar]
- 15.Deb S, Sehmi HA. Comparative study of the properties of dental resin composites polymerized with plasma and halogen light. Dent Mater. 2003;19:517–22. doi: 10.1016/s0109-5641(02)00099-4. [DOI] [PubMed] [Google Scholar]
- 16.Kurachi C, Aparecida AM, Magalhaes DV, Bagnato SG. Hardness evaluation of a dental composite polymerized with experimental LED-based devices. Dent Mater. 2001;17:309–15. doi: 10.1016/s0109-5641(00)00088-9. [DOI] [PubMed] [Google Scholar]
- 17.Ramp LC, Broome JC, Ramp MH. Hardness and wear resistance of two resin composites cured with equivalent radiant exposure from a low irradiance LED and QTH light-curing units. Am J Dent. 2006;19:31–6. [PubMed] [Google Scholar]
- 18.Polydorou O, Manolakis A, Hellwig E, Hahn P. Evaluation of the curing depth of two translucent composite materials using a halogen and two LED curing units. Clin Oral Investig. 2008;12:45–51. doi: 10.1007/s00784-007-0142-z. [DOI] [PubMed] [Google Scholar]
- 19.Soh MS, Yap AU, Siow KS. Effectiveness of composite cure associated with different curing modes of LED lights. Oper Dent. 2003;28:371–7. [PubMed] [Google Scholar]
- 20.Oberholzer TG, Preez DI, Kidd M. Effect of LED curing on the microleakage, shear bond strength and surface hardness of a resin-based composite restoration. Biomaterials. 2005;26:3981–6. doi: 10.1016/j.biomaterials.2004.10.003. [DOI] [PubMed] [Google Scholar]
- 21.Hubbezoğlu I, Bolayir G, Doğan OM, Doğan A, Ozer A, Bek B. Microhardness evaluation of resin composites polymerized by three different light sources. Dent Mater J. 2007;26:845–53. [PubMed] [Google Scholar]
- 22.Koupis NS, Vercruysse CW, Marks LA, Martens LC, Verbeeck RM. Curing depth of (polyacid-modified) composite resins determined by scraping and a penetrometer. Dent Mater. 2004;20:908–14. doi: 10.1016/j.dental.2004.01.001. [DOI] [PubMed] [Google Scholar]
- 23.Soh MS, Yap AU, Siow KS. The effectiveness of cure of LED and halogen curing lights at varying cavity depths. Oper Dent. 2003;28:707–15. [PubMed] [Google Scholar]
- 24.Soh MS, Yap AU, Siow KS. Comparative depths of cure among various curing light types and methods. Oper Dent. 2004;29:9–15. [PubMed] [Google Scholar]
- 25.Uhl A, Michaelis C, Mills RW, Jandt KD. The influence of storage and indenter load on the Knoop hardness of dental composites polymerized with LED and halogen technologies. Dent Mater. 2004;20:21–8. doi: 10.1016/s0109-5641(03)00054-x. [DOI] [PubMed] [Google Scholar]