

Abstract
The contribution of researchers from India in the field of electroconvulsive therapy (ECT) has been substantial. Over 250 papers have been published by authors from India in the past five decades on this issue; about half of these have appeared in the Indian Journal of Psychiatry. This article summarizes the papers on ECT research that have appeared in the Journal. A bulk of these articles has focused on establishing the efficacy in different disorders. Considerable numbers of papers describe refinement in the ECT procedure, including anesthetic modification, ECT machine and EEG monitoring. Papers on neurobiology of ECT and long-term follow-up of ECT-treated patients form a minority. Despite the decline in the use of ECT across the globe, papers on ECT have only increased in the recent decades in the Journal.
Keywords: ECT, Research, Indian
INTRODUCTION
Prologue
In this essay we attempt to follow research publications on Electro Convulsive Therapy (ECT), in the Indian Journal of Psychiatry, across the last five decades. We searched the database of the Indian Journal of Psychiatry for ECT research articles. We excluded reviews, orations, editorials and letters. More ECT publications from researchers in India have appeared in the recent 3 decades in other indexed journals (PubMed). Clearly, there is a need to examine all available ECT publications from Indian researchers to understand the present status. In the IJP alone, nearly 90 publications have appeared in the last five decades. Figure 1 clearly indicates a steady rise in ECT publications appearing in IJP over these decades; the number in the last decade alone equals the number of all publications in the first three decades. A national workshop on ECT towards the end of the third decade (1989) may have given an impetus to ECT research that explains a sharp increase in the number of ECT publications. Two Tilak Venkoba Rao oration awards of the Indian Psychiatric Society were published on ECT.
Figure 1.
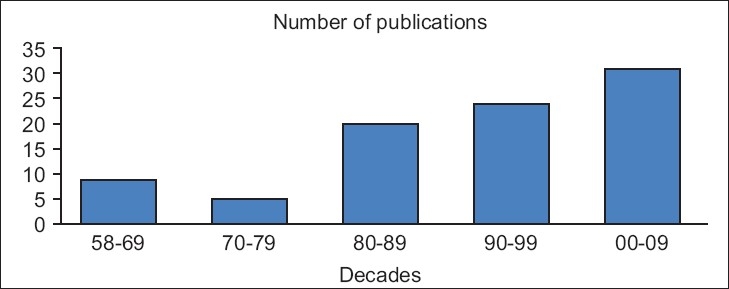
The number of original research papers on electroconvulsive therapy, which appeared in the Indian journal of Psychiatry across five decades
Early trends
Dr. DLN Murthy Rao published the first ever article describing the ectonus method ECT stimulation [Figure 1]. With the development of ECT stimulus machinery, though, this method of stimulation has now become obsolete. Initial reports documented the positive experience of use of ECT in a series of patients of either schizophrenia or manic depressive psychosis. Though ECT was introduced after its success in schizophrenia, the use of ECT in this diagnostic group has now become less frequent. Depression appears to be the most common diagnosis in ECT patients world over; this is not true of India, though. Similarly, researchers recorded the experience with adverse effects of ECT. The observations too were reassuring; the adverse effects were not alarming. Though most ECT services practiced only unmodified ECT for many decades, attempts at studying the role of modifying ECT with some anesthetic medications were published in the initial decade itself. No doubt, this offered a firm foundation for a change in ECT practice towards modified procedures in the later decades (in fact, two of the authors of this paper have not seen unmodified ECT at all).
Electroconvulsive therapy modification
The current practice includes use of anesthesia and muscle relaxant in modified ECT. Researchers explored different ‘anesthetics’ that include thiopentone, propanadid, etomidate, althesin and diazepam. Propanadid demonstrated some advantages over the more commonly used thiopentone in terms of faster recovery and blunted cardiovascular changes during ECT. The advantages did not perhaps outweigh the cost benefits and practical problems like anesthetists’ experience with propanadid that allowed thiopentone to remain the anesthetic of choice in modified ECT. A survey, conducted early in 1990s, indicates that unmodified ECT was the most prevalent practice in ECT. Muscle relaxation is a serious concern that limits modified ECT practice and calls for a more professional anesthesiologist’s attendance. Yet, as early as 1962, Dr. Bagadia used succinylcholine successfully in modified ECT. A method to assess the extent of muscle relaxation-related seizure modification was also developed as a tool for this area of ECT research, though much later (1999).
The relative merits of retaining the unmodified ECT as regards safety compared to the much-advocated modified ECT have been documented. A more recent study supported use of unmodified ECT if enforcing modified procedure discouraged use of ECT itself. This subject attracted comments on the debate of unmodified versus modified ECT.
Efficacy of electroconvulsive therapy
Expectedly, schizophrenia was the first condition tested in comparative trials of ECT. ECT added to the concurrent antipsychotic medication benefitted schizophrenia patients. One observation even noted that ECT conferred ‘protection’ against the drug-induced Parkinsonism. In the days of clozapine, a drug recommended for drug-resistant schizophrenias, ECT got a renewed interest. The former drug has feared side-effects of seizures. However, concurrent ECT in clozapine treated patients has not pointed to such concerns, though some precaution has been suggested in such combinations. When used as a first-line of treatment, ECT may just be as good as conventional doses of a standard antidepressant drug though the latter contributed to more adverse effects. In contrast to the well acclaimed dramatic effects of ECT in catatonia, one research report found that lorazepam produced nearly comparable anti-catatonic effects. Yet, ECT is perhaps the first preferred alternative therapy in catatonia when lorazepam is unsuccessful.
Predictors of electroconvulsive therapy efficacy
Many observations of predictors for response to ECT in depression, noted in standard ECT text books, have been confirmed in independent studies though with some exceptions. The response to the first ECT pointed to a subsequent response in the course for depression. Cardiovascular responses pointed to the potency of the seizure and hence successfully predict the therapeutic efficacy in depression.
Adverse effects
Ever since the introduction of ECT, the concern over adverse effects prompted research and Indian researchers did not fall behind in this clinic-academic venture. The studies included recording of physiological adverse effects on ECG, intraocular pressure as well as structural brain changes using neuroimaging. ECT passed this screening; sophisticated MRI-based neuroimaging studies failed to detect any brain changes acutely following ECT. Yet case reports of unusual side-effects such as catatonia, pneumothorax, CT-scan evidence of brain changes and even death following ECT have appeared in IJP. Traditional herbs may have the benefit of lowering the memory side-effects of ECT. Dr. Andrade even reviewed the molecular mechanisms of ECT-induced amnesia and possible interventions against such adverse effect. Coexisting medical (even neurological) conditions had usually discouraged clinicians from use of ECT. Observations suggest that ECT can be safely used against psychiatric disorders against the odds of a risk associated with concurrent medical condition. However, this may need additional monitoring mechanisms and expertise.
Electroconvulsive therapy stimulus
The first report of ectonus type of stimulus has been mentioned earlier. The stimulus laterality has been explored. Bilateral ECT remains the most popularly used as observed in surveys. A model ECT machine of sine wave type of stimulus was assembled and its scientific description appeared in the IJP. It may be remembered that sine wave ECT stimulus is nearly obsolete. A national workshop on ECT, in 1989, suggested designing of indigenous but state-of-the-art ECT machine with pulse stimulus waveform. Very recently, a comparative review of ECT machines of such stimulus output was reported. The author expressed some concerns and a need for a regulatory body for the standards of ECT device
Monitoring the seizure
Technological advances saw the introduction of EEG monitoring. Initial studies focused on the standardization of EEG monitoring procedures. This included the measurement of ECT seizure duration reliably by noting the change in the seizure morphology. Though EEG monitoring conferred some benefits over mere motor seizure monitoring, the former did not attract ECT practitioners as it carried inherent difficulties, additional expertise, time and cost, to mention a few. Paperless (computer-aided) seizure monitoring may be less cumbersome by avoiding the use of roles of ECT paper.
An alternative physiological measure was also explored, to aid reliable estimation of physiological seizure in ECT, as the behavioral seizure (convulsion) may be missed or is attenuated with modification procedures. Cardiovascular response demonstrated success as a potential alternative; sharp drop in the heart rate following the induction of convulsion marked the end of seizure. Some EEG measures in seizure could be extracted and these had value in predicting the efficacy of ECT.
Other issues regarding electroconvulsive therapy
Surveys of ECT practice by Indian psychiatrists indicated that we differ from Western practice as regards the frequency of use of modification, choices of conditions prescribed ECT and the ECT stimulus devices. The attitudes of patients and their relatives to ECT have attracted research. The fact that patients as well as their relatives have a favorable attitude towards ECT may also have allowed more patients to receive and benefit from ECT; and hence, contribute to the bulk of ECT research publications.
Anything left?
The mechanisms of action of ECT have been poorly explored as seen in the published ECT research. Some animal research has appeared pointing to dopamine receptor changes following electroconvulsive shocks (a model of clinical ECT). Among human studies, the publications included comparison of DST results and platelet 5-HT uptake between ECT and imipramine treated patients. Have researchers from India published more on this subject in other indexed journals? This area merits more investigation with the use of modern technology such as magnetic resonance spectroscopy.
NOTE ON THE SEARCH
A search was conducted in all volumes of Indian Journal of Psychiatry from 1959 till 2009. The search was carried out using the following key words: Electroconvulsive therapy, electroconvulsive, ECT, E.C.T. The study has included all studies related to humans, original articles, case series, case reports and excluded animal studies, review articles, editorials and letters that are not data-based, as they are opinions of various authors and not the real clinical data.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Agarwal AK, Winny GC. Role of ECT-Phenothiazine combination in schizophrenia. Indian J Psychiatry. 1985;27:233–6. [PMC free article] [PubMed] [Google Scholar]
- 2.Agarwal AK, Andrade C. Indian psychiatrists’ attitudes towards Electroconvulsive Therapy. Indian J Psychiatry. 1997;39:54–60. [PMC free article] [PubMed] [Google Scholar]
- 3.Andrade C, Gangadhar BN, Subbakrishna DK, Channabasavanna SM, Pradhan N. Clinical prediction of rate of response of endogenous depression to electroconvulsive therapy. Indian J Psychiatry. 1988;30:381–7. [PMC free article] [PubMed] [Google Scholar]
- 4.Andrade C, Gangadhar BN, Vythilingam M, Channabasavanna SM, Pradhan N. Initial response to ECT as a predictor of outcome in endogenous depression. Indian J Psychiatry. 1989;31:293–5. [PMC free article] [PubMed] [Google Scholar]
- 5.Andrade C. Seizure duration and related issues in ECT for endogenous depression. Indian J Psychiatry. 1993;35:43–7. [PMC free article] [PubMed] [Google Scholar]
- 6.Bagadia VN and Shah AV. Comparative study of four techniques of Electro convulsive therapy. Indian J Psychiatry. 1962;4:207–15. [Google Scholar]
- 7.Bagadia VN, Shah LP, Pradhan PV, Doshi J, Abhyankar R. Indian J Psychiatry. 1981;23:324–9. [PMC free article] [PubMed] [Google Scholar]
- 8.Bhaskaran K. A case of circular type of manic depressive psychosis treated with long term electroconvulsive therapy. Indian J Psychiatry. 1963;5:185–8. [Google Scholar]
- 9.Chatterjee SP, Bhaduri AP, Pande RK. Diazepam in modified ECT. Indian J Psychiatry. 1977;19:68–73. [Google Scholar]
- 10.Chavan BS, Kumar S, Arun P, Bala C, Singh T. ECT: Knowledge and attitude among patients and their relatives. Indian J Psychiatry. 2006;48:34–8. doi: 10.4103/0019-5545.31616. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Chopra VK, Sinha VK. ECT in mentally retarded subjects with psychiatric illness. Indian J Psychiatry. 2002;44:57–64. [PMC free article] [PubMed] [Google Scholar]
- 12.Chopra VK, Sinha VK, Das S. Normal pressure hydrocephalus presenting as psychotic depression: Moderately successful treatment with a course of ECT and pharmacotherapy: A case report. Indian J Psychiatry. 2002;44:71–5. [PMC free article] [PubMed] [Google Scholar]
- 13.Dalal PK, Lal N, Trivedi JK, Seth PK, Agarwal AK, Khalid A. ECT and platelet 5-HT uptake in major depression. Indian J Psychiatry. 1997;39:272–7. [PMC free article] [PubMed] [Google Scholar]
- 14.Dalal PK, Lal N, Trivedi JK, Seth PK, Agarwal AK and Khalid A. Active platelet 5-HT uptake in major depression. Indian J Psychiatry. 1998;40:60–6. [PMC free article] [PubMed] [Google Scholar]
- 15.Deshmukh DK, Sethna KJ, Nagesh RP, Haridas RM, Patankar SV. A comparative study to evaluate the efficacy of spaced V/s daily electroconvulsive therapy in schizophrenia. Indian J Psychiatry. 1980;22:366–7. [PMC free article] [PubMed] [Google Scholar]
- 16.Dutt ND, Mahapatra PK, Gangadhar BN, Sadasivan PK, Janakiramaiah N, Subbakrishna DK, et al. EEG-Delta band spectral power: Differences between unilateral and bilateral ECT seizures. Indian J Psychiatry. 1997;39:61–3. [PMC free article] [PubMed] [Google Scholar]
- 17.Gada MT. Prolonged apnoea with succinyl choline during electroconvulsive therapy. Indian J Psychiatry. 1985;27:335–6. [PMC free article] [PubMed] [Google Scholar]
- 18.Gangadhar BN, Choudhary RJ, Channabasavanna SM. ECT and drug induced Parkinsonism. Indian J Psychiatry. 1983;25:212–3. [PMC free article] [PubMed] [Google Scholar]
- 19.Gangadhar BN, Jyoti Rao KM, Sujatha BL, Janakiramaiah N, Subbakrishna DK. ECT induced EEG seizure: Validity of duration estimation by last spike. Indian J Psychiatry. 1993;35:175–6. [PMC free article] [PubMed] [Google Scholar]
- 20.Gangadhar BN, Candade VS, Laxmana G, Janakiramaiah N, Mahapatra PK. Computers in ECT and paperless EEG measuring. Indian J Psychiatry. 1995;37:98. [PMC free article] [PubMed] [Google Scholar]
- 21.Gill NS, Girish K, Gangadhar BN. Ictal RPP-A supplement to cuff method in detecting ECT induced cerebral seizure. Indian J Psychiatry. 2002;44:29–33. [PMC free article] [PubMed] [Google Scholar]
- 22.Girish K, Prasad KMR, Gangadhar BN, Janakiramaiah N, Subbakrishna DK. Clinical predictors of seizure threshold in bilateral ECT. Indian J Psychiatry. 1998;40:327–30. [PMC free article] [PubMed] [Google Scholar]
- 23.Girish K, Jayakumar PN, Murali N, Gangadhar BN, Janakiramaiah N, Subbakrishna DK. ECT and T2 relaxometry: A static water proton magnetic resonance imaging study. Indian J Psychiatry. 2001;43:22–4. [PMC free article] [PubMed] [Google Scholar]
- 24.Girish K, Gangadhar BN, Janakiramaiah Merits of EEG monitoring during ECT: A prospective study on 485 patients. Indian J Psychiatry. 2002;44:24–8. [PMC free article] [PubMed] [Google Scholar]
- 25.Girish K, Gill NS. Electroconvulsive therapy in lorazepam non-responsive catatonia. Indian J Psychiatry. 2003;45:21–5. [PMC free article] [PubMed] [Google Scholar]
- 26.Girish K, Jayakumar PN, Janakiramaiah N, Gangadhar BN. MRI - T2 relaxometry of brain regions and cognitive dysfunction following electroconvulsive therapy. Indian J Psychiatry. 2007;49:195–9. doi: 10.4103/0019-5545.37321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Girish K. A survey on falling trends in ECT in a mental health trust in UK: Future implications. Indian J Psychiatry. 2007;49:32. [Google Scholar]
- 28.Goswami U, Kumar U, Singh B. Efficacy of electroconvulsive therapy in treatment resistant schizophrenia: A double blind study. Indian J Psychiatry. 2003;45:26–9. [PMC free article] [PubMed] [Google Scholar]
- 29.Gupta UK, Mahendru RK, Mehta RK, Sonkar P. A comparative study of etomidate and thiopentone in modified ECT. Indian J Psychiatry. 1986;28:151–4. [PMC free article] [PubMed] [Google Scholar]
- 30.Gupta N, Avasthi A, Kulhara P. Response to first ECT in depression: A predictor of outcome. Indian J Psychiatry. 1998;40:322–6. [PMC free article] [PubMed] [Google Scholar]
- 31.Gupta N, Avasthi A, Kulhara P. Clinical variables as predictors of response to electroconvulsive therapy in endogenous depression. Indian J Psychiatry. 2000;42:60–5. [PMC free article] [PubMed] [Google Scholar]
- 32.Jain G, Kumar V, Chakrabarti S, Grover S. Use of electroconvulsive treatment in elderly: A clinical audit. Indian J Psychiatry. 2007;49:31. [Google Scholar]
- 33.Jain RK, Goyal SP, Jain VK, Mehrotra MP, Wahal PK, Prakash V. ECG changes following electroconvulsive therapy. Indian J Psychiatry. 1976;18:260–5. [Google Scholar]
- 34.Jana D, Banerjee G. Bilateral frontal lobe CT Scan abnormality following ECT in an adolescent. Indian J Psychiatry. 1992;34:392–4. [PMC free article] [PubMed] [Google Scholar]
- 35.Janakiramaiah N, Subbakrishna DK. ECT-Chlorpromazine combination compared with chlorpromazine only in schizophrenia. Indian J Psychiatry. 1981;23:230–3. [PMC free article] [PubMed] [Google Scholar]
- 36.Janakiramaiah N, Jyoti Rao KM, Praveen J, Sujatha L, Gangadhar BN, Subbakrishna DK. Seizure duration over ECT sessions: Influence of spacing ECTs. Indian J Psychiatry. 1992;34:124–7. [PMC free article] [PubMed] [Google Scholar]
- 37.Jayaprakash MS, Gangadhar BN, Janakiramaiah N, Subbakrishna DK. Limitations of motor seizure monitoring in ECT. Indian J Psychiatry. 1998;40:55–9. [PMC free article] [PubMed] [Google Scholar]
- 38.Kulkarni MR, Mulay VP. Value of propanidid in electroconvulsive therapy (comparison with thiopentone) Indian J Psychiatry. 1980;22:371–4. [PMC free article] [PubMed] [Google Scholar]
- 39.Kumar S, Jain M, Mohanty S. Effects of ECT in enhancing quality of life in mania. Indian J Psychiatry. 2007;49:35. [Google Scholar]
- 40.Kurian S, Tharyan P, Jacob KS. Combination of ECT and clozapine in drug-resistant schizophrenia. Indian J Psychiatry. 2005;47:245. doi: 10.4103/0019-5545.43067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Mahendru RK, Gupta UK, Mehta RK, Sonkar P. A comparative study of althesin and thiopentone in modified ECT. Indian J Psychiatry. 1989;31:338–40. [PMC free article] [PubMed] [Google Scholar]
- 42.Murali N, Sarvanan ES, Santosh MG, Gangadhar BN, Janakiramaiah N, Rao UM, et al. Cardiovascular response to ECT is unaffected by extent of motor seizure modification. Indian J Psychiatry. 1999;41:236–41. [PMC free article] [PubMed] [Google Scholar]
- 43.Murthy HN. Effects of electroconvulsive treatment on memory and intelligence in schizophrenics. Indian J Psychiatry. 1966;8:138–42. [Google Scholar]
- 44.Pandey RS, Sharma P. ECT induced catatonia: A case report. Indian J Psychiatry. 1988;30:105–7. [PMC free article] [PubMed] [Google Scholar]
- 45.Selvan PC, Mayur PM, Gangadhar BN, Janakiramaiah N, Subbakrishna DK, Murali N. Comparison of therapeutic efficacy of ECT and Imipramine: A randomized controlled trial. Indian J Psychiatry. 1999;41:228–35. [PMC free article] [PubMed] [Google Scholar]
- 46.Phutane VH, Thirthalli J, Harish T, Gangadhar BN. Why do psychiatrists prescribe ECT to schizophrenia? Indian J Psychiatry. 2007;49:33. doi: 10.4103/0019-5545.82544. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Ray SD, Kapur RL. Significance of some prognostic indices of schizophrenics treated with ECT and chlorpromazine. Indian J Psychiatry. 1963;5:190–5. [Google Scholar]
- 48.ECT and Clozapine combination producing delirium: A case report. Indian J Psychiatry. 2003;45:193. [PMC free article] [PubMed] [Google Scholar]
- 49.Shah AV, Bagadia VN. Analysis of 5021 electroconvulsive therapies. Indian J Psychiatry. 1961;4:129–38. [Google Scholar]
- 50.Shah VD, Mansur AM, Hakim IR, Mehd US, Mehta SH, Damany SJ. Cardiovascular and electrocardiographic changes after electroconvulsive therapy (ECT)-A series of 50 cases. Indian J Psychiatry. 1977;19:51–3. [Google Scholar]
- 51.Shukla GD, Sharma VC. Evaluation of thiopentone, diazepam and propanidid in modified ECT. Indian J Psychiatry. 1979;21:60–3. [Google Scholar]
- 52.Shukla GD, Sharma UC, Mehrotra AN. Intraocular pressure changes following modified ECT. Indian J Psychiatry. 1980;22:274–6. [PMC free article] [PubMed] [Google Scholar]
- 53.Shukla GD, Mishra DN. Death following ECT-A case report. Indian J Psychiatry. 1985;27:95–7. [PMC free article] [PubMed] [Google Scholar]
- 54.Sivaprakash B, Chandrasekaran R, Sahai A. Predictors of response to electroconvulsive therapy in major depression. Indian J Psychiatry. 2000;42:148–55. [PMC free article] [PubMed] [Google Scholar]
- 55.Srinivasan TN, Suresh TR, Jayaram V. Issues in the use of maintenance electroconvulsive therapy. Indian J Psychiatry. 1995;37:139–42. [PMC free article] [PubMed] [Google Scholar]
- 56.Thakur A, Dutta S, Jagadheesan K, Sinha VK. Electroconvulsive therapy in pre-pubertal catatonia: A case study. Indian J Psychiatry. 2001;43:354–6. [PMC free article] [PubMed] [Google Scholar]
- 57.Tharyan P, Saju PJ, Datta S, John JK, Kuruvilla K. Physical morbidity with unmodified ECT-A decade of experience. Indian J Psychiatry. 1993;35:211–4. [PMC free article] [PubMed] [Google Scholar]
- 58.Thirthalli J, Gangadhar BN, Janakiramaiah N, Girish K, Ramakrishnan AG. Post-seizure EEG fractal dimension and spectral power predict antidepressant response to unilateral ECT. Indian J Psychiatry. 2003;45:16–20. [PMC free article] [PubMed] [Google Scholar]
- 59.Thomas N, Suresh TR, Srinivasan TN. Electroconvulsive therapy in catatonia associated with pneumothorax. Indian J Psychiatry. 1994;36:91–2. [PMC free article] [PubMed] [Google Scholar]
- 60.Trivedi JK, Singh RP, Lal N, Viswanathan PN, Kumar S. Effect of imipramine and ECT on platelet MAO activity in depressives. Indian J Psychiatry. 1989;31:139–43. [PMC free article] [PubMed] [Google Scholar]
- 61.Varma SL, Lal N, Trivedi JK, Anand M. Dexamethasone suppression test in depressives treated with ECT. Indian J Psychiatry. 1987;29:353–7. [PMC free article] [PubMed] [Google Scholar]
- 62.Varma SL, Trivedi JK, Anand M, Gulam R, Lal N. Post dexamethasone plasma cortisol levels in depressives treated with imipramine and electroconvulsive therapy. Indian J Psychiatry. 1989;31:78–82. [PMC free article] [PubMed] [Google Scholar]