

Abstract
Vasitis or inflammation of the vas deferens is a rarely described condition categorized by Chan & Schlegel1 as either generally asymptomatic vasitis nodosa or the acutely painful infectious vasitis. Clinically, infectious vasitis presents with nonspecific symptoms of localized pain and swelling that can be confused with other, more common conditions such as epididymitis, orchitis, testicular torsion, and inguinal hernia. Ultrasound with duplex Doppler scanning can be used to exclude epididymitis, orchitis, and testicular torsion. On the other hand, while inguinal hernia is difficult to differentiate from vasitis using ultrasound, computed tomography (CT) is diagnostic. We describe 2 cases of vasitis with clinical and ultrasound findings that initially were interpreted as inguinal hernias. In both patients, CT was diagnostic for vasitis showing an edematous spermatic cord and no hernia. Urine cultures in both patients were negative, but the symptoms resolved with antibiotic treatment.
Introduction
Vasitis is rarely reported as an isolated condition. The more commonly described inflammation of the vas deferens, vasitis nodosa, is a benign condition that has been well-characterized (both macroscopically and microscopically) and is usually associated with a history of vasectomy. Clinically, patients present with a nodular mass in the vas deferens and are often asymptomatic and require no specific treatment.1 If necessary, a biopsy will establish the diagnosis.
Infectious vasitis, while rarely reported in the literature, is thought to be caused by common urinary tract pathogens. Patients present with pain and swelling in the groin and are usually thought to have epididymitis, orchitis, testicular torsion or inguinal hernia. In the few cases of infectious vasitis described, imaging was not used and the patients were treated surgically for suspected inguinal hernias with eventual cord excision and/or drainage when no hernia was found.2–5 The 2 cases presented in this report were differentiated using computed tomography (CT) and were treated non-invasively using antibiotics.
Case 1
A 40-year-old male presented to the emergency room with a 36-hour history of pain in the left groin extending down to the upper scrotum exacerbated with movement and coughing. The patient did not have fever, chills or urinary symptoms. There was no previous history of sexually transmitted infections, but the patient was recently divorced and was sexually active. There was no history of heavy lifting, but he had a long-standing complaint of left lower quadrant pain for which he had been given no specific diagnosis other than irritable bowel. On exam, the left groin was tender and swollen, but both testicles felt normal. Laboratory results were normal except for a slightly elevated white blood count (8.72 neutrophils) and a few cells in the urine (5–10 WBC, 10–40 RBC) but with normal urine cultures.
Ultrasound examination revealed normal and symmetrical testicular and epididymal size and blood flow, excluding orchitis, epididymitis and testicular torsion. An abnormal mass in the left inguinal canal was interpreted as a possible incarcerated inguinal hernia.
The patient was referred to general surgery for a hernia repair and a CT scan was ordered to assess the extent of the possible incarcerated hernia. The CT scan was negative for an inguinal hernia and instead revealed an inflamed spermatic cord consistent with vasitis. The patient was referred back to urology, given antibiotics, and the condition resolved.
Case 2
A 32-year-old male presented to the emergency room with a 12-hour history of pain in the right groin radiating to the upper scrotum. The pain was reportedly similar to that felt prior to the repair of a left inguinal hernia a few years earlier. There were no urinary symptoms, but the patient had a remote history of chlamydia, was sexually active and had a slight fever (38.2°C). On exam, he had tenderness and swelling in the right groin. Laboratory tests were negative with no cells in the urine; urine cultures for chlamydia and gonorrhea were negative.
Ultrasound examination revealed normal and symmetrical testicular and epididymal size and blood flow not consistent with orchitis, epididymitis or testicular torsion. An abnormal mass in the right inguinal canal was interpreted as a possible incarcerated inguinal hernia and a CT was suggested for further evaluation.
The CT scan was negative for inguinal hernia and instead revealed a thickened, edematous spermatic cord consistent with vasitis. The patient was referred to urology and given antibiotics once again with eventual resolution of symptoms.
Discussion
We are only aware of 4 cases of infectious vasitis described in English language medical journals since 1933 and none in the past 20 years when modern medical imaging has been readily available.2–5 Epididymitis, orchitis, testicular torsion and inguinal hernia are the most likely causes of groin pain and inflammation in males and it is not surprising that all previous reported cases of infectious vasitis underwent surgical intervention. An article with more of an imaging focus on this topic has been published.6
Epididymitis is the most common cause of intrascrotal inflammation and can occur with or without associated orchitis. Ultrasound of the area showing differential blood flow can confirm if the condition is isolated epididymitis or complicated with associated orchitis. These 2 conditions most frequently affect males between the ages of 18 and 35 years, and can occur with or without infection. Bacterial infection with Chlamydia or gonorrhea is the most likely causative agent and treatment usually consists of antibiotics.7
Testicular torsion, while possible at any age, most commonly occurs in males aged 12 to 18 years. The condition presents as acute onset of pain and the affected testicle may be elevated and oriented transversely. The cremasteric reflex is usually abnormal in cases of testicular torsion, and ultrasound will reveal decreased blood flow to the affected testicle.8
About 30% of men will experience an inguinal hernia in their lifetime, making inguinal hernia repair one of the most common surgical procedures. Hernias present as masses in the groin, and can become painful when incarcerated or trapped.9 The clinical and ultrasound findings of incarcerated inguinal hernias and vasitis can be very difficult to distinguish: both present clinically with groin masses and pain. In addition, on ultrasound, both conditions appear as masses in the area of the spermatic cord with normal testicular and epididymal size and blood flow. In the cases presented in this report, CT was used to differentiate between incarcerated inguinal hernia and vasitis.
Conclusion
While the clinical and ultrasound features of vasitis and inguinal hernia are similar, computed tomography can readily distinguish between the 2 avoiding unnecessary surgeries.
Fig. 1.

Axial computed tomography image showing thickened left spermatic cord with surrounding edema as compared to the normal right spermatic cord.
Fig. 2.

Sagittal computed tomography image showing inflamed left spermatic cord and no hernia.
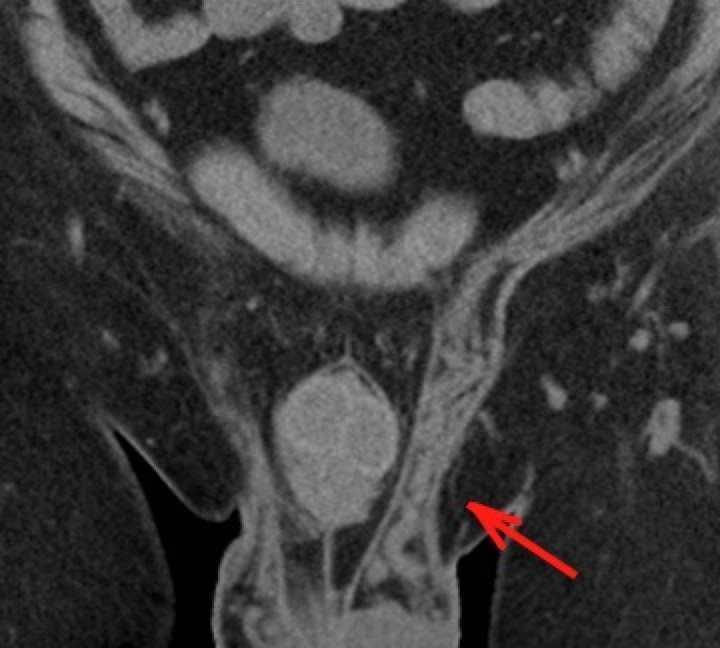
Fig. 3.

Coronal computed tomography image showing abnormal left spermatic cord with edema effacing the normal fat in the cord.
Fig. 4.
Coronal computed tomography image showing normal fat within the left spermatic cord after treatment.
Fig. 5.

Axial computed tomography image showing inflamed right spermatic cord compared with normal cord on left with preserved fat planes.
Fig. 6.

Sagittal computed tomography image showing inflamed right spermatic cord and no hernia.
Footnotes
Competing interests: None declared.
This paper has been peer-reviewed.
References
- 1.Chan PTK, Schlegel PN. Inflammatory conditions of the male excurrent ductal system. Part I and II. J Androl. 2002;23:453–69. [PubMed] [Google Scholar]
- 2.Bissada NK, Redman JF, Finkbeiner AE. Unusual inguinal mass secondary to vasitis. Urology. 1976;8:488–9. doi: 10.1016/0090-4295(76)90284-3. [DOI] [PubMed] [Google Scholar]
- 3.Maitra AK. Odd inguinal swelling. Lancet. 1970;1:45. doi: 10.1016/s0140-6736(70)90566-0. [DOI] [PubMed] [Google Scholar]
- 4.Ryan SP, Harte PJ. Suppurative inflammation of vas deferens: an unusual groin mass. Urology. 1988;31:245–6. doi: 10.1016/0090-4295(88)90151-3. [DOI] [PubMed] [Google Scholar]
- 5.Wolbarst AL. Vas deferens, generally unrecognized clinical entity in urogenital disease. J Urol. 1933;29:405. [Google Scholar]
- 6.Eddy K, Connell D, Goodacre B, et al. Imaging findings prevent unnecessary surgery in vasitis: an under-reported condition mimicking inguinal hernia. Clin Radiol. 2011;66:475–7. doi: 10.1016/j.crad.2010.12.006. [DOI] [PubMed] [Google Scholar]
- 7.Trojian TH, Lishnak TS, Heiman D. Epididymitis and orchitis: an overview. Am Fam Physician. 2009;79:583–7. [PubMed] [Google Scholar]
- 8.Edelsberg JS, Surh YS. The acute scrotum. Emerg Med Clin North Am. 1988;6:521–46. [PubMed] [Google Scholar]
- 9.Jenkins JT, O’Dwyer PJ. Inguinal hernias. BMJ. 2008;336:269–72. doi: 10.1136/bmj.39450.428275.AD. [DOI] [PMC free article] [PubMed] [Google Scholar]