

Abstract
Objectives
To compare whether four methods to measure or estimate height among wheelchair users result in significantly different estimates and to determine which method is most accurate.
Design
Height data were obtained for 141 wheelchair users. Height estimates included asking for self-report and measuring recumbent length, knee height, and armspan. All analyses were conducted separately for men and women. A two-group confirmatory factor analysis assessed which measure provided the best estimate of height in this population. It also tested the measurement invariance of the four height estimates between men and women and whether there were significant differences across these estimates within each sex.
Results
CFA findings indicated that the four measures yielded significantly different height estimates and BMI values for both men and women. For both sexes, armspan resulted in the longest estimate and measured recumbent length the shortest, with the reverse pattern for BMI values. The common variance estimates were outstanding for recumbent length (92%) and knee height (>83%) and very good for self-report (>75%), while the common variance for armspan was poor (<42%).
Conclusions
The measurement method used to estimate height yields significantly different values for both height and BMI among wheelchair users who cannot stand to be measured using a stadiometer. Recumbent length yields the most accurate height estimate for wheelchair users. However, when logistical and practical considerations pose difficulties for obtaining this measure, height estimates based on knee height and self-report may provide reasonable alternatives.
Keywords: Body Height, Measures, Wheelchairs
Obtaining an accurate height estimate is important for calculating body mass index [BMI], 1-3 pulmonary function, 4 determining body surface area for drug dosages and renal clearances, and other patient care issues.1 However, measuring height can be difficult for individuals who cannot stand,2,5 or who have various physical anomalies such as spasticity, 6 contractures, fractures, amputations, scoliosis, paralysis,1 or osteoporosis.7 Unfortunately, there is no criterion standard to measure or estimate height for those who cannot stand to be measured with a stadiometer. Lack of a standardized approach for those who cannot stand limits data availability and quality for this population. For example, without guidelines recommending how to measure height for those unable to stand, the federal initiative designed to assess the health and nutritional status of Americans, the National Health and Nutrition Examination Survey (NHANES), has forgone collecting height data for those unable to stand unassisted. Therefore, NHANES data which are used to calculate BMI and track obesity prevalence are not available for those with mobility impairments that affect walking or standing.
Individuals with serious mobility impairment that precludes standing are not the only group for whom standing height measures are difficult to obtain. Standing height is also difficult to obtain among older adults with kyphosis and hospitalized, bedridden patients. Investigators have assessed the validity of armspan,8-10 demi-span,11 half-armspan, and knee height12,13 among others for use as potential height estimates for use in these groups in lieu of standing height.
Several published studies have explored alternate methods for measuring or estimating stature among this population.14,15 Using a similar approach to the one created to predict stature among older adults, Chumlea et al.15 used knee height to predict stature among children and adults with mobility impairments based on data from the National Health and Nutrition Examination Survey (NHES, 1960-1970). Although these equations derive from non-impaired populations, the authors suggest the estimates can be applied to a mobility impaired sample.
More recently, Canda14 explored which of several estimation equations best predicted stature for mobility impaired individuals, but also collected data from a non-impaired sample. Estimation equations were derived from eight anthropometric indices: sitting height, armspan, upper arm length, forearm length, hand length, thigh length, lower leg length, and foot length. The authors report that the equations that include sitting height and upper and lower extremities yielded the highest correlations with the lowest errors, although the specific measures included in equations differed by sex. Thus, the authors suggest obtaining multiple measures for use in an equation to derive the best height estimate.
Garshick et al.4 examined the accuracy of self-report and whether upper extremity measures predicted stature in those with spinal cord injury (SCI) compared to recumbent length. Although upper extremity measures significantly predicted measured body length, self-reported height accounted for greater variance in measured length than any upper extremity measures, including armspan. Nevertheless, men with SCI overestimated their height by an average of 2.3 cm ± 3.45 cm. Finally, results from several studies support measuring upper arm length or knee height as alternate approaches for estimating height among children and adults with cerebral palsy.6,16,17
Despite the array of available height measurement and estimation methods, there is a need to investigate which of several approaches is most accurate for determining height among those who cannot stand. Therefore, the purpose of this study was to determine 1) if various methods for measuring height yield significantly different height estimates among wheelchair users with diverse impairments and 2) which method yields the most accurate height estimate for this population. Height assessment methods examined included (a) self-report; (b) recumbent length, (c) armspan length and (d) estimate from knee height using a formula developed for individuals with mobility impairment.15
METHODS
Recruitment
Height data were collected as part of an ongoing randomized-controlled trial that investigates the effectiveness of an intervention promoting physical activity adoption and maintenance among wheelchair users (NIH grant #R01 HD48628). Recruitment methods encompassed numerous activities including disseminating posters and brochures to healthcare providers and facilities and advertising in multiple outlets.18 Interested individuals called the office to undergo a telephone screening to determine their eligibility. Three-hundred and fifty-five individuals were screened, 172 of whom were eligible, although 38 declined to participate. Baseline data were collected on 143 individuals, while data from two double amputees were excluded, leaving a sample size of 141. Thus, the sample is based on 141 eligible individuals who underwent baseline testing. The human subjects committee of the sponsoring institution approved the study (HSC #10053), and all participants signed a consent form.
Participants
Participants had to meet the following eligibility requirements:
experience a mobility impairment for ≥ six months that necessitates wheelchair use for mobility outside of the home;
be between the ages of 18 – 65;
not be currently physically active;
receive physician consent to exercise;
Exclusion criteria included the following:
body mass index of 50 or higher;
medical conditions such as chronic obstructive pulmonary disease, liver or kidney disease, or cardiac problems that their physician identifies as being contraindicated for participating in unsupervised exercise;
presence of significant cognitive impairment that precludes ability to self-direct daily activities;
pregnant, or planning to become pregnant; and
two missing lower limbs.
Data Collection
Weight and height data were collected during participants’ baseline visit to the exercise lab of the General Clinical Research Center of the University of Kansas Medical Center between 2006 and 2009. Weight was measured using a wheelchair access scale (Seca # 664) in three steps: weighing participants in their wheelchair, weighing their chair alone, and subtracting the wheelchair weight from the combined weight. Height assessment included obtaining participants’ self-reported height and obtaining measurements using three different methods, described below. All measures were performed twice, with a third taken if the first two were discrepant by more than one quarter inch (for armspan and recumbent length) or 0.4 centimeter for knee height. For each measure, an average of the estimates was calculated. To assure the independent measures, the anthropometer was removed and the device reset before repeating the procedure. A single tester conducted all height measures.
Armspan and recumbent lengths were measured with a custom-made anthropometer devised for this study using two adjustable A squares (U.S. Patent # 4,525,933), four wooden blocks, and two metal plates. Wooden blocks secured the two 48-inch rulers with screws, permitting the ruler to slide open for measuring lengths between 48 and 85 inches, with a metal plate affixed to the inside edge at each end. The following paragraphs describe the methods for measuring recumbent and armspan lengths with this anthropometer.
Armspan
Participants remained in their wheelchairs and were asked to abduct their shoulders to 90 degrees while fully extending elbows, wrists, and fingers. With a tester on either side of the participant, the ruler was aligned with their shoulders and slid apart to the tips of the longest fingers. Staff assisted participants to steady their arms during each measurement reading.
Recumbent Length
This measure required participants’ lie in supine on a raised mat table. With the participant’s head in the Frankfort plane, staff placed one metal plate against the top of the participant’s head and the ruler along the right side of the participant’s body. With the right leg aligned with their hip, the other end of the ruler was placed on the distal end of the calcaneous of their right foot. If the participant had spasticity, contractures, or could not lie flat or dorsiflex the ankle to 90 degrees, staff manually assisted in extending the leg as far as possible or dorsiflexing the ankle. Height was recorded to the nearest 1/16 of an inch.
Knee Height
A knee height caliper (The Shorr Knee-Height Caliper, Weigh and Measure, LLC [formerly Shorr Productions], Olney, Maryland) was used for this measure. While on the mat table, participants were instructed to sit upright and hang their legs off the table edge. Using a goniometer, the participant’s right knee was held at a 90 degree angle with the caliper’s fixed blade at the distal end of the calcaneus and the sliding blade on the anterior side of the distal condyles of the femur so the caliper shaft would align with the tibia. Measurement was determined to the nearest 0.1 cm. The knee height value was applied to a formula developed for mobility- impaired individuals 15 to estimate their height. The formula varies based on sex, race, and age. Formulas can be found in the original paper.
Data Analysis
Data were analyzed in SPSS version 1719 and SAS version 9.2.20 Prior to conducting all analyses, we imputed the few data points that were missing (3.9%). Assuming a combination of MCAR and MAR, which is a very reasonable assumption for these data, we imputed the missing values using the iterative Bayesian MCMC algorithm in SAS PROC MI (www.SASinstitue.com) with the maximum likelihood EM algorithm used as the prior estimates for the MCMC algorithm.21 Due to sex differences in height, we conducted separate analyses for men and women and examined whether there were significant differences between sexes on relevant demographic variables. Basic descriptive analyses were conducted for demographic data and we conducted t-tests for continuous variables (age, age of disability onset, and time with disability) and chi-square tests for categorical variables (race, education level, employment status, and impairment etiology) to examine whether there were significant differences between sexes. The three height estimates measured in inches (self-reported height, recumbent length, and armspan) were converted to centimeters to assure height estimates were on the same metric.
To examine the relationships among the four measures of height and to determine which measure provides the best estimate of a person’s height in this population, we conducted a 2-group (men, n = 70, vs. women, n = 71) confirmatory factor analysis (CFA; see Brown 22) of the four height measures. With this analysis, the reference standard for height becomes the common factor defined by the shared variance among the four indicators of height (see Figure 1). We view this reference standard as the best possible standard given that there is not an objective criterion standard for this population to which one can compare. To assist in determining which indicators are more accurate in estimating height we used the non-arbitrary effects-coded method of scale setting.23 This method of scale setting constrains the loadings to average 1.0 instead of arbitrarily assigning one of the indicators to be 1.0. The result is a set of loadings that vary around 1.0. Loadings that are higher than others are stronger loadings, contributing more variance to the definition of the construct than do loadings that are lower. Using the effects-coded method to scale the construct mean is similarly constrained, but the intercepts of the indicators are constrained to average 0. The result is an estimate of the latent mean that is equal to the average estimated height across the four methods but weighted by the strength of the loading.
FIGURE 1.
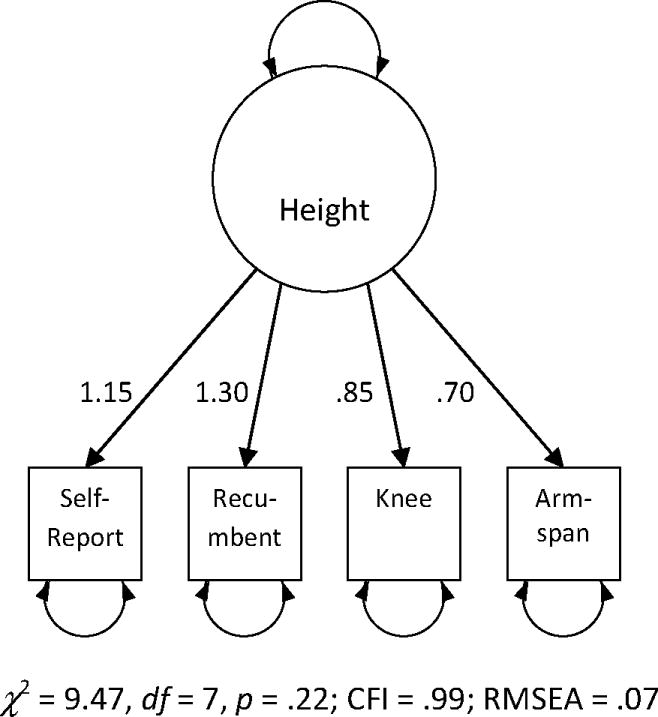
CFA model of weak invariance. CFA indicates confirmatory factor analysis; CFI, comparative fit index, RMSEA, root mean square error of approximation.
We conducted likelihood ratio (LR) tests of exact fit, which is commonly referred to as chi-square test of model fit, to evaluate measurement invariance of the four height measures between sexes. Based on the invariance testing results, we pairwise compared the CFA model-implied means of the four measures using LR tests with Bonferroni adjustment.
RESULTS
Table 1 presents participant demographics. The sample included almost equal men (49.6%) and women (50.4%) with no significant differences between the sexes in terms of their average age, age of disability onset, or time with disability. Men’s and women’s average age was about 44 with a range of 18 to 65 years and they lived an average of 22 years with their mobility impairment. Among both men and women SCI is the primary cause of mobility impairment, and spina bifida (SB) and cerebral palsy (CP) are the second most common causes of impaired mobility. However, significantly more men experienced SCI than women, χ2 (1, n=141) = 10.79, p < .01. Although all participants used a wheelchair for mobility, some (37.6%) could walk.
Table 1.
Participant Demographics
| Demographic variable | Men (n=70) % (n) / M (SD) | Women (n=71) % (n) / M (SD) | χ2 / t | p |
|---|---|---|---|---|
| Age | 44.61 (11.77) | 44.18 (13.42) | .20 | .84 |
| Age of disability onset | 23.28 (16.30) | 21.99 (19.63) | .42 | .67 |
| Time w/ disability | 21.88 (15.56) | 21.97 (16.25) | -.03 | .97 |
| Disability since birth | 18.6 (13) | 28.2 (20) | 1.82 | .18 |
| Disability onset before 18 years old | 35.7 (25) | 45.1 (32) | 1.28 | .26 |
| Race/Ethnicity | .02a | 1.00 | ||
| Hispanic | 2.9 (2) | 4.2 (3) | ||
| White | 78.6 (55) | 78.9 (56) | ||
| Black | 15.7 (11) | 14.1 (10) | ||
| Other | 2.9 (2) | 2.8 (2) | ||
| Primary impairment | 14.90 | < .01 | ||
| Spinal Cord Injury | 61.4 (43) | 33.8 (24) | ||
| Spina Bifida/Cerebral Palsy | 12.9 (9) | 25.4 (18) | ||
| Multiple Sclerosis | 5.7 (4) | 12.7 (9) | ||
| Amputation | 5.7 (4) | 1.4 (1) | ||
| Other | 14.3 (10) | 26.8 (19) | ||
| Education | .03a | .54 | ||
| ≥High School | 18.6 (13) | 21.1 (15) | ||
| Some college/Bachelor’s degree | 41.4 (29) | 50.7 (36) | ||
| Some graduate school/Grad. degree | 27.1 (19) | 19.7 (14) | ||
| Other | 5.7 (4) | 2.8 (2) | ||
| Employment | ||||
| Employed (full/part) | 35.7 (25) | 31 (22) | .79 | .67 |
| Unemployed | 34.3 (24) | 42.3 (30) | ||
| Other (Retried, Student, Homemaker) | 21.4 (15) | 21.1 (15) |
Fisher’s exact probability
Table 2 (men) and Table 3 (women) provide the sufficient statistics (correlations, means, and standard deviations) among the four measures evaluated in the CFA model. A casual inspection of the correlations shows that armspan correlates much less with the other three, suggesting that armspan is a less reliable indicator of body height.
Table 2.
Sufficient Statistics among Height Measures (in centimeters) for Men
| Variable | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| 1. Self-reported height | 1.00 | |||
| 2. Recumbent length | .87** | 1.00 | ||
| 3. Knee height | .83** | .89** | 1.00 | |
| 4. Armspan length | .58** | .56** | .62** | 1.00 |
| M | 177.20 | 173.48 | 175.12 | 180.79 |
| SD | 10.92 | 11.78 | 8.29 | 9.24 |
p < .05,
p < .01
Table 3.
Sufficient Statistics among Height Measures (in centimeters) for Women
| Variable | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| 1. Self-reported height | 1.00 | |||
| 2. Recumbent length | .84** | 1.00 | ||
| 3. Knee height | .77** | .87** | 1.00 | |
| 4. Armspan length | .61** | .59** | .61** | 1.00 |
| M | 160.59 | 158.28 | 161.25 | 163.94 |
| SD | 11.45 | 11.52 | 7.64 | 9.79 |
p < .05,
p < .0
Table 4 presents the fit information for the CFA model testing for measurement invariance across men and women. This table shows that weak invariance was tenable indicating that the strength of the relations among the four indicators of height is statistically the same for men and women. The equality constraints on the loadings also improved model fit so that the weak invariance model provided acceptable comparative fit index (CFI) and root mean square error of approximation (RMSEA) values. Figure 1 shows the loadings, which are also known as validity coefficients, that were estimated for this sample. The recumbent measure had the highest loading on the common factor with greater than 90% explained variance for both men and women, indicating that it is more centrally related to the common factor than the other three measures. Knee height had greater than 80% variance accounted for by the common factor for both sexes. Armspan had the lowest loading, indicating that it is not a very valid measure of height relative to the other three measures of height. The variance explained in armspan was only about 40% for both men and women (see Table 5).
Table 4.
Fit information for Test of Invariance across Men vs. Women
| Model | χ2 | df | p | Δχ2 | Δdf | p | CFI | RMSEA |
|---|---|---|---|---|---|---|---|---|
| Configural invariance | 7.82 | 4 | .09 | -- | .99 | .12 | ||
| Weak invariance | 9.47 | 7 | .22 | 1.64 | 3 | .65 | 1.00 | .07 |
| Strong invariance | 45.05 | 10 | < .01 | 35.59 | 3 | < .01 | .93 | .22 |
Table 5.
Height and BMI Estimates from the CFA Model
| Self-reported height | Recumbent length | Knee height | Armspan length | |
|---|---|---|---|---|
| Variance explained by height common factor | ||||
| Men | .83 | .92 | .85 | .42 |
| Women | .75 | .92 | .83 | .38 |
| Mean height | ||||
| Men | 177.133*,24** | 173.4114** | 175.1414** | 180.73123** |
| Women | 160.5224* | 158.221*34** | 161.274*2** | 163.8913*2** |
| Mean height difference between men vs. women | 16.62 | 15.20 | 13.87 | 16.85 |
| Mean BMI | ||||
| Men | 29.7524** | 30.983*14** | 30.182*4** | 28.44123*** |
| Women | 31.204* | 31.8834** | 30.602** | 29.9312** |
Self-reported height,
recumbent length,
knee height estimate,
armspan length
Adjusted p < .05,
Adjusted p < .01
Table 4 also shows that strong measurement invariance was not tenable. A post-hoc investigation of the constraints on the intercepts indicated that the four height measures yielded significant differences (see Table 5). For men, armspan length was significantly greater than all other height measures. Recumbent length was significantly less than the self-reported height, and it was less than the knee height but not significantly so. Self-reported height was significantly greater than the knee height. For women, armspan length was significantly greater than all other height estimates and measured recumbent length was significantly less than all other measurement methods (self-reported and knee height and armspan). Notably, the stature estimate using knee height applying the formula for mobility impaired adults fell between the men’s self-reported height and recumbent length. While for women this stature estimate yielded a larger estimate than for both self-reported and recumbent length.
Table 5 also presents the CFA model-implied BMI means. The pattern follows findings for the height values, with measures that yielded the greater height estimates resulting in the lower BMI values or vice versa. Thus, armspan length yielded a significantly lower BMI value than all other height estimates for men and two other estimates for women (self-report height and recumbent length). Recumbent length yielded a significantly greater BMI value than all other height estimates for men and two other estimates for women (knee height and armspan length).
We found that self-reported height and knee height had similar differences across sexess whereas recumbent length and armspan length showed differential differences (see Table 5). Because armspan length is not a central measure of height as indicated by the low loading on the common factor, the mean differences (16.85 cm) are less trustworthy than the other measures. In a similar logic because recumbent length is the strongest and most central measure of height, the mean levels of height as indicated by this measure appear most trust worthy. The latent means in height as estimated by the CFA model were estimated at 176. 65 cm for men and 161.02 cm for women (mean difference = 15.63). This mean difference is based on the combined information among all of the indicators (height measures) and is corrected for the degree of unreliability of each indicator.
Returning to Table 5, we see that the manifest indicator that is closest to this estimated latent height difference is recumbent length. Armspan length clearly overestimates the difference in heights and because of its low validity coefficients we can see that armspan should be the last resort for assessing height in this population.
DISCUSSION
Obtaining an accurate height estimate for individuals with severe mobility impairments who use wheelchairs is challenging, as the impairment typically precludes people from standing for measurement with a stadiometer. Further, having an accurate estimate is important for use in equations related to patient care such as determining appropriate drug dosages, assessing pulmonary function, and measuring BMI (formula is weight in kilograms/height in meters2). This study investigated whether four methods of measuring or estimating height among wheelchair users yielded significantly different estimates and examined the accuracy of these estimates. The results demonstrate that various approaches do generate significantly different height estimates and provide evidence supporting recumbent length as the most accurate method. Further, applying these height estimates to the BMI equation also results in significantly different BMI values.
The accuracy of the four methods was assessed using CFA. Based on the variances accounted for by the different methods, recumbent length (92% variance) yielded the most accurate height estimate for wheelchair users. Yet, with knee height accounting for 83%-85% of the common variance and self-report accounting for 75%-83%, both methods also yield reasonable estimates of height.
Armspan length yielded the largest height estimate for both men and women and recumbent length the shortest, and both sexes self-reported their height as significantly greater than their recumbent length. Knee height yielded larger height estimates for both sexes than recumbent length, although the difference was only significant for women.
Selecting the measurement method must be balanced with the need for accuracy as well as logistical and practical issues such as the testing environment, time, and the population. Recumbent measurement requires the testing environment accommodate a table upon which individuals can safely transfer. Additionally, substantial time and effort are needed as some individuals need assistance to transfer as well as remain in the recumbent position. Finally, many wheelchair-users experience contractures or other physical anomalies that prevent them from lying flat even with assistance, especially when paralysis or spasticity restricts autonomous lower limb movement. In these cases, measurement is less precise. Notably, measurement difficulties for recumbent length were recorded for 25% of this sample.
These study findings support the use of the equation for mobility impaired individuals15 to estimate total height based on knee height as a valid alternative. The downside of this approach is that it provides an estimated rather than measured value, and for women differed significantly from their recumbent length. Yet for those unable to lie flat, the knee height estimate may be more accurate than a recumbent measure and notably, the time and effort required to measure knee height is substantially less than for recumbent length. Despite our measuring participants’ knee height from the mat table immediately after obtaining their recumbent length, knee height can be measured from the wheelchair as long as the leg can freely dangle. This can be accomplished by unlocking and swinging away the foot plate on wheelchairs with this feature. Those who opt for fixed footplates likely can transfer easily to an adjustable height exam table from which the leg can dangle. Additional study of this approach with larger mobility impaired samples will provide useful evidence of the accuracy of the approach, and can generate data to improve the prediction equation.
This study also supports self-report as a less, but still reasonably accurate height estimate. Deciding to use self-report should include consideration of two issues. First, most people tend to overestimate their height, and this discrepancy is greater for men. 24-26 In this study, women overestimated their height an average of 2.31 cm and men an average of 3.82 cm. These findings are consistent with those of Garshick et al.4 who reported SCI men overestimated their height by an average of 2.3 cm ± 3.45 cm. Second, reporting inaccuracy for a mobility-impaired sample may be compounded by several factors such as age at disability onset, loss of stature, or recall error. Developmental onset may result in the person not being accurately measured after achieving their full height if they cannot stand. Loss of stature due to aging or other disease processes such as bone demineralization and contractures can contribute to inaccuracy. Additionally, recall error may be greater because of the irregularity or infrequency of measuring height among those who cannot or have difficulty standing.
Finally, the finding that armspan provided the least accurate estimate, with only 38%-42% common variance is similar to those of Garshick4 who reported armspan (and other upper body measures) yielded unacceptably high variability in predicting stature among individuals with SCI. In contrast, evidence supports armspan as a reasonably accurate height estimate for ambulatory young and middle-aged1,8 and ambulatory older adults.10 Although armspan estimates a person’s maximum achievable height, several factors may affect the estimate for those with mobility impairment. People with early onset disability likely never achieved their “maximal” height, in part due to lack of weight bearing on the long leg bones. Also, those with more severe mobility impairment may have physical anomalies, such as joint contractures that restrict full body extension or bone demineralization that contribute to discrepancies between armspan and body length.
Notably, the various height estimates also yielded significantly different BMI values. Because the BMI formula is weight in kilograms divided by height in meters squared, observed differences among these estimates are squared. Differences across BMI values generally followed the pattern observed across height measures; methods that yielded the largest height estimates yielded the lowest BMI values and vice versa. This is not purely an academic concern, given potential surveillance and clinical implications. In terms of population surveillance, using a less accurate height estimate to calculate BMI may result in gross undercounting of wheelchair users or others with serious mobility problems who are overweight or obese. Clinically, this misclassification may result in providers not addressing weight control and healthy eating for many in need. To gauge the extent of this misclassification, we used BMI based on self-reported height as the reference (a commonly used method) and counted the number of participants whose change in BMI altered their weight status (normal, overweight, or obese) when compared against BMI using recumbent height or knee height values. Overall, 34 instances of a weight category change occurred among 26 people (17.7%) as the weight status increased for 24 (17.0%) from normal to overweight (n=14, 9.98.5) or overweight to obese (n=10, 7.1%), and decreased for 10 (4.3%) from obese to overweight (n=6, 4.3%) or overweight to normal (n=4, 2.8%). Specifically, using recumbent length (compared to self-report) for BMI resulted in a weight status increase for 14 people (9.9%) and reduction for 4 (2.8%), while using the knee height estimate resulted in a status increase for 10 people (7.1%) and reduction for 6 (4.3%). Thus, using self-reported height for BMI potentially undercounts those with weight issues and extrapolating to the population-level, these misclassifications are substantial. While problems associated with measuring recumbent length may contribute to some inaccuracy, only 9/34 people whose recumbent length was difficult to measure account for these weight status changes.
Limitations
Several study limitations should be noted. First, results derive from a relatively small sample of longstanding wheelchair users. Thus, additional studies should be conducted with larger sample sizes. Second relates to the sample heterogeneity, as participants differed on several dimensions that may affect height, such as impairment etiology, onset age, condition duration and severity, and ability to stand and walk. This study lacked sufficient sample sizes for specific impairment groups to conduct subanalyses, although the accuracy of a specific method may vary by impairment type. Finally, the measurement difficulties associated with a non-ambulatory sample prevented our ability to obtain participants’ “true height” for comparison. However, we are confident that the statistical modeling techniques employed provide strong support for our conclusions.
CONCLUSIONS
Obtaining a valid height measure for wheelchair users is important to help clinicians provide quality and appropriate health care and to researchers for surveillance and intervention. Evidence from this study suggests that measuring recumbent height yields the most valid method for wheelchair users who cannot stand, but when this measure may not be practical or feasible, measuring knee height or asking people to self-report may be reasonable alternatives.
Acknowledgments
This work was funded by NIH/NICHD grant #R01 HD048628.
Footnotes
Disclosures: Financial disclosure statements have been obtained, and no conflicts of interest have been reported by the authors or by any individuals in control of the content of this article.
These data were presented at the Disability Forum of the 138th Annual American Public Health Association conference in November 2010. The authors have received no financial benefits in conducting this research. Data were collected while Dr. Froehlich-Grobe was at KU, and this paper was submitted after she joined the UT School of Public Health.
References
- 1.Brown J, Whittemore K, Knapp T. Is arm span an accurate measure of height in young and middle-age adults? Clin Nurs Res. 2000;9(1):84–94. doi: 10.1177/10547730022158456. [DOI] [PubMed] [Google Scholar]
- 2.Han T, Lean M. Lower leg length as an index of stature in adults. Int J Obes. 1996;20:21–27. [PubMed] [Google Scholar]
- 3.Roubenoff R, Wilson PWF. Advantage of knee height over height as an index of stature in expression of body composition in adults. Am J Clin Nutr. 1993;57:609–613. doi: 10.1093/ajcn/57.5.609. [DOI] [PubMed] [Google Scholar]
- 4.Garshick E, Ashba J, Tun CG, Lieberman SL, Brown R. Assessment of stature in spinal cord injury. J Spinal Cord Med. 1997;20(1):36–42. doi: 10.1080/10790268.1997.11734580. [DOI] [PubMed] [Google Scholar]
- 5.Watt T, Dodd F, Keegan M, Campbell LT. Accuracy and precision of techniques used for measuring height in critical illness. Manchester, UK: University Department of Anaesthesia, Withington Hospital; 1994. [Google Scholar]
- 6.Hogan SE. Knee height as a predictor of recumbent length for individuals with mobilty-impaired cerebral palsy. J Am Coll Nutr. 1999;18(2):201–205. doi: 10.1080/07315724.1999.10718851. [DOI] [PubMed] [Google Scholar]
- 7.[WHO] WHO. Physical status: The use and interpretation of anthropometry. Geneva: World Heatlh Organization; 1995. p. 854. [PubMed] [Google Scholar]
- 8.Brown J, Feng J, Knapp T. Is self-reported height or arm span a more accurate alternative measure of height? Clin Nurs Res. 2002;11(4):417–432. doi: 10.1177/105477302237454. [DOI] [PubMed] [Google Scholar]
- 9.Haboubi NY, Hudson PR, Pathy MS. Measurement of height in the elderly. J Am Geriatr Soc. 1990;38:1008–1010. doi: 10.1111/j.1532-5415.1990.tb04424.x. [DOI] [PubMed] [Google Scholar]
- 10.Kwok T, Whitelaw M. The use of armspan in nutritional assessment of the elderly. J Am Geriatr Soc. 1991;39:492–496. doi: 10.1111/j.1532-5415.1991.tb02495.x. [DOI] [PubMed] [Google Scholar]
- 11.Bassey J. Demi-span as a measure of skeletal size. Ann Hum Biol. 1986;13(5):449–502. doi: 10.1080/03014468600008661. [DOI] [PubMed] [Google Scholar]
- 12.Chumlea W, Roche A, Steinbaugh M. Estimating stature from knee height for persons 60 to 90 years of age. J Am Geriatr Soc. 1985;33:116–120. doi: 10.1111/j.1532-5415.1985.tb02276.x. [DOI] [PubMed] [Google Scholar]
- 13.Chumlea C, Guo S. Equations for predicting stature in white and black elderly individuals. J Gerontol (A Biol Sci Med Sci) 1992;47(6):M197–M203. doi: 10.1093/geronj/47.6.m197. [DOI] [PubMed] [Google Scholar]
- 14.Canda A. Statue estimation from body segment lengths in young adults - application to people with physical disabilities. Journal of Physiological Anthropology. 2009;28(2):71–82. doi: 10.2114/jpa2.28.71. [DOI] [PubMed] [Google Scholar]
- 15.Chumlea C, Guo S, Steinbaugh M. Prediction of stature from knee height for black and white adults and children with application to mobility-impaired or handicapped persons. J Am Diet Assoc. 1994;94:1385–1388. 1391. doi: 10.1016/0002-8223(94)92540-2. [DOI] [PubMed] [Google Scholar]
- 16.Johnson R, Ferrara M. Estimating stature from knee height for persons with cerebral palsy: An evaluation of estimation equations. J Am Diet Assoc. 1991;91(10) [PubMed] [Google Scholar]
- 17.Spender QW, Cronk CE, Charney EB, Stallings VA. Assessment of linear growth of children with cerbral palsy: Use of alternative measures to heigjt or length. Dev Med Child Neurol. 1989;31(2):206–214. doi: 10.1111/j.1469-8749.1989.tb03980.x. [DOI] [PubMed] [Google Scholar]
- 18.Nary DE, Froehlich-Grobe K, Aaronson L. Recruitment issues in a randomized controlled exercise trial targeting wheelchair users. Contemporary Clinical Trials. 2011;32(2):188–195. doi: 10.1016/j.cct.2010.10.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.SPSS Inc. SPSS Base 16.0.2 for Windows User’s Guide. Chicago: SPSS Inc; 2008. [Google Scholar]
- 20.SAS Institute. SAS/STAT 9.1 user’s guide. Cary, NC: SAS Institute Inc; 2004. [Google Scholar]
- 21.Enders CK. Applied missing data analysis. New York, NY: Guilford Press; in press. [Google Scholar]
- 22.Brown RL. Assessing specific mediational effects in complex theoretical models. Structural Equation Modeling. 1997;4:142–156. [Google Scholar]
- 23.Little TD, Slegers DW, Card NA. A non-arbitrary method of identifying and scaling latent variables in SEM and MACS models. Structural Equation Modeling. 2006;13:59–72. [Google Scholar]
- 24.Prince SA, Adamo KB, Hamel ME, Hardt J, Connor Gorber S, Tremblay M. A comparison of direct versus self-report mesasures for assessing physical activity in adults: A systematic review. International Journal of Behavioral Nutrition and Physical Activity. 2008;5(56):24. doi: 10.1186/1479-5868-5-56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Shields M, Gorber SC, Tremblay M. Estimates of obesity based on self-report versus direct measures. Health Rep. 2008 June;19(2):1–16. [PubMed] [Google Scholar]
- 26.Palta M, Prineas RJ, Berman R, Hannon P. Comparison of self-reported and measured height and weight. Am J Epidemiol. 1982;115:223–230. doi: 10.1093/oxfordjournals.aje.a113294. [DOI] [PubMed] [Google Scholar]