

Abstract
Noncompliance with labor and occupational health and safety laws contributes to economic and health inequities. Environmental health agencies are well positioned to monitor workplace conditions in many industries and support enhanced enforcement by responsible regulatory agencies. In collaboration with university and community partners, the San Francisco Department of Public Health used an observational checklist to assess preventable occupational injury hazards and compliance with employee notification requirements in 106 restaurants in San Francisco's Chinatown. Sixty-five percent of restaurants had not posted required minimum wage, paid sick leave, or workers' compensation notifications; 82% of restaurants lacked fully stocked first-aid kits; 52% lacked antislip mats; 37% lacked adequate ventilation; and 28% lacked adequate lighting. Supported by a larger community-based participatory research process, this pilot project helped to spur additional innovative health department collaborations to promote healthier workplaces.
In the 20th century, labor laws such as child labor protections, occupational safety standards, wage and hour rules, and the right to collective bargaining have played a critical role in mitigating health inequities by protecting and improving worker and population health.1–4 However, the ability of regulatory agencies to monitor and enforce health-protective labor standards is significantly undermined by inadequate funding and growth of the informal and unregulated economy.5–9 Partnerships among local and state agencies, research institutions, community-based organizations, and worker centers may help fill regulatory gaps.10,11 Collaborations in New York, California, and Illinois have proven successful in documenting conditions faced by immigrant, low-wage, and other hard-to-reach workers; promoting policy change; and facilitating stronger enforcement of wage and hour laws and access to workers' compensation.7,12–15 Given their role in local enforcement of businesses such as restaurants, local health and environmental health agencies may be particularly well situated to help address unhealthy conditions in workplaces.16,17
This article shares the experience of one local health agency, working in collaboration with community and university partners, to develop and apply an instrument to observe workplace hazards and labor law violations in restaurants. The research aims of this project were to (1) assess labor law compliance and workplace hazards in restaurants in one San Francisco, California, neighborhood; (2) assess the feasibility of using an observational checklist to routinely monitor workplace conditions in the course of regulatory inspections; and (3) assess the relationship between observed workplace hazards and food safety scores. Consistent with community-based participatory research (CBPR) principles of generating collective understanding and action to address a priority social problem,18–20 this article describes the process of creating and applying the checklist and the findings from this application. We discuss lessons learned regarding the utility of the checklist as a data-collection instrument and the feasibility of incorporating the checklist into routine environmental inspections. Finally, we discuss the impacts of the assessment on the San Francisco Department of Public Health (SFDPH) and its relevance for environmental health practice.
BACKGROUND
The restaurant industry, which includes food services and drinking establishments, is one of the largest private-sector employers in the United States, employing more than 9.3 million workers nationwide.21 Wages for many restaurant workers are very low (the average is $10.04 an hour, compared with $20.90 an hour for all occupations),22 and known occupational hazards include sprains and strains from falls, slips, and lifting; cuts from knives and food processors; and burns.23 Occupational injuries and illnesses can be prevented with proper training, the provision of safety equipment, and mitigation of physical hazards.24 Research has also shown that employer provision of a livable wage, health insurance, and paid sick days can help decrease premature death, hunger, homelessness, risk of early childbirth, and transmission of communicable diseases, as well as improve access to primary and preventive care.25–27
Similar to restaurants in other urban areas,7,13,28 workers in San Francisco's Chinatown restaurants experience low-wage jobs with long hours, few benefits, and exposure to dangerous and often unlawful workplace conditions. According to a recent survey of 433 Chinatown restaurant workers, 95% of workers earned less than a living wage, 50% earned less than minimum wage, 42% never received paid sick days, 31% never received their full wages owed, and only 3% received health insurance from their employers. Work-related injury rates were also high, with 48% of workers reporting work-related burns, 40% reporting cuts, and 17% reporting falls in the previous year, with significantly higher injury rates among cooks. At the same time, 61% of workers reported some bodily pain in the four weeks prior, 25% reported a significant level of psychological stress, and 64% reported not receiving any on-the-job training. (Unpublished report. Salvatore A, Krause N. Health and working conditions of restaurant workers in San Francisco's Chinatown: report of preliminary survey findings. San Francisco: March 2010.)18,29
In 2006, community organizers from the Chinese Progressive Association and researchers from the University of California, Berkeley, School of Public Health/Labor Occupational Health Program, and the University of California, San Francisco, Division of Occupational and Environmental Medicine approached the staff of SFDPH's Program on Health, Equity, and Sustainability to collaborate on a project to document and address work conditions of immigrant restaurant workers in San Francisco's Chinatown. Initiated as part of a larger CBPR study, the project involved the collective development and administration of two instruments—a restaurant worker survey and an observational checklist of restaurant conditions—to gather individual- and restaurant-level data about environmental, organizational, and individual factors affecting Chinatown restaurant workers' health. This article focuses on the checklist creation and application to conduct observations in Chinatown restaurants. We also describe how participation has affected SFDPH environmental health practice. Detailed descriptions of the worker survey development and survey findings are described elsewhere. (Unpublished report. Salvatore A, Krause N. Health and working conditions of restaurant workers in San Francisco's Chinatown: report of preliminary survey findings. San Francisco: March 2010.)18,29
METHODS
Development of an observational instrument
Checklist development was a collective process and informed by a literature review, state occupational safety and health recommendations, and interviews with restaurant workers and SFDPH food safety inspection staff.18 Checklist observations included (1) the number and gender of employees, (2) legally required notifications (posters) of three labor laws, (3) common occupational hazards, and (4) protective equipment to mitigate hazards and prevent injuries. The checklist did not include items deemed to be time intensive or intrusive to restaurant work (e.g., opening cabinets or interfering with employees' work). Restaurant workers involved in the development and administration of the worker survey made suggestions that improved the checklist (e.g., whether first-aid kits were not only available but also fully stocked and whether required notifications were available in Chinese). Additional items identified during pilot testing (e.g., ventilation and machine guards) were also added.
Data collection
One SFDPH staff member observed food establishments in the Chinatown area of San Francisco that had a kitchen and sold prepared, non-prepackaged food, including takeout restaurants, regardless of whether seating space was available. SFDPH food safety inspectors supported this staff member in gaining access to restaurants and understanding communication protocols and the needs of restaurant staff and management. SFDPH student interns provided Cantonese/Mandarin interpretation. From March 2008 through August 2008, SFDPH collected data at 106 Chinatown restaurants, including 10 restaurants involved in an initial pretest evaluation. Checklist implementation took approximately 10–15 minutes to conduct.
We retrieved restaurant food safety scores from the SFDPH Environmental Health Database to explore any relationship between the food safety score (an indicator of consumer safety violations) and labor law notifications or observable workplace hazards (indicators of worker safety violations). The food safety score is a weighted measure of serious violations observed during regular food safety inspections.30 Food safety scores range from 0 to 100, with 100 being an establishment with no violations.
Data analysis
We tabulated frequencies for all checklist items including gender and location of workers. We created a composite score of 11 checklist items to represent a summary measure of observed occupational hazards and absence of protective equipment. The composite score did not include observed labor law notification postings, which were analyzed separately, or the presence of fully stocked first-aid kits, which may be considered treatment rather than hazards.
Statistical analyses were conducted using Stata® version 11.31 We explored the relationship between checklist variables and restaurants' food safety scores using simple linear regression and correlation analyses. We compared mean composite scores across the three food safety score categories (poor: 0–79, adequate: 80–89, and excellent: 90–100) using analysis of variance. To analyze the relationship between postings of labor law notifications and food safety scores, we conducted correlation analyses.
RESULTS
We observed working conditions using the checklist instrument in 106 of 108 restaurants within San Francisco Chinatown census tracts from March to August 2008.
Workers and worker demographics
During observations, SFDPH counted a total of 813 restaurant workers (mean = 7.7 workers per restaurant), including 370 females and 443 males. Kitchen or “back of the house” workers, who typically have no direct contact with customers, included cooks, dishwashers, bakers, and butchers working in the kitchen/back area. Restaurant or “front of the house” workers, who have customer contact, included hostesses, busboys, cashiers, waitresses, counter people at coffee shops, and butchers working at meat market counters. SFDPH observed that females were more likely to be working in “front of the house” (66% female vs. 34% male) than “back of the house” (30% female vs. 70% male) positions.
Posting of employee labor law notifications
Table 1 presents the number of observed labor law notifications in English and Chinese. Of the 106 restaurants observed, 65% did not have any of the three selected employee notifications posted in a visible location in any language. Of the 37 restaurants that did have at least one labor law posted, 10 (27%) had the poster in English only, and 15 (41%) had only one of three posters posted.
Table 1.
Checklist findings—observed noncompliance with employee notification requirements of select California and San Francisco labor laws: Chinatown Restaurant Worker Health Project, San Francisco, 2008
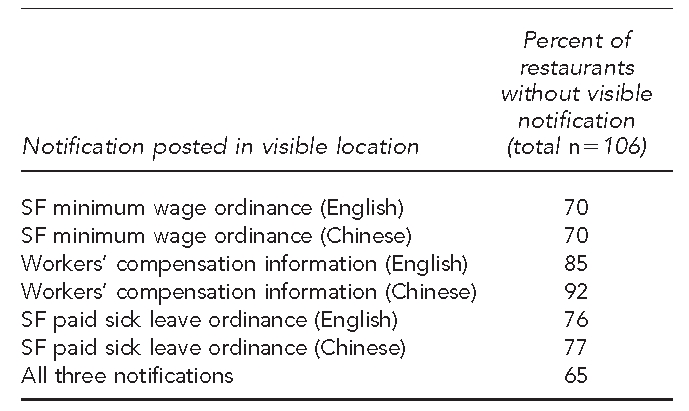
SF = San Francisco
Exposure and protection from hazards
Observed preventable occupational hazards were common (Table 2). The majority of kitchens visited were small and had cooks working at overcrowded range tops (70%). In part due to limited storage space in small kitchens, many employers stored food supplies, cookware, and empty boxes by the exits, occasionally blocking the establishment's emergency exits (7%). The vast majority of cooks did not wear long-sleeve shirts (90%), which may mitigate or prevent burns, and 96% of the restaurant workers only used rags to hold hot items.
Table 2.
Checklist findings—observed preventable occupational hazards: Chinatown Restaurant Worker Health Project, San Francisco, 2008
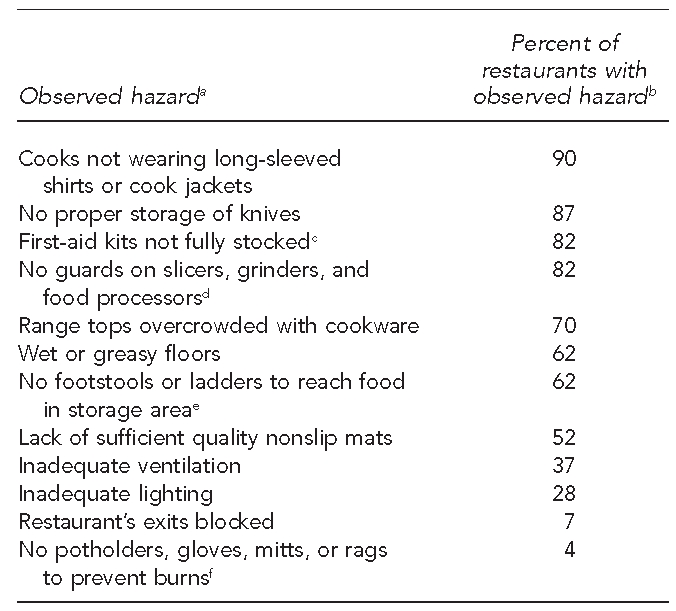
aHazards observed included the presence of common occupational hazards (e.g., slippery/wet floors) and the absence of protective safety equipment and features to mitigate hazards and prevent injuries (e.g., slicing guards).
bTotal n=106, except where noted
cOnly 19 of the 106 restaurants (18%) had a fully stocked first-aid kit at the time of observation. Of the remaining restaurants, 13 did not have any first-aid kit, and 74 had only adhesive bandages.
dOnly four of the 22 restaurants with a slicer, grinder, and/or food processor had a protective guard. This item was not applicable to 79% of restaurants (n=84).
eOnly five of the 13 restaurants that stored food in a hard-to-reach area had a footstool or ladder present at the time of observation. This item was not applicable to 88% of restaurants (n=93).
fAll restaurants observed with burn-prevention materials for handling hot foods (n=102/106) used rags to prevent burns. Potholders, gloves, and mitts were rarely observed.
Sixty-two percent of the establishments visited had wet and greasy floors, creating hazards for slips and falls. Although the majority of establishments visited used some materials covering floors to address wet conditions, more than half of all restaurants (52%) lacked mats specifically designed to prevent slips and falls. Some of the mats and pallets observed were in poor condition and slippery as a result of the accumulated grease and exposure to water.
Eighty-seven percent of restaurants observed lacked proper storage of knives on the counters or walls, 37% lacked adequate ventilation, and 28% lacked adequate lighting. Although 70% of restaurants had bandages available, 82% of restaurants did not have fully stocked first-aid kits. Finally, 18 of the 22 establishments (81%) that slice, grind, or process food did not have any visible guards for their slicing, grinding, and food processing machines.
Association among labor law notifications, observed working conditions, and food safety scores
We found no significant correlation between the number of labor law notification postings in each language and food safety scores (p=0.13 for English postings and p=0.17 for Chinese postings). We also found no association between the individual restaurant composite hazard and food safety scores (β=4.5, p=0.61), whether food safety scores were considered as a continuous or categorical variable.
DISCUSSION
We believe this assessment was unique in that it considered both physical occupational hazards and noncompliance with labor rules simultaneously in workplaces. Observations documented a substantial lack of compliance with local and state employee labor law notification requirements. We observed few required labor notices in Chinese, despite the fact that more than 60% of Chinatown residents32 and 95% of surveyed restaurant workers do not speak English well.29 Observations documented a high frequency of occupational hazards and a lack of protective safety equipment for workers in Chinatown. Although we did not find a correlation between observed hazards in restaurants and their consumer food safety scores, others have found an association between labor law and safety violations,33 suggesting the need for additional data collection and analysis.
Feasibility of using the checklist in routine environmental health inspections
This project sought to assess whether the checklist could be feasibly integrated into the course of routine restaurant inspections. Although SFDPH is not the enforcement agency for most labor and safety laws, local restaurant inspectors are potentially well placed to observe safety hazards, refer potential violations to responsible regulatory agencies, and educate restaurant employers on both labor law requirements and hazard-reduction practices. A correlation between observed hazards, labor law violations, and food safety scores could potentially be used to help target enforcement efforts.
Our experience suggests that the checklist implementation itself is not time-consuming. However, restaurant inspectors suggested that explanation of findings to restaurant operators and discussion of a large number of observed deficiencies would require substantial time and resources. SFDPH restaurant inspectors also noted that investment of time and intentional relationship building with employers, owners, and workers are key components of preventing and addressing food safety violations. Some inspectors expressed concerns that monitoring for labor and occupational health conditions might detract from their responsibility to monitor for consumer food safety.
Inspectors also noted that the checklist assumes that observed hazardous conditions can be feasibly mitigated. Although some preventive measures, such as antislip mats, are relatively cheap and easy to install, other improvements, such as replacing an exhaust ventilation system, may be prohibitively expensive, especially when managers rent their restaurant space.
A feasibility assessment for long-term application of the checklist would need to explore organizational commitment requirements, resources to support significant additional inspector training and time, responsive target agencies for referral, and clear advice for action in response to observed deficiencies. The impact of a local monitoring system for worker health by a local environmental regulatory agency also depends on effective communication with and responsive action by designated enforcement agencies. SFDPH anticipates that ongoing conversations and collaborations with enforcement agencies, businesses receiving SFDPH health permits, and worker centers will result in additional ideas and actions to promote healthier workplaces and stronger enforcement.
Relevance to local environmental health practice
The process of collaborating with local community partners helped identify a priority issue area and potential actions that the local health department could take to address the issue.11,34 The findings of the study motivated SFDPH administrators to explore other ways to more comprehensively assure their legislative mandate to ensure compliance with health-relevant laws in facilities they permit. Following this project, three inspectors independently assessed 198 restaurants both within and beyond Chinatown for six labor law notifications, finding noncompliance in more than 70% of restaurants. SFDPH instructed restaurants on how to obtain proper signage and made referrals to the appropriate state or local enforcement agency. Furthermore, in May 2009, SFDPH began requiring proof of workers' compensation coverage for all new and change-of-business health permit requests. To evaluate compliance with workers' compensation, SFDPH asked 400 randomly selected establishments to demonstrate proof of insurance. Of the 400, more than 20 businesses obtained workers' compensation insurance to comply with the regulations following contact with SFDPH.
SFDPH is collaborating with the local Office of Labor Standards Enforcement (OLSE) to enforce restaurant compliance with local minimum wage, paid sick leave, and health-care contribution requirements. SFDPH has temporarily revoked health permits for businesses with unresolved local labor violations. SFDPH and OLSE are also exploring ways to better coordinate data systems to identify violators and repeat offenders. The Figure outlines additional potential strategies that local health departments might use to improve labor and safety conditions for low-wage and immigrant workers.
Figure 1.
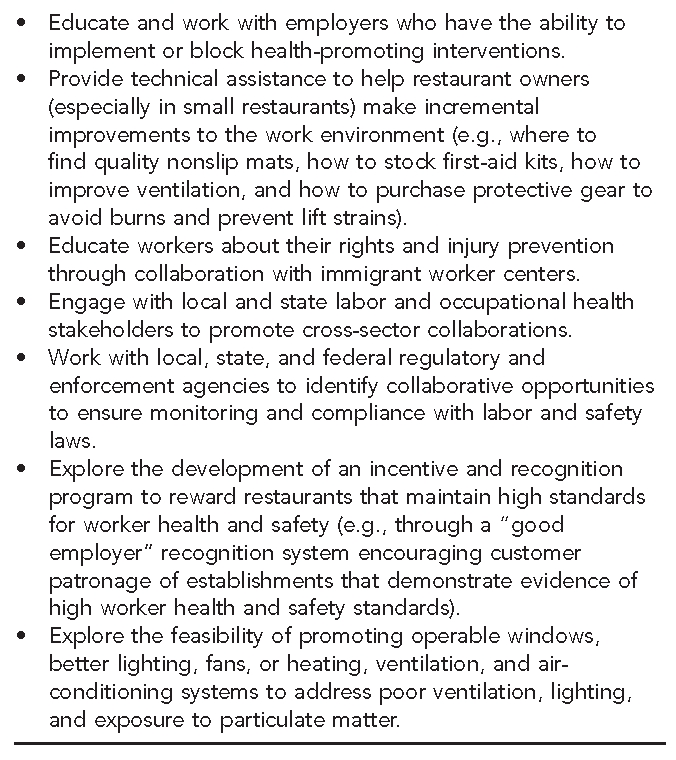
Potential local public health agency actions to improve compliance with labor laws and occupational safety standards in restaurants: Chinatown Restaurant Worker Health Project, San Francisco, 2008
Strengths and limitations
An important strength of this assessment related to the CBPR process35 was the involvement of impacted stakeholders in checklist development and interpretation of findings. Both environmental health inspectors and restaurant workers contributed to the interpretation of findings. For example, health inspectors noted that sometimes interventions (e.g., cheap rubber mats to prevent falls or long sleeves to prevent burns) may result in other ergonomic or occupational hazards (e.g., lack of cushioning in some mats when standing for long hours, or inadvertently increasing the risk of sleeves being caught in flames, ovens, or slicers). Restaurant workers noted that they observed machine guards in Western restaurants but not in Chinese ones and that large food canisters are regularly used as footstools.
Our checklist application had several limitations, including a lack of standardized metrics, lack of observation of actual work practices, variable inspection timing, heterogenity in restaurant types, and focus on one neighborhood. Because one staff person conducted all 106 inspections, there was likely higher internal consistency across restaurants observed. However, external reliability and generalizability would benefit from standardized definitions of concepts such as “adequacy” of lighting and ventilation, “overcrowding” of oven ranges, and ”sufficient quality” of nonslip mats.36 Potentially, measurement tools such as light meters and particulate air pollutant monitors could increase objectivity.
The checklist alone does not provide evidence that observed conditions result in poor health and welfare among workers. The presence of first-aid kits, machine guards, and employee hand-washing stations in restaurants does not guarantee that workers are able to access and utilize them when needed or that they use them effectively. Similarly, the posting of labor laws in a visible location is not necessarily a proxy for employer compliance with wage and labor laws. The checklist also did not capture work pace (e.g., rushing) and other psychosocial factors that may affect actual injuries. In the future, we intend to analyze relationships among observed restaurant hazards and health outcomes (as measured by the worker survey).
The variation in time of observations relative to cycles of business operation may have affected results. Most checklist observations were conducted in the morning to avoid being intrusive to restaurant work; this may have resulted in underestimating the prevalence of wet, greasy floors and related problems that intensify during peak business hours. Subsequent applications could conduct observations at similar times of day or analyze associations among hazards and the time of day. Our sample included diverse establishment types, including meat markets, bakeries, cafes, and other eating establishments, whose conditions may vary significantly from restaurants and from each other. Broader application of this checklist may benefit from disaggregating findings by business type.
CONCLUSION
This assessment demonstrated the substantial occupational hazards facing vulnerable workers in San Francisco's Chinatown. The study also highlighted the potential of community, academic, and governmental collaborations to support compliance with labor and health and safety laws at a community level. In the future, local environmental health agencies could develop an important role in the enforcement of occupational health and safety laws though routine monitoring of working conditions and coordinated compliance activities with responsible enforcement agencies.
Acknowledgments
The authors thank the project's organizational partners including Robin Baker of the University of California, Berkeley, Labor Occupational Health Program; Alex Tom and Fei Ye Chen of the Chinese Progressive Association (CPA); the members of CPA's Restaurant Workers' Leadership Group; Henning Chu, Alex Cooper, Elizabeth Hom, and Margaret Lee, the Occupational Health Internship Program (OHIP) interns who contributed to the original checklist development; the San Francisco Department of Public Health (SFDPH) environmental health inspectors who provided input on project development; June Weintraub for support with data analysis; Natalie Gee and Qi Ting Zhao for help with interpretation during checklist administration; and Karen Yu for her work to support SFDPH's internal capacity building to address labor law violations.
The Worker Health and Safety in Chinatown Restaurants study was funded by the National Institute for Occupational Safety and Health (NIOSH) (1R21OH009081-01) and The California Endowment and received additional support from OHIP. The contents of this article are solely the responsibility of the authors and do not necessarily represent the official views of NIOSH, The California Endowment, or OHIP, or the official policies of the City and County of San Francisco. Mention of the SFDPH does not imply its endorsement.
REFERENCES
- 1.Benach J, Muntaner C, Santana V Employment Conditions Knowledge Network. Employment conditions and health inequalities. Final report to the World Health Organization Commission on Social Determinants of Health. 2007. [cited 2011 Feb 15]. Available from: URL: http://www.who.int/social_determinants/resources/articles/emconet_who_report.pdf.
- 2.Marlenga B, Berg RL, Linneman JG, Brison RJ, Pickett W. Changing the child labor laws for agriculture: impact on injury. Am J Public Health. 2007;97:276–82. doi: 10.2105/AJPH.2005.078923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.National Institute for Occupational Safety and Health (US) Delivering on the nation's investment in worker safety and health. NIOSH publication no. 2010-122. Washington: Department of Health and Human Services (US); 2009. [Google Scholar]
- 4.Mischel L, Walters M. How unions help all workers. Economic Policy Institute briefing paper no. 143. Washington: EPI; 2003. [Google Scholar]
- 5.Bernhardt A, Boushey H, Dresser L, Tilly C, editors. Confronting the gloves-off economy: America's broken labor standards and how to fix them. Champaign (IL): Labor and Employment Relations Association; 2008. [Google Scholar]
- 6.Lashuay N, Harrison R. Barriers to occupational health services for low-wage workers in California: a report to the Commission on Health and Safety and Workers' Compensation, California Department of Industrial Relations. San Francisco: CHSWC; 2006. [Google Scholar]
- 7.Bernhardt A, Milkman R, Theodore N, Heckathorn D, Auer M, DeFilippis J, et al. Broken laws, unprotected workers: violations of employment and labor laws in America's cities. Chicago, New York, Los Angeles: University of Illinois at Chicago, Center for Urban Economic Development; National Employment Law Project; University of California, Los Angeles, Institute for Research on Labor and Employment; 2009. [Google Scholar]
- 8.American Federation of Labor—Congress of Industrial Organizations. Death on the job: the toll of neglect. A national and state-by-state profile of worker safety and health in the United States. 19th ed. Washington: AFL-CIO; 2010. [Google Scholar]
- 9.Government Accountability Office (US) Department of Labor: wage and hour division needs improved investigative processes and ability to suspend statute of limitations to better protect workers against wage theft. Report to the Committee on Education and Labor, House of Representatives. GAO-09-629. Washington: GAO; 2009. [Google Scholar]
- 10.Schulz AJ, Israel BA, Parker EA, Lockett M, Hill Y, Wills R. The East Side Village Health Worker Partnership: integrating research with action to reduce health disparities. Public Health Rep. 2001;116:548–57. doi: 10.1016/S0033-3549(04)50087-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Wallerstein N, Duran B. Community-based participatory research contributions to intervention research: the intersection of science and practice to improve health equity. Am J Public Health. 2010;100(Suppl 1):S40–6. doi: 10.2105/AJPH.2009.184036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.National Institute for Occupational Safety and Health (US) NIOSH-funded research grants. [cited 2010 May 20]. Available from: URL: http://www.cdc.gov/niosh/programs/ohd/grants.html.
- 13.Restaurant Opportunities Center United. New York: ROC-United; 2011. [cited 2010 May 20]. Behind the kitchen door: a multi-site study of the restaurant industry. Also available from: URL: http://www.rocunited.org/files/1101_BKD_EXEC_final.pdf. [Google Scholar]
- 14.New York State Department of Labor. Labor Department initiative empowers ordinary people to join fight against wage theft [press release]; 2009 Jan 26. [cited 2010 May 20]. Available from: URL: http://www.labor.state.ny.us/pressreleases/2009/Jan26_2009.htm.
- 15.California Department of Industrial Relations. Department of Industrial Relations partners with community-based organizations to provide extra assistance to injured workers [press release]; 2009 May 28. [cited 2010 May 20]. Available from: URL: http://www.dir.ca.gov/dirnews/2009/ir2009-18.html.
- 16.Parker E, Margolis LH, Eng E, Henríquez-Roldáan C. Assessing the capacity of health departments to engage in community-based participatory public health. Am J Public Health. 2003;93:472–6. doi: 10.2105/ajph.93.3.472. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Brosseau LM, Parker DL. Interventions: advancing the state of the art. Public Health Rep. 2009;124(Suppl 1):1–3. doi: 10.1177/00333549091244S101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Minkler M, Lee PT, Tom A, Chang C, Morales A, Liu SS, et al. Using community-based participatory research to design and initiate a study on immigrant worker health and safety in San Francisco's Chinatown restaurants. Am J Ind Med. 2010;53:361–71. doi: 10.1002/ajim.20791. [DOI] [PubMed] [Google Scholar]
- 19.Israel BA, Parker EA, Rowe Z, Salvatore A, Minkler M, López J, et al. Community-based participatory research: lessons learned from the Centers for Children's Environmental Health and Disease Prevention Research. Environ Health Perspect. 2005;113:1463–71. doi: 10.1289/ehp.7675. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Minkler M. Using participatory action research to build healthy communities. Public Health Rep. 2000;115:191–7. doi: 10.1093/phr/115.2.191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Bureau of Labor Statistics (US) Employment, hours, and earnings from the Current Employment Statistics survey, 2010. [cited 2011 Feb 15]. Available from: URL: http://data.bls.gov/pdq/querytool.jsp?survey=ce.
- 22.Bureau of Labor Statistics (US) Occupational employment statistics 2009: national occupational employment and wage estimates. [cited 2010 May 3]. Available from: URL: http://www.bls.gov/oes/current/oes_nat.htm.
- 23.Webster T. Occupational hazards in eating and drinking places. Compensation and Working Conditions [serial online] 2001 Summer. [cited 2010 May 20]. Available from: URL: http://www.bls.gov/opub/cwc/archive/summer2001art4.pdf.
- 24.Department of Labor (US), Occupational Safety and Health Administration. 40 OSHA. [cited 2011 Feb 15]. Available from: URL: http://www.osha.gov/osha40.
- 25.Bhatia R, Katz M. Estimation of health benefits from a local living wage ordinance. Am J Public Health. 2001;91:1398–402. doi: 10.2105/ajph.91.9.1398. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Cole BL, Shimkhada R, Morgenstern H, Kominski G, Fielding JE, Wu S. Projected health impact of the Los Angeles City living wage ordinance. J Epidemiol Community Health. 2005;59:645–50. doi: 10.1136/jech.2004.028142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Bhatia R, Farhang L, Heller J, Capozza K, Melendez J, Gilhuly K, et al. A health impact assessment of the California Healthy Families, Healthy Workplaces Act of 2008. Oakland (CA): Human Impact Partners and San Francisco Department of Public Health; 2008. [Google Scholar]
- 28.Koreatown Immigrant Workers Alliance; Special Service for Groups. At risk in the restaurant: perilous health and safety conditions in one of Koreatown's key industries. Los Angeles: KIWA; 2007. [Google Scholar]
- 29.Chinese Progressive Association. Check, please' Health and working conditions in San Francisco Chinatown restaurants. San Francisco: CPA; 2010. [cited 2010 Oct 9]. Also available from: URL: http://www.cpasf.org/downloads/CPA%20full%20report_ENG.pdf. [Google Scholar]
- 30.San Francisco Department of Public Health. Food safety program. [cited 2010 Apr 28]. Available from: URL: http://www.sfdph.org/dph/EH/Food/Inspections.asp.
- 31.StataCorp LP. Stata®: Release 11. College Station (TX): StataCorp LP; 2009. [Google Scholar]
- 32.Health Development Measurement Tool. Proportion of non-English speaking population (2000) [cited 2010 Apr 28]. Available from: URL: http://www.thehdmt.org/indicators/view/168.
- 33.Restaurant Opportunities Center of New York; Restaurant Opportunities Centers United; New York City Restaurant Health and Safety Taskforce; New York City Restaurant Industry Coalition. Burned: high risks and low benefits for workers in the New York City restaurant industry. New York: ROC-NY and ROC-United; 2009. [Google Scholar]
- 34.Minkler M. Linking science and policy through community-based participatory research to study and address health disparities. Am J Public Health. 2010;100(Suppl 1):S81–7. doi: 10.2105/AJPH.2009.165720. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Israel BA, Schulz AJ, Parker EA, Becker AB. Review of community-based research: assessing partnership approaches to improve public health. Annu Rev Public Health. 1998;19:173–202. doi: 10.1146/annurev.publhealth.19.1.173. [DOI] [PubMed] [Google Scholar]
- 36.Courtney TK, Verma SK, Huang YH, Chang WR, Li KW, Filiaggi AJ. Factors associated with worker slipping in limited-service restaurants. Inj Prev. 2010;16:36–41. doi: 10.1136/ip.2009.022749. [DOI] [PubMed] [Google Scholar]