

Introduction
Botulinum neurotoxin (BoNT) has proved to be a remarkably effective therapy for numerous movement disorders associated with muscle overactivity such as dystonia and related disorders, as well as spasticity [Table 1]. Additional therapeutic benefits accrue from actions such as blockade of acetylcholine release at autonomic nerve analysis as well as the blockade of release of nonacetylcholine transmitters at peripheral nerve endings.
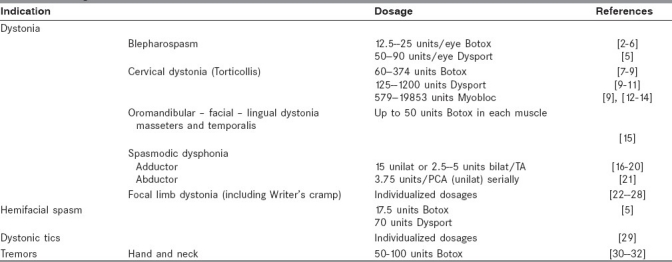
Table 1.
Dosage of botulinum toxin for various indications
Three broad categories of undesirable side effects are seen with BoNT. These are[1] diffusion of toxin into neighboring muscles and nerve endings,[2] sustained neuro-transmission blockade producing effects akin to anatomic denervation, and[3] development of antibodies to BoNT with subsequent immunoresistance.[1]
Indications
Most appropriate conversion factor between Botox and Dysport units is less than 3 in cervical dystonia.[7]
Relative Contraindications
These include any excessive weakness, fixed contractures and neuromuscular disease such myasthenia gravis, Eaton-Lambert syndrome, and motor neuron disease. Other relative contraindications include pregnancy and lactation and the concurrent use of aminoglycosides.
Assessment
This would include a detailed clinical examination and a video analysis for later comparative evaluation. Patient education and counseling are essential and treatment goals should be agreed and documented. Consent should be obtained and BoNT should be prescribed. Secondary causes of treatable dystonia such as drugs or Wilson's disease should be ruled out. Physicians administering BTX should have a good understanding of both the anatomy of affected muscles and the resultant movement disorder. EMG monitoring helps diagnose the underlying disorder and identify appropriate muscles for injection.
Goals for Treatment
Dystonia
Treatment of focal dystonia with BoNT is designed to improve the patients’ postures and function and to relieve associated pain. BoNT temporarily weakens dystonic muscles, thereby allowing more normal posture and function. The benefits that BONT conveys to a particular patient depend on the localization and relative degree of severity of the dystonic muscles being injected. The decision to combine injections of BTX-A with other forms of treatment for dystonia is based on associated factors and individual decision.
Blepharospasm
Blepharospasm may be idiopathic or induced by drugs such L-dopa or neuroleptics. It needs to be differentiated from facial tics in patients with Tourette's syndrome and apraxia of eyelid opening.
The injections are done on an outpatient basis. Intradermal injection with a 27--30-gauge needle is recommended. Typically 3--5 points around each eye are injected. The principle is to avoid the midportion of the upper eyelid to avoid inadvertent diffusion into the levator palpebrae superiors, which would lead to undesirable ptosis.
Focal hand dystonia
Among these, Writer's cramp is the most common form of occupational dystonia. However, these has been described in those professional whose work involves frequent and repetitive movements such as musicians, typists, milkers, cashiers, cobblers, ticket collectors, and seamstresses. Neurologic evaluation and nerve conduction studies are required to rule out radiculopathy or peripheral nerve involvement such as ulnar neuropathy or median entrapment neuropathy at the rest. Doses used for writer's cramps are 5 U for small muscles and 10-20 U for muscles in the forearm. Benefit has been reported in as many as 80%--90% patients and is usually apparent 5--7 days after injection.
Cervical Dystonia
The movements of the neck – rotation, anterior, and posterior flexion, tilt, and shift in the antero--posterior or lateral planes – can occur in any combination in cervical dystonia. This can be associated with shoulder involvement as well as jerky or tremulous movements and also pain. Muscles involved in the abnormal posturing are isolated using standard anatomic landmarks. The most commonly injected muscles include sternocleidomastoid, trapezius, splenius capitis, levator scapulae, and scalene complex. Usually 2--6 muscles are injected at muscle sites. The BTX should be injected along the belly of the muscle to allow for adequate diffusion. Comella et al.[33] reported a significantly greater magnitude of improvement in those cases where the treated neck muscles were selected by clinical and electromyographic guidance than the cases in which only clinical examination was used.
Oromandibular dystonia
This typically involves the masticatory, lower facial, and tongue muscles and is associated with jaw deviation and spasm. BTX should be injected into the inappropriately contracting muscles in different combinations including masseter, temporalis lateral pterygoids, and submental muscles. The lingual muscles need to be injected carefully.
Laryngeal dystonia
They are three types---adductor spasmodic dysphonia (strained strangled voice), abductor spasmodic dysphonia (whispering voice), and adductor breathing dysphonia (paradoxical vocal fold motion). The thyroaarytenoid muscles are located with EMG guidance, and percutaneous injections of BTX are administered through the cricothyroid membrane. Bilateral injection approach is the most common technique for adductor dysphonia, while for the rarer abductor variety unilateral injections are done serially into the posterior cricoarytenoid muscles.
Hemifacial spasm
This can be a very disabling disease because severely affected individuals are socially handicapped and functionally blind. This can involve any combination of orbicularis oculi, frontalis, risorius, zygomaticus major, and platysma muscles. Injections of BTX are given according to the muscles in spasm which differ from patient to patient.
Palatal Tremor (myoclonus)
This may be idiopathic or symptomatic. BTX injection of the tensor veli palitini muscle may reduce the symptom by reducing the amplitude of myoclonic jerk.
Bruxism
This is an involuntary chewing such as rhythmic jaw movement occurring especially at night, with grinding of the teeth. In this disease, BoNT is injected into the most sore part of the muscle, weakening the most spastic part of the masseter muscle without affecting the ability to chew.
Tics
These can be either motor or phonic tics. Both of these can be simple or complex and also classified as clonic, tonic, and dystonic. BoNT produces significant decrease in both tic frequency and urge to tic. It improves the quality of life as reported by the patients. One has to be cautious of producing hypophonia.
Outcome measurement and follow up
Measurement methods include the use of physical measures, techniques to quantify individual symptoms or benefits, such as visual analogs scales and verbal scales as well as other rating scales. Follow-up appointment should be at approximately 3--17 weeks post injection using the same assessment as pre injection. It should be assessed again 4--6 months interval.
Spasticity
Symptomatic improvement decreases spasm frequency and relief of pain. There is a reduction of generalized spasticity – it facilitates sitting, and positioning or standing and also allows wearing of orthosis. In functional improvement it improves mobility in terms of speed, quality or endurance of gait, endurance of wheel chair propulsion, improves ease and safety of transfers, dexterity and reaching. There is decrease in burden on care givers such as positioning (e.g., feeding) care and hygiene, e.g., washing and catheterization, dressing, decreases care time to allow quality time. In prevention of complications, it prevents unnecessary use of antispasmodic and others medications, and also prevents pressure sores and contractures. It prevents or delays surgery. Cosmetically, it improves body image.
BoNT injection
BoNT should be offered as a treatment option to reduce muscle tone and improve passive function in adults with spasticity (Level A) and should be considered to improve function (Level B).[34] Patient should be selected for BoNT depending on the focal spasticity, dynamic spastic component, clearly identified goals for treatment and anticipated functional gains. Patient and their families/care givers should be given adequate information, prior to treatment and should agree goals before treatment is given. Informed consent should be obtained from patients prior to injection. If the patient does not have the mental capacity to concern current policies for obtaining consent should be followed. The maximum dose used in a single treatment should not exceed 1500 mu Dysport (Ipsen), 400 U Botox (Allergan) or 10,000 U Myobloc. The dose of BoNT injected intramuscularly depends on the muscle size. Small muscles such as the open cords receive 0.75 U, whereas larger neck muscles may require 100--150 U and lower limb muscles may require 200--300 U to exert a desirable effect.
Other services
BoNT injection must be a part of rehabilitation program involving postinjection exercise, muscle stretch and/splinting, to achieve an optimal beneficial clinical effect. Clinical should have access to facilities to aid in assessment, selection and treatment planning, e.g., electromyography (EMG). Clinical should familiarize themselves with a single agent to avoid confusion over dose.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Simpson LL. Identification of the major steps in Botulinum toxin action. Ann Rev Pharmacol Toxicol. 2004;44:167–93. doi: 10.1146/annurev.pharmtox.44.101802.121554. [DOI] [PubMed] [Google Scholar]
- 2.Girlanda P, Quartarone A, Sinicropi S, Nicolosi C, Messina C. Unilateral injection of botulinum toxin in blepharospam: Single fiber electromyography and blink reflex study. Mov Disord. 1996;11:27–31. doi: 10.1002/mds.870110107. [DOI] [PubMed] [Google Scholar]
- 3.Jankovic J, Orman J. Botulinum A toxin for cranial-cervical dystonia: A double-blind, placebo-controlled study. Neurology. 1987;37:616–23. doi: 10.1212/wnl.37.4.616. [DOI] [PubMed] [Google Scholar]
- 4.Nussgens Z, Roggenkamper P. Comparison of two Botulinum-toxin preparations in the treatment of essential blepharospasm. Gracfes Arch Clin Exp Ophthalmol. 1997;235:197–9. doi: 10.1007/BF00941758. [DOI] [PubMed] [Google Scholar]
- 5.Sampaio C, Ferreira JJ, Simões F, Rosas MJ, Magalhães M, Correia AP, et al. DYSBOT: A single-blind, randomized parallel study to determine w4hether any differences can be detected in the efficacay and tolerability of two formulations of botulinum toxin type A-Dysport and Botox - assuming a ratio of 4:1. Mov Disord. 1997;12:1013–8. doi: 10.1002/mds.870120627. [DOI] [PubMed] [Google Scholar]
- 6.Yoshimura DM, Aminoff MJ, Tami TA, Scott AB. Treatment of hemifacial spasm with Botulinum toxin. Muscle Nerve. 1992;15:1045–9. doi: 10.1002/mus.880150909. [DOI] [PubMed] [Google Scholar]
- 7.Ranoux D, Gury C, Fondarai J, Mas JL, Zuber M. Respective potencies of Botox and Dysport: A double blind, randomised, crossover study in cervical dystonia. J Neurol Neurosurg Psychiatry. 2002;72:459–62. doi: 10.1136/jnnp.72.4.459. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Garcia Ruiz PJ, Martínez Castrillo JC, Burguera JA, Campos V, Castro A, Cancho E, et al. Evolution of dose and response to botulinum toxin A in cervical dystonia: A multicenter study. J Neurol. 2011 Jan 1; doi: 10.1007/s00415-010-5880-1. [DOI] [PubMed] [Google Scholar]
- 9.Chapman MA, Barron R, Tanis DC, Gill CE, Charles PD. Comparison of botulinum neurotoxin preparations for the treatment of cervical dystonia. Clin Ther. 2007 Jul;29:1325–37. doi: 10.1016/j.clinthera.2007.07.020. [DOI] [PubMed] [Google Scholar]
- 10.Poewe W, Deuschl G, Nebe A, Feifel E, Wissel J, Benecke R, et al. What is the optimal dosse of botulinum toxin A in the treatment of cervical dystonia? Results of a double blind, placebo controlled, dose ranging study using Dysport. German Dystonia Study Group. J Neurol Neurosurg Psychiatry. 1998;64:13–7. doi: 10.1136/jnnp.64.1.13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Truong D, Duane DD, Jankovic J, Singer C, Seeberger LC, Comella CL, et al. Efficacy and safety of Botulinum type A toxin (Dysport) in cervical dystonia: Results of the first US randomized, double-blind, placebo-controlled study. Mov Disord. 2005;20:783–91. doi: 10.1002/mds.20403. [DOI] [PubMed] [Google Scholar]
- 12.Brashear A, Lew MF, Dykstra DD, Comella CL, Factor SA, Rodnitzky RL, et al. Safety and efficacy of NeuroBloc (Botulinum toxin type B) in type A-responsive cervical dystonia. Neurology. 1999;53:1439–46. doi: 10.1212/wnl.53.7.1439. [DOI] [PubMed] [Google Scholar]
- 13.Brin MF, Lew MF, Adler CH, Comella CL, Factor SA, Jankovic J, et al. Safety and efficacy of NeuroBloc (botulinum toxin type B) in type A-resistant cervical dystonia. Neurology. 1999;53:1431–8. doi: 10.1212/wnl.53.7.1431. [DOI] [PubMed] [Google Scholar]
- 14.Lew MF, Adornato BT, Duane DD, Dykstra DD, Factor SA, Massey JM, et al. Botulinum toxin type B: A double-blind, placebo-controlled, safety and efficacy study in cervical dystonia. Neurology. 1997;49:701–7. doi: 10.1212/wnl.49.3.701. [DOI] [PubMed] [Google Scholar]
- 15.Jankovic J, Schwartz K, Donovan DT. Botulinum toxin treatment of cranial-cervical dystonia, spasmodic dysphonia, other focal dystonias and hemifacial spasm. J Neurol Neurosurg Psychiatry. 1990;53:633–9. doi: 10.1136/jnnp.53.8.633. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Troung DD, Rontal M, Rolnick M, Aronson AE, Mistura K. Double-blind controlled study of Botulinum toxin in adductor spasmodic dysphonia. Laryngoscope. 1991;101:630–4. doi: 10.1288/00005537-199106000-00010. [DOI] [PubMed] [Google Scholar]
- 17.Murry T, Woodson GE. Combined-modality treatment of adductor spasmodic dysphonia with botulinum toxin and voice therapy. J Voice. 1995;9:460–5. doi: 10.1016/s0892-1997(05)80211-5. [DOI] [PubMed] [Google Scholar]
- 18.Wong DL, Adams SG, Irish JC, Durkin LC, Hunt EJ, Charlton MP. Effect of neuromuscular activity on the response to Botulinum toxin injections in apasmodic dysphonia. J Otolaryngol. 1995;24:209–16. [PubMed] [Google Scholar]
- 19.Warrick P, Dromey C, Irish JC, Durkin L, Pakiam A, Lang A. Botulinum toxin for essential tremor of the voice with multiple anatomical sites of tremor: A crossover design study of unilateral versus bilateral injection. Laryngoscope. 2000;110:1366–74. doi: 10.1097/00005537-200008000-00028. [DOI] [PubMed] [Google Scholar]
- 20.Adler CH, Bansberg SF, Hentz JG, Ramig LO, Buder EH, Witt K, et al. Botulinum toxin type A for treating voice tremor. Arch Neurol. 2004;61:1416–20. doi: 10.1001/archneur.61.9.1416. [DOI] [PubMed] [Google Scholar]
- 21.Blitzer A, Brin MF. The evaluation and management of abductor laryngeal dystonia. In: Jankovic J, Hallet M, editors. Therapy with Botulinum toxin. New York: Marcel Dekker, Inc; 1994. pp. 451–9. [Google Scholar]
- 22.Kruisdijk JJ, Koclman JH, Ongerboer de Visscr BW, de Haan RJ, Speelman JD. Botulinum toxin for writer's cramp: A randomized, placebo-controlled trial and 1-year follow-up. J Neurol Neurosurg Psychiatry. 2007;78:264–70. doi: 10.1136/jnnp.2005.083170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Yoshimura DM, Aminoff MJ, Olney RK. Botulinum toxin therapy for limb dystonias. Neurology. 1992;42:627–30. doi: 10.1212/wnl.42.3.627. [DOI] [PubMed] [Google Scholar]
- 24.Tsui JK, Bhatt M, Calne S, Calne DB. Botulinum toxin in the treatment of writer's cramp: A double-blind study. Neurology. 1993;43:183–5. doi: 10.1212/wnl.43.1_part_1.183. [DOI] [PubMed] [Google Scholar]
- 25.Cole R, Hallett M, Cohen LG. Double-blind trial of Botulinum toxin for treatment of focal hand dystonia. Mov Disord. 1995;10:466–71. doi: 10.1002/mds.870100411. [DOI] [PubMed] [Google Scholar]
- 26.Chen R, Karp BI, Goldstein SR, Bara-Jimenez W, Yaseen Z, Hallett M. Effect of muscle activity immediately after botulinum toxin injection for writer's cramp. Mov Disord. 1999;14:307–12. doi: 10.1002/1531-8257(199903)14:2<307::aid-mds1016>3.0.co;2-3. [DOI] [PubMed] [Google Scholar]
- 27.Geenen C, Consky E, Ashby P. Localizing muscles for botulinum toxin treatment of focal hand dystonia. Can J Neurol Sci. 1996;23:194–7. doi: 10.1017/s0317167100038506. [DOI] [PubMed] [Google Scholar]
- 28.Molloy FM, Shill HA, Kaelin-Lang A, Karp BI. Accuracy of muscle localization without EMG: Implications for treatment of limb dystonia. Neurology. 2002;58:805–7. doi: 10.1212/wnl.58.5.805. [DOI] [PubMed] [Google Scholar]
- 29.Marras C, Andrews D, Sime E, Lang AE. Botulinum toxin for simple motor tics: A randomized, double-blind, controlled clinical trial. Neurology. 2001;56:605–10. doi: 10.1212/wnl.56.5.605. [DOI] [PubMed] [Google Scholar]
- 30.Jankovic J, Schwartz K, Clemence W, Aswad A, Mordaunt J. A randomized, double-blind, placebo-conrolled study to evaluate Botulinum toxin type A in essential hand tremor. Mov Disord. 1996;11:250–6. doi: 10.1002/mds.870110306. [DOI] [PubMed] [Google Scholar]
- 31.Brin MF, Lyons KE, Doucette J, Adler CH, Caviness JN, Comella CL, et al. A randomized, double masked, controlled trial of botulinum toxin type A in esssential hand tremor. Neurology. 2001;56:1523–8. doi: 10.1212/wnl.56.11.1523. [DOI] [PubMed] [Google Scholar]
- 32.Pahwa R, Busenbark K, Swanson-Hyland EF, Dubinsky RM, Hubble JP, Gray C, et al. Botulinum toxin treatment of essential head tremor. Neurology. 1995;45:822–4. doi: 10.1212/wnl.45.4.822. [DOI] [PubMed] [Google Scholar]
- 33.Comella CL, Buchman AS, Tanner CM, Brown-Toms NC, Goetz CG. Botulinum toxin injection for spasmodic torticollis: Increased magnitude of benefit with electromyographic assistance. Neurology. 1992;42:878–82. doi: 10.1212/wnl.42.4.878. [DOI] [PubMed] [Google Scholar]
- 34.Simpson DM, Gracies JM, Graham HK, Miyasaki JM, Naumann M, Russman B, et al. Assessment: Botulinum neurotoxin for the treatment of spasticity (an evidence-based review).Report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology. 2008;70:1691–8. doi: 10.1212/01.wnl.0000311391.00944.c4. [DOI] [PubMed] [Google Scholar]