

Abstract
Posttraumatic stress disorder (PTSD) may produce internal “threats to the self,” which generate shame. Shame is theoretically and empirically linked to intimate partner violence (IPV) perpetration. We examined relations among PTSD, cognitive processing of shame-relevant information, and IPV perpetration. Forty-seven community participants completed an emotional Stroop task with shame-relevant and neutral words. Stimuli were presented supraliminally (i.e., until vocal response) and subliminally (i.e., below an individualized threshold of conscious awareness). Facilitated color-naming of shame-relevant words (thought to reflect congruence between shame and self-schemas) mediated the relation between PTSD severity and IPV perpetration frequency. Mediation results for subliminal stimuli suggest that biased processing of shame cues may occur preconsciously and potentially catalyze processes (i.e., expectations of rejection in ambiguous situations with one's partner; avoidance that minimizes discomfort and protects self-image) that lead to IPV perpetration. Psychotherapeutic approaches to PTSD and IPV should consider the role of facilitated processing of shame cues.
Keywords: PTSD, trauma, partner abuse, cognitive bias, cognition
PTSD is a chronic, disabling psychological disorder that results from exposure to trauma. The overall lifetime prevalence of PTSD in the United States is 6.8% (NCS-R; Kessler, Berglund, Demler, Jin, & Merikangas, 2005). Individuals suffering from PTSD encounter a variety of problems, including occupational and educational impairment (see Kessler, 2000). Researchers have recently focused on the “social ecology” of PTSD, or the interplay between PTSD symptoms and social phenomena in the development, maintenance, and consequences of PTSD (Charuvastra & Cloitre, 2008). For example, PTSD is associated with elevated risk of intimate partner violence (IPV) perpetration (e.g., Marshall, Panuzio, & Taft, 2005; Stuart, Moore, Gordon, Ramsey, & Kahler, 2006) and PTSD symptoms mediate the link between trauma severity and IPV perpetration (Taft, Vogt, Marshall, Panuzio, & Niles, 2007). Furthermore, longitudinal studies suggest a causal relationship in which PTSD symptomatology leads to IPV perpetration (e.g., Wolfe, Wekerle, Scott, Straatman, & Grasley, 2004). However, understanding of mechanisms underlying the relation between PTSD and IPV perpetration remains limited (Bell & Naugle, 2008).
We conceptualize the link between PTSD and IPV perpetration within the context of social information processing models, generally positing that individuals with PTSD exhibit overgeneralized negative appraisals of socially threatening information, which lead to aggressive behavior. This proposition is derived from models that link aggression in PTSD to hypervigilance to physical threat cues (e.g., Chemtob, Novaco, Hamada, Gross, & Smith, 1997), research demonstrating that the link between social rejection and aggression towards peers is mediated by social information processing deficits (Dodge et al., 2003), and research demonstrating pervasive deficits in social information processing among men who perpetrate IPV (see Holtzworth-Munroe, 2000). In the context of intimate relationships, individuals with PTSD may be apt to misperceive ambiguous partner behaviors as indicating probable social threat (e.g., rejection). Such misperceptions could increase hyperarousal, which impairs adaptive reappraisal of social cues and inhibits one's ability to control aggressive responses (Chemtob et al., 1997). Preliminary research suggests that later-stage deficits in social information processing (i.e., misattribution of partners' behavior to partners' negative intentions, decision-making in response to negative marital interactions) are important in the link between PTSD and male-perpetrated IPV (Taft, Schumm, Marshall, Panuzio, & Holtzworth-Munroe, 2008). Further examination of more specific social information processes in the relation between PTSD and IPV is warranted, particularly that focused on understanding early-stage information processing since earlier stage processes (e.g., perception, appraisal) influence later stages (McFall, 1982).
Ehlers and Clark (2000) posit that PTSD becomes persistent when individuals process trauma in a way that leads to a sense of current physical threat and/or “threats to the self” (i.e., threats to the view of oneself as a capable and acceptable person). In the context of trauma, “threats to the self” are theorized to generate shame (Dunmore, Clark, & Ehlers, 2001). Individuals with PTSD exhibit elevated levels of self-reported shame (Leskela, Dieperink, & Thuras, 2002) and post-trauma shame is associated with the maintenance of PTSD symptoms over time (Andrews, Brewin, Rose, & Kirk, 2000). Shame is characterized by evaluative threats to one's self-schema, which are theorized to increase one's propensity to perceive negative evaluation from others (Gilbert, Pehl, & Allan, 1994) and appraise ambiguous events as representing probable rejection (Claesson & Sohlberg, 2002). In the context of relationships, shame can result in maladaptive relationship behaviors, perhaps due to feelings of inadequacy to perform in a needed manner and a desire to hide the (assumed) incompetent self from others (Covert, Tangney, Maddux, & Heleno, 2003). In fact, self-reported shame is associated with IPV perpetration (Dutton, van Ginkel, & Starzomski, 1995). Guilt is also a prominent feature of PTSD (Kubany, 1994) and correlates highly with shame (Tangney & Dearing, 2002), but is not thought to result from “threats to the self” (i.e., guilt is characterized by negative evaluation of a specific behavior, rather than the self, and does not include the expectation of negative evaluation; Lewis, 1971) and is negatively correlated with aggression (Tangney & Dearing, 2002). The current study therefore focuses on shame-related processes.
Individuals with PTSD may be especially prone to using maladaptive strategies to control shame-relevant cognitions (e.g., avoidance; Foa, Riggs, & Gershuny, 1995), which can occur automatically and with little awareness (Dunmore et al., 2001). Under conditions in which individuals “bypass” (i.e., avoid, deny, or fail to acknowledge) shame and its associated cognitions, shame is theorized to lead to the deflection of self-blame and hostility toward the source of expected rejection in order to protect one's self-image and prevent further vulnerability (Lewis, 1971). In fact, shame is associated with externalization of blame (an avoidant response), which is associated with aggressive behavior (Stuewig, Tangney, Heigel, Harty, & McCloskey, 2010). Despite exclusive use of self-report measures, this work highlights the important role of “bypassed” shame in the prediction of aggressive behavior.
Because “bypassed” shame is, by definition, avoided or unacknowledged, implicit measurement of shame-related processes may be most valid. Psychopathology-related processes can be triggered by information that is too weak to produce verbal recognition and report (Nisbett & Wilson, 1977), and self-report scales, which are also prone to the influence of social desirability, place heavy demands on respondents' ability to identify painful cognitions (Kugler & Jones, 1992). Further, behavioral responses to shame can occur preemptively and without individuals' recognition that anticipation of shame influenced their behaviors (Schoeleber & Berenbaum, 2010). Thus, implicit measures, which indicate activation of associations stored in memory without reflecting the individual's belief in the strength of the associations, may be especially useful for measuring undesirable cognitions (Gawronski & Bodenhausen, 2006).
The emotional variant of the Stroop (1935) task is the most frequently used paradigm for investigating psychopathology-related cognitive processing biases without relying on self-report (Williams, Mathews, & MacLeod, 1996). Participants name the ink color of emotionally significant and neutral words, and color-naming reaction times are expected to differ as a function of words' emotional salience. Following the premise that emotional content interferes with the color-naming task (see Williams et al., 1996), many researchers have found longer color-naming latencies for emotional, compared to neutral, words; however, others have found facilitated color-naming of emotional words (e.g., Kyrios & Iob, 1998; McNally et al., 1994).
We expect PTSD and IPV perpetration severity to be associated with shorter Stroop color-naming latencies for shame relevant than neutral words (i.e., facilitated processing). Theories of self-schema processing (e.g., Markus, 1977) suggest that schema-congruent content is prioritized in the competition for cognitive processing resources. Because trauma-exposed individuals' self-schemas are often characterized by shame (Dutra, Callahan, Forman, Mendelsohn, & Herman, 2008) and the Stroop task is proposed to measure efficiency of processing compatible (versus incompatible) information (MacLeod & MacDonald, 2000), shame-relevant (i.e., schema-compatible) information should be processed especially rapidly in PTSD. In addition, associative networks including previous shame experiences may make shame representations readily accessible by subtle cues (Dalgleish, 1994). Furthermore, because facilitated processing has been conceptualized as cognitive avoidance of the semantic content in order to avoid becoming overwhelmed by intrusive thoughts related to it (Constans, McCloskey, Vasterling, Bailey, & Mathews, 2004; Kyrios & Iob, 1998), an individual who experiences covert (“bypassed”) shame may process shame-relevant stimuli in a facilitated manner. Because avoidance is a primary maintenance factor in PTSD and avoidance (or “bypassing”) of shame-related cognitions is thought to serve as a means for coping with shame (Elison, Pulos, & Lennon, 2006), this effect may be especially prominent among individuals with more severe PTSD. Such processing could accelerate negative appraisals of ambiguous social situations and serve as an initial step in a cascade of processes that contribute to IPV perpetration.
In the current study, we hypothesized that: (a) PTSD severity would be positively associated with frequency of IPV perpetration; (b) PTSD severity would be negatively associated with shame processing speed (i.e., color-naming reaction time differences between shame and neutral words on the emotional Stroop task); (c) shame processing speed would be negatively associated with IPV perpetration frequency; and (d) shame processing speed would mediate the association between PTSD severity and IPV perpetration frequency. Although most studies of PTSD have focused on processing of consciously perceived (i.e., supraliminal) stimuli (Buckley, Blanchard, & Neill, 2000), facilitated processing of shame-relevant material may be most sensitively measured using subliminally presented words. Thus, we primarily expected to observe these relations for the subliminal presentation condition, but relations were expected to hold for the supraliminal condition because automatic processing is thought to contribute to responses on these trials. Women were included in the current sample because of the high prevalence of PTSD among women (Olff, Langeland, Draijer, & Gersons, 2007) and research demonstrating that women perpetrate IPV at rates greater than or equal to men (Archer, 2000), which is not attributable solely to self-defense (DeKeseredy & Schwartz, 1998). Furthermore, predictors of IPV perpetration do not differ as a function of gender (Carney, Buttell, & Dutton, 2007), both men and women experience posttraumatic shame (Andrews et al., 2000), and threats to self-schemas are associated with shame across genders (Ferguson, Eyre, & Ashbaker, 2000). Therefore, gender differences in the overall models were not expected.
1. Method
1.1. Participants and Procedures
Community participants were recruited for a larger study of PTSD and relationship functioning using newspaper and internet advertisements (71%), and postcards and/or flyers placed in local businesses (22%) and a local outpatient mental health clinic (7%). Recruitment materials indicated that heterosexual couples in which at least one partner experienced a stressful life event should contact the laboratory for a study of stressful life events and relationships.
Couples were screened over the telephone for probable PTSD in either partner using the PTSD Checklist, Civilian Version (PCL-C; Weathers, Litz, Herman, Huska, & Keane, 1993). Each recruited couple included at least one partner who met screening criteria for PTSD (i.e., PCL-C cut-score of 44; Blanchard, Jones-Alexander, Buckley, & Forneris, 1996). A total of 276 couples contacted the lab about the study. Among 192 couples, both partners were interested in the study and completed the screening. Couples were deemed ineligible if neither partner met the PCL-C cut-score (n = 122 couples), partners' combined income exceeded $100,000 per year and/or either partner had more than six years post-high school education (n = 3), they could not be contacted for scheduling (n = 2), or they ended their relationship prior to completing the study (n = 1). Income and education restrictions were included in order to exclude university faculty and affiliated families, thus maintaining a sample representative of individuals typically served by community clinics and those residing in surrounding rural communities. As such, few fulltime students (n = 6) and no university faculty were included in the current sample.
Sixty-four couples were included in the larger study. For the current report, only partners with the greater PTSD severity based on responses to the Clinician Administered PTSD Scale (CAPS; Blake, Weathers, Nagy, & Kaloupek, 1995) were included in the analyses; therefore, the sample is composed of individuals who were currently in a relationship and whose PTSD symptoms were more severe relative to their partner's. This method effectively avoids dependency of partners within couples (i.e., ensures random sampling of individuals from the population). In addition, because not all participants who screened into the study met diagnostic criteria for PTSD upon clinical interview, this method yields a normal distribution of PTSD severity scores that is not contaminated by low PTSD severity scores of partners who did not screen into the study. Of the 64 individuals with higher PTSD severity scores compared to their partners, 16 did not complete the Stroop task due to a programming error that was not discovered until after data collection began (n = 10), computer software and server malfunctions (n = 5), and incorrect instruction provided to the participant (n = 1). Furthermore, one participant's data was not included because more than 20% of her trials were deemed to be outliers.
The final sample consisted of 47 individuals (36 female) with a mean age of 37.93 (SD= 12.75) years. Participants self-identified as Caucasian (84.8%), biracial/multiracial (6.5%), Hispanic/Latino (4.3%), or African-American (4.3%). Participants' mean relationship length was 13.72 (SD = 13.20) years and participants had an average of 0.98 (SD = 1.21) children together. Participants had an average individual income of $1,299.00 (SD= $1,190.00) per month, an average of 14 (SD = 2.07) years of education, 63.4% were currently employed, and approximately 62% of these participants were recruited from relatively rural areas.
As part of the larger study, participants completed the current study procedures during the beginning of one eight-hour laboratory session or during the first of two four-hour sessions. Men and women completed study procedures in different orders because tasks could not be completed simultaneously due to equipment and personnel restrictions. Men completed study procedures (see below) in the following order: questionnaires and PTSD diagnostic interview (administered consecutively), pretest to establish threshold for subliminal trials (90 minutes after the interview), and emotional Stroop and self-referential encoding tasks (administered consecutively 42 minutes after the pretest). Women completed study procedures in the following order: pretest to establish threshold for subliminal trials, emotional Stroop and self-referential encoding tasks (administered consecutively 16 minutes after the pretest), questionnaires (40 minutes after completion of the self-referential encoding task), and PTSD diagnostic interview (60 minutes after completion of questionnaires).
1.2. Apparatus and Materials
1.2.1. PTSD diagnosis
Current PTSD symptoms were confirmed using the Clinician Administered PTSD Scale (CAPS; Blake et al., 1995). The CAPS, a structured interview that assesses the frequency and intensity of each symptom using standard prompt questions and explicit, behaviorally-anchored rating scales, is commonly considered the gold standard in PTSD assessment. The CAPS has demonstrated high interrater reliability (r = .92 - .99), high internal consistency (r = .73 - .85), and high convergent validity with other PTSD measures (Weathers, Keane, & Davidson, 2001). In the current sample, coefficient alpha was .89.
1.2.2. Traumatic events
The Traumatic Life Events Questionnaire (TLEQ; Kubany et al., 2000) was used to assist in the determination of the primary trauma to be assessed during the CAPS. The TLEQ lists 22 types of potentially traumatic events and asks respondents to indicate if they experienced each event, and if so, how many times. The TLEQ also includes queries about fear, helplessness, horror, and which trauma currently causes the most distress. The TLEQ has demonstrated adequate levels of test-retest reliability and good content validity (Kubany et al., 2000).
1.2.3. Intimate partner violence
The 12-item Revised Conflict Tactics Scale (CTS2; Straus, Hamby, Boney-McCoy, & Sugarman, 1996) physical assault subscale, which includes moderate (e.g., “I pushed or shoved my partner”) and severe (e.g., “I kicked my partner”) physical aggression items, was used as a measure of intimate partner violence (IPV). The CTS2 physical assault subscale has good internal consistency and test-retest reliability (Straus et al., 1996; Vega & O'Leary, 2007), as well as convergent validity across a wide range of measures (Schumacher, Feldbau-Kohn, Slep, & Heyman, 2001). Participants indicated how many times during the past year (ranging from “never” to “more than 20 times”) they and their partners engaged in each behavior. Each behavior was assigned a severity weight based on risk of physical injury (Straus & Gelles, 1990), then weighted frequency scores were summed. Because partner agreement on measures of IPV perpetration is often low, and social desirability may lead to underreporting of aggression, we used the higher total weighted IPV perpetration score (either male or female report) within each couple. In the current sample, the internal consistency reliability coefficient was .76. Due to positive skew, a logarithm transformation was used to normalize the distribution.
1.2.4. Test for colorblindness
Three widely used Ishihara (1939) color-blindness schemes were administered to ensure that participants could accurately identify the four colors in the emotional Stroop task.
1.2.5. Subliminal threshold pretest
Participants completed a lexical decision task to establish individualized stimulus thresholds as a means of ensuring that participants were not consciously aware of the word content on subliminal trials (Merikle & Reingold, 1990). Participants pressed one of two response buttons to indicate whether a word (e.g., “apple”) or a nonword (e.g., “fump”) was present in each of 240 trials. An adaptive staircase procedure including six stimulus presentation durations (ranging from 13ms to 169ms) was used to determine how long the stimulus word should be presented before replacement with a pattern mask for participants to identify stimuli at chance level. Pattern masks were randomly generated patterns composed of overlapping uppercase letters that preserve few of the letters' visual features necessary to identify stimuli at chance level (Breitmeyer & Ogmen, 2006). A 60ms threshold, based on the refresh rate of the computer monitor and previous studies of subliminal processing in PTSD (Buckley et al., 2000), was assigned to participants whose lexical decision accuracy across the range of presentation times did not rise above chance level (n = 4).
1.2.6. Emotional Stroop stimuli
Emotional Stroop task stimuli included six categories of words (i.e., neutral, shame, guilt, non-interpersonal negative, non-interpersonal positive, physical threat). Only responses to shame and neutral words were examined in the current study. Positive words were included to prevent development of negative response sets and habituation to negatively valenced words.
Shame words were taken from literature on posttraumatic shame and generated by the authors and lab research assistants. Words were subjected to two stages of ratings in which five clinical psychology graduate students rated each word for its relevance to each category on a scale from 0 (“does not represent the indicated category”) to 10 (“represents the indicated category perfectly”). The first rating included 300 words, of which approximately 50 were broadly considered shame-relevant. Raters were then provided empirically-informed definitions of each category when rating a reduced list of 200 words more specific to one category according to the first round of ratings. Highly rated shame-relevant words for which there are no lexical norms in the English Lexicon Project (ELP; Balota et al., 2007) were discarded. The final twelve words for the shame category were chosen according to an algorithm meant to balance mean rating within the shame category (M = 5.43), meaningful differences in ratings across categories (mean difference between shame and other categories = 4.3), and overall length and abstractness. Nine of the twelve shame words were appropriate for K-6th grade (Paynter, Bodrova, & Doty, 2005). For the three words that had no published grade equivalence, word length was used as a proxy for abstractness/difficulty (Chall & Dale, 1995). Though ratings of appropriateness to the shame category were not uniformly high across final words, likely due to conceptual overlap with related constructs with which shame is highly correlated (e.g., guilt), a confirmatory factor analysis conducted with Mplus statistical software (Muthén & Muthén, 2006) revealed that these words represent a unitary factor. The model fit was within appropriate limits, χ2 = 67.53, df = 54, ns; SRMR = 0.05, RMSEA = 0.08, CFI = 0.97, TLI = 0.96 (Hu & Bentler, 1999). Factor loadings ranged from .54 to .88. Shame words were belittle, contempt, exposed, hide, humiliated, incompetent, insult, mock, pathetic, reject, scorn, and shame.
To reduce likelihood of inflated reaction times to emotion words, which are typically longer and have lower frequency of use than neutral words (Larsen, Mercer, & Balota, 2006), word length, frequency, and orthographic neighborhood information was obtained for shame words through the ELP (Balota et al., 2007). The ELP then generated neutral words with matching lexical characteristics. Neutral words were brands, caller, closet, dental, fixing, laying, plates, puzzle, raises, rental, sticks, and trucks.
1.2.7. Emotional Stroop task
The task started with a black screen and a white fixation point. Participants were asked to name the color of each stimulus presented centrally against a black background in capitalized 24-point bold Arial font by speaking into the microphone as quickly as possible. Words were randomly paired with four text colors (i.e., blue, green, red, and yellow), each used in 25% of the trials. In the supraliminal condition, word stimuli were displayed until vocal response. In the subliminal condition, each trial included a backward masking procedure in which a pattern mask of the same color as the stimulus word followed the word at a stimulus onset asynchrony equal to the duration established in the pretest. The mask remained displayed until vocal response. Words were presented in a fully randomized manner, and the supraliminal and subliminal presentation trials were randomly intermixed. Each of the 72 word stimuli (including 12 shame-relevant and 12 neutral words) was presented twice in both conditions for a total of 288 trials (96 trials included in the current study). The fixed inter-trial interval was 500ms. Vocal responses were recorded with a voice-activated dynamic microphone that was connected to the computer via a response box (PST Serial Response Box, Psychology Software Tools, Pittsburgh, PA). E-Prime software calculated the delay between the onset of the stimulus word and the detection of the participant's verbal response.
1.2.8. Self-referential encoding task
To confirm that shame-relevant stimuli reflected participants' self-schemas, participants indicated whether each word described him or her by pressing the appropriate key (i.e., “yes” or “no”). The task began with a fixation point presented for 500ms on a computer screen. Each trial consisted of the prompt “Describes me?” presented for 500ms, followed by a 250ms pause, presentation of a word from the Stroop task in capitalized letters, and removal of the word from the screen after the participant's response. The inter-trial interval was 1000ms.
1.3. Data Analysis
Continuous PTSD severity scores were used for the analyses because they improve statistical power, are more stable over time, display higher levels of reliability and validity, and yield a greater amount of clinically relevant information than categorical measures of psychopathology (Cohen, 1992; Watson, 2005; Widiger & Clark, 2000). Furthermore, taxometric analyses suggest that PTSD is a dimensional, rather than a categorical, disorder and PTSD may be more accurately conceptualized as an extreme reaction to traumatic life events rather than as a discrete clinical syndrome (e.g., Broman-Fulks et al., 2006).
Responses to 75 (1.7%) Stroop trials that were not made between 100ms and 4s after word presentation were discarded. Shame processing speed was calculated by subtracting the mean reaction time for neutral words from the mean reaction time for shame words. Negative processing speed scores reflect faster color-naming of shame words than neutral words. Positive processing speed scores reflect slower color naming of shame words than neutral words. Separate processing speed scores were calculated for subliminal and supraliminal conditions.
Because of the strength of the directional hypotheses (Jones, 1952) and well-cited criticisms of null hypothesis testing (e.g., Cohen, 1994), particularly within small samples in which power is limited, one-tailed tests were used to maximize power to detect small effects (Cohen, 1992). In addition to bivariate correlations, mediation models using Preacher and Hayes' (2004) bootstrapping methods were examined. These procedures provide greater statistical power for detecting effects and avoiding both Type I and II errors, compared to more traditional methods. Possible gender differences were explored by investigating gender as a simultaneous moderator of both paths in both mediation models. This method offers the greatest power to detect conditional indirect effects (Preacher, Rucker, & Hayes, 2007).
2. Results
2.1. Descriptive Statistics
Descriptive statistics are displayed in Table 1. CAPS severity scores ranged from 13 to 102, indicating that some participants were experiencing only mild symptoms of PTSD. Most participants reported moderate to severe PTSD symptoms (M = 53.26, SD = 20.03) and 28 participants (60% of the sample) met full DSM-IV diagnostic criteria for PTSD using the 1/2 frequency/intensity rule (Weathers, Ruscio, & Keane, 1999). Participants engaged in an average non-severity-weighted frequency of 4.38 acts of IPV in the past year (SD = 13.77; range = 0 -75), while the 17 participants (36% of the sample) who engaged in IPV perpetrated an average of 12.12 acts of IPV (SD = 21.11). The mean threshold for participants who successfully completed the pretest was 56.37ms (SD = 22.58), which was similar to the threshold assigned to individuals for whom performance accuracy did not rise above chance (i.e., 60ms). Despite sex differences in task order, there was no sex difference in individualized thresholds, t (41) = 1.08, p = .29.
Table 1. Descriptive Statistics and Intercorrelations Among Study Variables.
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|
| 1. PTSD symptom severity | -- | |||||||
| 2. Reexperiencing symptoms | .76*** | -- | ||||||
| 3. Avoidance symptoms | .91*** | .54*** | -- | |||||
| 4. Hyperarousal symptoms | .79*** | .37** | .61*** | -- | ||||
| 5. IPV perpetration | .37** | .23 | .39** | .26* | -- | |||
| 6. Subliminal presentation shame processing speed | -.35** | -.13 | -.39** | -.31* | -.36* | -- | ||
| 7. Supraliminal presentation shame processing speed | -.29* | -.21 | -.27* | -.22 | -.12 | .23 | -- | |
| 8. Number of self-descriptive shame words | .53*** | .41** | .51*** | .36** | .31* | -.42** | -.33* | -- |
| M | 53.26 | 15.23 | 21.09 | 16.94 | 6.28 | -8.93 | 15.94 | 3.19 |
| SD | 20.03 | 7.17 | 10.06 | 6.95 | 19.62 | 73.63 | 69.01 | 3.03 |
| Range | 13-102 | 1-31 | 3-41 | 2-32 | 0-103 | -254-138 | -207-176 | 0-10 |
Notes.
IPV = intimate partner violence (severity-weighted frequency scores);
p < .05,
p < .01,
p < .001,
all one-tailed
2.2. Associations Between Study Variables
Bivariate correlations are displayed in Table 1. As predicted, PTSD severity and IPV perpetration frequency exhibited a medium-sized positive relationship. PTSD severity and shame processing speeds in the subliminal and supraliminal conditions exhibited negative relationships of medium magnitude. Interestingly, PTSD avoidance symptoms were most strongly and consistently associated with shame processing speeds. IPV frequency and shame processing speed in the subliminal trial condition exhibited a medium-sized negative relationship, while the relationship between processing speed in the supraliminal trial condition and IPV frequency was statistically nonsignificant. Effect sizes of the positive relationships between the number of shame-relevant words labeled as self-descriptive and PTSD symptoms and IPV perpetration were large and medium, respectively. Finally, negative relationships between the number of shame-relevant words endorsed as self-descriptive and shame processing speeds in the subliminal and supraliminal conditions were of medium-to-large and medium magnitude, respectively, indicating that the more shame-relevant words endorsed as self-descriptive, the faster these words were color-named in relation to neutral words.
2.3.Mediation Analyses
As displayed in Figure 1, the direct effect of PTSD severity on shame processing speed in the subliminal condition was statistically significant (β = -.35, p < .05), the direct effect of shame processing speed in the subliminal condition on IPV perpetration frequency was statistically significant (β = -.36, p < .05), and the direct effect of PTSD severity on IPV perpetration was statistically significant (β = .37, p < .05). In addition, the effect of PTSD severity on IPV perpetration was reduced to nonsignificance when accounting for the effect of shame processing speed in the subliminal condition (β = .29, ns). Results of the bootstrap analysis indicate that mediation was present (M = .0058, SE = .0054; 95% CI = .0048 - .0165).
Figure 1.
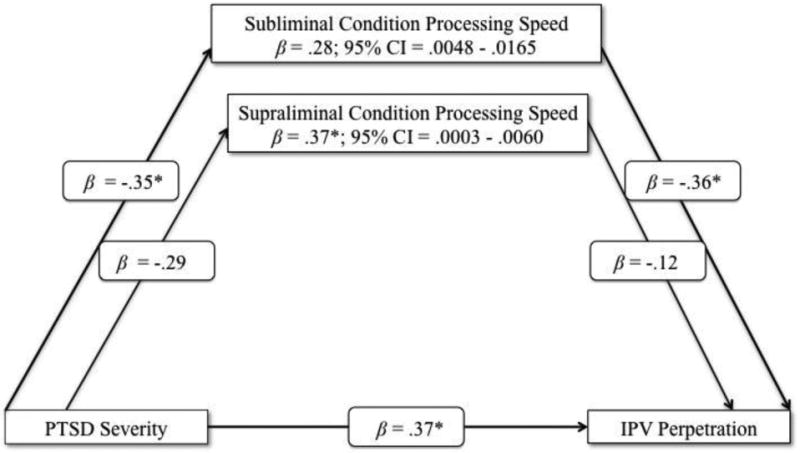
Mediating effect of shame processing speed on the relation between PTSD severity and IPV perpetration frequency. IPV = intimate partner violence; β = standardized beta; CI = confidence interval. *p < .05, **p < .01, all one-tailed.
The direct effect of PTSD symptom severity on shame processing speed in the supraliminal condition was statistically significant (β = -.29, p < .05), but the direct effect of shame processing speed in the supraliminal condition on IPV perpetration was not statistically significant (β = -.12, p = .21). The effect of PTSD symptom severity on IPV perpetration frequency was reduced when accounting for the effect of shame processing speed in the supraliminal condition (β= .37, p < .05). Results of the bootstrap analysis indicate that partial mediation was present (M = .0004, SE = .0033; 95% CI = .0003 - .0060).1
Neither of the models were moderated by gender, as the interactions between PTSD severity and gender were nonsignificant (subliminal: t = .23, ns; supraliminal: t = .15, ns) and the interactions between shame processing speed and gender were nonsignificant (subliminal: t = 1.09, ns; supraliminal: t = .58, ns).
3. Discussion
The current study was a preliminary investigation of the relations among PTSD symptom severity, cognitive processing of shame-relevant stimuli, and IPV perpetration frequency. We proposed that PTSD severity would be associated with facilitated processing of shame-relevant stimuli, which would theoretically lead to expectations of negative evaluation and rejection in ambiguous situations with one's partner. In turn, maladaptive avoidance strategies used to minimize discomfort elicited by these expectations would theoretically lead to intimate partner violence perpetration. Participants with PTSD symptoms of a wide range of severity were presented with subliminal and supraliminal shame-relevant stimuli in an emotional Stroop task and assessed for IPV perpetrated during the past year. Participants with more severe PTSD symptoms exhibited facilitated color-naming of subliminally presented shame-relevant words, which mediated the positive relation between PTSD severity and frequency of IPV perpetration. This model also held for the supraliminal presentation condition, though, as expected, results were less robust. These results suggest that PTSD-related cognitive processing of shame cues, particularly implicit shame cues, may facilitate aggressive behavior against intimate partners.
These findings broadly support a developing research literature based on the premise that PTSD may be associated with hypervigilance to threats to interpersonal relationships (see Bell & Orcutt, 2009) and extend the literature addressing the influence of social information processing on the link between PTSD and IPV. In fact, these findings suggest that Taft and colleagues' (2008) findings as to later-stage social information processes may have been partly a function of earlier stage processes. Facilitated detection and processing of shame-relevant stimuli may serve as early-stage warnings of impending negative affect, negative evaluation, and/or social rejection, to which individuals with elevated PTSD symptoms may respond with maladaptive coping strategies. This interpretation can be understood from the perspectives of shame theorists and researchers, who are generally consistent in their proposition that redirection of blame and hostility toward the individual viewed as disapproving and rejecting serves to defend one's self-schema against feelings of powerlessness (e.g., Lewis, 1971; Covert et al., 2003). As such, the results also broadly support Ehlers and Clark's (2000) assertion that PTSD is associated with internal “threats to the self,” which include shame-related cognitions.
Current findings highlight value of considering specific PTSD symptom clusters in relation to IPV perpetration. Relations among severity of avoidance symptoms, facilitated processing of subliminal shame stimuli, and frequency of IPV perpetration were most robust, which broadly supports Lewis' (1971) proposition that “bypassed,” or avoided, shame is especially likely to lead to aggression. However, more direct investigation of preattentive avoidance of shame cues in relation to IPV perpetration is warranted. The relations among hyperarousal symptoms, facilitated processing of shame stimuli, and frequency of IPV perpetration are also notable and consistent with Chemtob and colleagues' model of PTSD-related general aggression, suggesting that this model may also be applicable to IPV. Because contact with one's intimate partner uniquely mitigates responses to threat (Coan, Schaefer, & Davidson, 2006), individuals with elevated PTSD symptoms may depend on their intimate partners, more so than others, to alleviate distress. Thus, potential threats to intimate relationships may be particularly likely to elicit defensive, self-protective processes.
Although the current study results are preliminary, methodological considerations strengthen our confidence that findings were due to self-schema consistency of the shame-relevant stimuli rather than design artifacts that went unaddressed in many prior emotional Stroop studies (e.g., lack of consideration of lexical characteristics or direct testing of if Stroop stimuli represent participants' self-schemas). Our careful consideration of presentation durations for subliminal stimuli trials was a stronger test of preconscious (i.e., automatic, early-stage) processing than has been present in most previous studies. Furthermore, this study's novel method for investigating processing of shame-relevant information sets it apart from studies with PTSD populations that included only self-report measures (e.g., Leskela et al., 2002) and brief open-ended questions (Andrews et al., 2000) regarding the experience of shame.
The current study replicated the PTSD-IPV relation that has previously been found in a mixed-gender community sample (Christopher, Pflieger, Canary, Guerrero, & Holtzworth-Munroe, 2008), among women arrested for IPV (Stuart et al., 2006), community and clinical samples of men (Taft et al., 2007, 2008), and male veterans (Marshall et al., 2005). Unlike other studies, a substantial proportion of participants were recruited from relatively rural communities, adding to the generalizability of the observed PTSD-IPV relation and the sparse literature on the needs of rural populations. The current sample was composed of approximately 75% women, which is representative of the PTSD sex ratio in the general population (Olff et al., 2007), and the processes examined in the current study did not differ as a function of gender, further extending generalizability of the findings. Furthermore, this is the first study to link PTSD and IPV perpetration in a mixed-gender community sample using the CAPS, rather than brief self-report inventories (Christopher et al., 2008; Taft et al., 2008). Such scales are typically intended to be used as screening instruments and do not demonstrate better positive predictive power than measures of general distress (Shalev, Freedman, Peri, Brandes, & Sahar, 1997). Thus, current results offer stronger evidence that PTSD symptoms, beyond general distress, are related to IPV perpetration in community samples.
It is important to note that support for a mediation model based on cross-sectional data does not allow for causal conclusions and the directionality of the model could function differently than hypothesized (Preacher & Hayes, 2004). For example, it is likely that IPV perpetration maintains PTSD via decreased social support (Ozer, Best, Lipsey, & Weiss, 2003). Regardless of directionality, however, it is important to first recognize that processing of shame cues plays a role in the PTSD-IPV relationship. Future research should include examination of directionality and mechanistic assumptions with experimental and longitudinal designs.
We did not measure the emotional experience of shame because of the strong theoretical rationale for measuring early-stage processing of shame cues in relation to PTSD and IPV. Therefore, these results cannot speak to whether one variable (cognitive processing of shame-relevant stimuli) is more important to the PTSD-IPV relation than the other (emotional experience of shame). It may be warranted that researchers replicating this work make attempts to decompose the construct of “shame” into these related, but theoretically independent, components to clarify which components account for the present findings. We also did not measure internal “threats to the self,” despite drawing upon Ehlers and Clark's (2000) cognitive model of PTSD, which is necessary to provide a direct test of their model. Finally, it is important to note that the relation between facilitated processing of shame-relevant stimuli and IPV may not be specific to PTSD, and may be present in individuals who exhibit psychological difficulties that are highly correlated with PTSD, such as those with elevated symptoms of depression or borderline personality disorder. Similarly, there are many other predictors of IPV perpetration in addition to PTSD, including conditions that frequently co-occur with PTSD, such as substance use and depression (e.g., Lipsky, Caetano, Field, & Bazargan, 2005); future studies may elucidate whether shame processing bias operates within those contexts to confer risk for IPV.
Treatments that modify PTSD patients' shame-oriented appraisals of themselves and their coping (e.g., cognitive processing therapy; Resick & Schnicke, 1993) may reduce preconscious processing of shame cues, increase self-control, and reduce externalization of blame (Claesson & Sohlberg, 2002). According to our theoretical model, reducing facilitated processing of shame cues in the context of PTSD should decrease IPV perpetration, which could improve relationship satisfaction and social support and reciprocally reduce PTSD symptoms (Ozer et al., 2003).
Consideration of biased processing of shame cues could also be incorporated into interventions for IPV, which have shown only minimal influence on recidivism (Babcock, Green, & Robie, 2004). These programs have been criticized for their limited consideration of proximal factors related to IPV (e.g., Whitaker et al., 2006). Current findings suggest that clinical consideration of both distal (i.e., PTSD symptoms) and proximal (i.e., biased processing of shame cues) factors in IPV perpetration is warranted in treatments for IPV.
In summary, findings from this first study of cognitive bias toward shame-relevant stimuli in PTSD highlight the importance of processing of shame cues in the PTSD-IPV relationship, in addition to suggesting that individual differences in the processing of shame cues can be empirically measured, can occur without conscious awareness, and may indicate a very rapid form of cognitive detection and avoidance that facilitates aggressive behavior. Processing of shame cues should thus be targeted for further investigation and possible clinical intervention.
Research Highlights.
First to examine cognitive processing of shame cues in the context of PTSD and IPV.
Extends findings of a link between PTSD and IPV to a mixed-gender community sample.
Link mediated by facilitated processing of shame cues in an emotional Stroop task.
Mediation effect was especially robust for subliminal processing of shame cues.
Results support the integration of theory and findings across diverse literatures.
Acknowledgments
Dr. Marshall is supported by the National Institutes of Health's Building Interdisciplinary Research Careers in Women's Health (BIRCWH) program (1 K12 HD055882). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
We thank Fiona Barwick, Kaitlyn Hanley, Kelly Parker-Maloney, Lauren Szkodny, and numerous undergraduate research assistants for their helpful contributions to participant recruitment and data collection.
Footnotes
When expectation-maximization estimation was used to impute missing data for 17 participants, the pattern of results remained the same.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributor Information
Lauren M. Sippel, Email: lms455@psu.edu.
Amy D. Marshall, Email: AmyMarshall@psu.edu.
References
- Andrews B, Brewin CR, Rose S, Kirk M. Predicting PTSD symptoms in victims of violent crime: The role of shame, anger, and childhood abuse. Journal of Abnormal Psychology. 2000;109:69–73. doi: 10.1037//0021-843x.109.1.69. [DOI] [PubMed] [Google Scholar]
- Archer JA. Sex differences in aggression between heterosexual partners: A meta-analytic review. Psychological Bulletin. 2000;126:651–680. doi: 10.1037/0033-2909.126.5.651. [DOI] [PubMed] [Google Scholar]
- Babcock JC, Green CE, Robie C. Does batterers' treatment work? A meta-analytic review of domestic violence treatment. Clinical Psychology Review. 2004;23:1023–1053. doi: 10.1016/j.cpr.2002.07.001. [DOI] [PubMed] [Google Scholar]
- Balota DA, Yap MJ, Cortese MJ, Hutchison KA, Kessler B, Loftis B, et al. Treiman R. The English Lexicon Project. Behavior Research Methods. 2007;39:445–459. doi: 10.3758/bf03193014. [DOI] [PubMed] [Google Scholar]
- Bell KM, Naugle AE. Intimate partner violence theoretical considerations: Moving towards a contextual framework. Clinical Psychology Review. 2008;28:1096–1107. doi: 10.1016/j.cpr.2008.03.003. [DOI] [PubMed] [Google Scholar]
- Bell KM, Orcutt HK. Posttraumatic stress disorder and male-perpetrated intimate partner violence. Journal of the American Medical Association. 2009;302:562–564. doi: 10.1001/jama.2009.1126. [DOI] [PubMed] [Google Scholar]
- Blake DD, Weathers FW, Nagy LM, Kaloupek DG. The development of a Clinician-Administered PTSD Scale. Journal of Traumatic Stress. 1995;8:75–90. doi: 10.1007/BF02105408. [DOI] [PubMed] [Google Scholar]
- Blanchard EB, Jones-Alexander J, Buckley TC, Forneris CA. Psychometric properties of the PTSD Checklist (PCL) Behaviour Research and Therapy. 1996;34:669–673. doi: 10.1016/0005-7967(96)00033-2. [DOI] [PubMed] [Google Scholar]
- Breitmeyer BO, Ogmen H. Visual masking: Time slices through conscious and unconscious vision. Oxford: Oxford University Press; 2006. [Google Scholar]
- Broman-Fulks JJ, Ruggiero KJ, Green BA, Kilpatrick DG, Danielson CK, Resnick HS, Saunders BE. Taxometric investigation of PTSD: Data from two nationally representative samples. Behavior Therapy. 2006;37:364–380. doi: 10.1016/j.beth.2006.02.006. [DOI] [PubMed] [Google Scholar]
- Buckley TC, Blanchard EB, Neill WT. Information processing and PTSD: A review of the empirical literature. Clinical Psychology Review. 2000;20:1041–1065. doi: 10.1016/s0272-7358(99)00030-6. [DOI] [PubMed] [Google Scholar]
- Carney MM, Buttell F, Dutton DG. Women who perpetrate intimate violence: A review of the literature with recommendations for treatment. Aggression and Violent Behavior. 2007;12:108–115. [Google Scholar]
- Chall JS, Dale E. Readability revisited: The new Dale-Chall readability formula. Cambridge, MA: Brookline Books; 1995. [Google Scholar]
- Charuvastra A, Cloitre M. Social bonds and posttraumatic stress disorder. Annual Review of Psychology. 2008;59:301–328. doi: 10.1146/annurev.psych.58.110405.085650. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chemtob CM, Novaco RW, Hamada RS, Gross DM, Smith G. Anger regulation deficits in combat-related posttraumatic stress disorder. Journal of Traumatic Stress. 1997;10:17–36. doi: 10.1023/a:1024852228908. [DOI] [PubMed] [Google Scholar]
- Christopher FS, Pflieger JC, Canary DJ, Guerrero LK, Holtzworth-Munroe A. Targeted neighborhood sampling: A new approach for recruiting abusive couples. Journal of Family Violence. 2008;23:89–100. [Google Scholar]
- Claesson K, Sohlberg S. Internalized shame and early interactions characterized by indifference, abandonment and rejection: Replicated findings. Clinical Psychology and Psychotherapy. 2002;9:277–284. [Google Scholar]
- Coan JA, Schaefer HS, Davidson RJ. Lending a hand: Social regulation of the neural response to threat. Psychological Science. 2006;17:1032–1039. doi: 10.1111/j.1467-9280.2006.01832.x. [DOI] [PubMed] [Google Scholar]
- Cohen J. The earth is round (p < .05) American Psychologist. 1994;49:997–1003. [Google Scholar]
- Cohen J. Statistical power analysis. Current Directions in Psychological Science. 1992;1:98–101. [Google Scholar]
- Constans JI, McCloskey M, Vasterling JJ, Bailey K, Mathews A. Suppression of attentional bias in PTSD. Journal of Abnormal Psychology. 2004;113:315–323. doi: 10.1037/0021-843X.113.2.315. [DOI] [PubMed] [Google Scholar]
- Covert MV, Tangney JP, Maddux JE, Heleno NM. Shame-proneness, guilt-proneness, and interpersonal problem solving: A social cognitive analysis. Journal of Social and Clinical Psychology. 2003;22:1–12. [Google Scholar]
- Dalgleish T. Cognitive approaches to posttraumatic stress disorder: The evolution of multirepresentational theorizing. Psychological Bulletin. 1994;130:228–260. doi: 10.1037/0033-2909.130.2.228. [DOI] [PubMed] [Google Scholar]
- DeKeseredy WS, Schwartz MD. Woman abuse on campus: Results from the Canadian National Survey. Thousand Oaks, CA: Sage; 1998. [Google Scholar]
- Dodge KA, Lansford JE, Burks VS, Bates JE, Pettit GS, Fontaine R, Price JM. Peer rejection and social information-processing factors in the development of aggressive behavior problems in children. Child Development. 2003;74:374–393. doi: 10.1111/1467-8624.7402004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dunmore E, Clark DM, Ehlers A. A prospective investigation of the role of cognitive factors in persistent Posttraumatic Stress Disorder (PTSD) after physical or sexual assault. Behaviour Research and Therapy. 2001;39:1063–1084. doi: 10.1016/s0005-7967(00)00088-7. [DOI] [PubMed] [Google Scholar]
- Dutra L, Callahan K, Forman E, Mendelsohn M, Herman J. Core schemas and suicidality in a chronically traumatized population. The Journal of Nervous and Mental Disease. 2008;196:71–74. doi: 10.1097/NMD.0b013e31815fa4c1. [DOI] [PubMed] [Google Scholar]
- Dutton D, van Ginkel C, Starzomski A. The role of shame and guilt in the intergenerational transmission of abusiveness. Violence and Victims. 1995;10:121–131. [PubMed] [Google Scholar]
- Ehlers A, Clark DM. A cognitive model of posttraumatic stress disorder. Behaviour Research and Therapy. 2000;38:319–345. doi: 10.1016/s0005-7967(99)00123-0. [DOI] [PubMed] [Google Scholar]
- Elison J, Pulos S, Lennon R. Shame-focused coping: An empirical study of the compass of shame. Social Behavior and Personality. 2006;34:161–168. [Google Scholar]
- Ferguson TJ, Eyre HL, Ashbaker M. Unwanted identities: A key variable in shame—anger links and gender differences in shame. Sex Roles. 2000;42:133–157. [Google Scholar]
- Foa E, Riggs D, Gershuny B. Arousal, numbing, and intrusion: Symptom structure of PTSD following assault. American Journal of Psychiatry. 1995;152:116–20. doi: 10.1176/ajp.152.1.116. [DOI] [PubMed] [Google Scholar]
- Gawronski B, Bodenhausen GV. Associative and propositional processes in evaluation: An integrative review of implicit and explicit attitude change. Psychological Bulletin. 2006;132:692–731. doi: 10.1037/0033-2909.132.5.692. [DOI] [PubMed] [Google Scholar]
- Gilbert P, Pehl J, Allan S. The phenomenology of shame and guilt: An empirical investigation. British Journal of Medical Psychology. 1994;67:23–36. doi: 10.1111/j.2044-8341.1994.tb01768.x. [DOI] [PubMed] [Google Scholar]
- Holtzworth-Munroe A. Social information processing skills deficits in maritally violent men: Summary of a research program. In: Vincent JP, Jouriles EN, editors. Domestic violence: Guidelines for research-informed practice. London: Jessica Kingsley; 2000. [Google Scholar]
- Hu L, Bentler PM. Cutoff criteria for fit indices in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling. 1999;6:1–55. [Google Scholar]
- Ishihara S. Tests for colour-blindness. Tokyo: Kanehara & Co., Ltd; 1939. [Google Scholar]
- Jones LV. Test of hypothesis: One-sided vs. two-sided alternatives. Psychological Bulletin. 1952;49:43–46. doi: 10.1037/h0056832. [DOI] [PubMed] [Google Scholar]
- Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry. 2005;62:593–602. doi: 10.1001/archpsyc.62.6.593. [DOI] [PubMed] [Google Scholar]
- Kessler RC. Posttraumatic stress disorder: The burden to the individual and to society. Journal of Clinical Psychiatry. 2000;61:4–12. [PubMed] [Google Scholar]
- Kubany ES. A cognitive model of guilt typology in combat-related PTSD. Journal of Traumatic Stress. 1994;7:3–19. doi: 10.1007/BF02111908. [DOI] [PubMed] [Google Scholar]
- Kubany ES, Leisen MB, Kaplan AS, Watson SB, Haynes SN, Owens JA. Development and preliminary validation of a brief broad-spectrum measure of trauma exposure: The Traumatic Life Events Questionnaire. Psychological Assessment. 2000;12:210–224. doi: 10.1037//1040-3590.12.2.210. [DOI] [PubMed] [Google Scholar]
- Kugler K, Jones WH. On conceptualizing and assessing guilt. Journal of Personality and Social Psychology. 1992;62:318–327. [Google Scholar]
- Larsen RJ, Mercer KA, Balota DA. Lexical characteristics of words used in emotional Stroop experiments. Emotion. 2006;6:62–72. doi: 10.1037/1528-3542.6.1.62. [DOI] [PubMed] [Google Scholar]
- Leskela J, Dieperink M, Thuras P. Shame and posttraumatic stress disorder. Journal of Traumatic Stress. 2002;15:223–226. doi: 10.1023/A:1015255311837. [DOI] [PubMed] [Google Scholar]
- Lewis HB. Shame and guilt in neurosis. Oxford: International Universities Press; 1971. [PubMed] [Google Scholar]
- MacLeod C, MacDonald P. Interdimensional interference in the Stroop effect: Uncovering the cognitive and neural anatomy of attention. Trends in Cognitive Sciences. 2000;4:383–391. doi: 10.1016/s1364-6613(00)01530-8. [DOI] [PubMed] [Google Scholar]
- Markus H. Self-schemata and processing information about the self. Journal of Personality and Social Psychology. 1977;35:63–78. [Google Scholar]
- Marshall AD, Panuzio J, Taft CT. Intimate partner violence among military veterans and active duty servicemen. Clinical Psychology Review. 2005;25:862–876. doi: 10.1016/j.cpr.2005.05.009. [DOI] [PubMed] [Google Scholar]
- McFall R. A review and reformulation of the concept of social skills. Behavioral Assessment. 1982;4:1–33. [Google Scholar]
- Merikle PM, Reingold EM. Recognition and lexical decision without detection: Unconscious perception? Journal of Experimental Psychology: Human Perception and Performance. 1990;16:574–583. doi: 10.1037//0096-1523.16.3.574. [DOI] [PubMed] [Google Scholar]
- Muthén LK, Muthén BO. Mplus user's guide. 4th. Los Angeles: Author; 2006. [Google Scholar]
- Nisbett RE, Wilson TD. Telling more than we can know: Verbal reports on mental processes. Psychological Review. 1977;84:231–259. [Google Scholar]
- Olff M, Langeland W, Draijer N, Gersons BPR. Gender differences in posttraumatic stress disorder. Psychological Bulletin. 2007;133:183–204. doi: 10.1037/0033-2909.133.2.183. [DOI] [PubMed] [Google Scholar]
- Ozer EJ, Best SR, Lipsey TL, Weiss DS. Predictors of posttraumatic stress disorder and symptoms in adults: A meta-analysis. Psychological Bulletin. 2003;129:52–73. doi: 10.1037/0033-2909.129.1.52. [DOI] [PubMed] [Google Scholar]
- Paynter DE, Bodrova E, Doty JK. For the love of words: Vocabulary instruction that works. San Francisco, CA: Jossey-Bass; 2005. [Google Scholar]
- Preacher KJ, Hayes AF. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behavior Research Methods, Instruments & ComputersSpecial Issue: Web-based archive of norms, stimuli, and data: Part 2. 2004;36:717–731. doi: 10.3758/bf03206553. [DOI] [PubMed] [Google Scholar]
- Preacher KJ, Rucker DD, Hayes AF. Addressing moderated mediation hypotheses: Theory, methods, and prescriptions. Multivariate Behavioral Research. 2007;42:185–227. doi: 10.1080/00273170701341316. [DOI] [PubMed] [Google Scholar]
- Resick PA, Schnicke MK. Cognitive processing therapy for rape victims: A treatment manual. Newbury Park, CA: Sage; 1993. [Google Scholar]
- Schumacher JA, Feldbau-Kohn S, Smith Slep AM, Heyman RE. Risk factors for male-to-female partner physical abuse. Aggression and Violent Behavior. 2001;6:281–352. [Google Scholar]
- Shalev AY, Freedman S, Peri T, Brandes D, Sahar T. Predicting PTSD in trauma survivors: Prospective evaluation of self- report and clinician-administered instruments. The British Journal of Psychiatry. 1997;170:558–564. doi: 10.1192/bjp.170.6.558. [DOI] [PubMed] [Google Scholar]
- Straus MA, Gelles RJ. Physical violence in American families: Risk factors and adaptations to violence in 8,145 families. New Brunswick, NJ: Transaction; 1990. pp. 542–543. [Google Scholar]
- Straus MA, Hamby SL, Boney-McCoy S, Sugarman DB. The revised Conflict Tactics Scales (CTS2): Development and preliminary psychometric data. Journal of Family Issues. 1996;17:283–316. [Google Scholar]
- Stroop JR. Studies of interference in serial verbal reactions. Journal of Experimental Psychology: General. 1935;121:15–23. [Google Scholar]
- Stuart GL, Moore TM, Gordon KC, Ramsey SE, Kahler CW. Psychopathology in women arrested for domestic violence. Journal of Interpersonal Violence. 2006;21:376–389. doi: 10.1177/0886260505282888. [DOI] [PubMed] [Google Scholar]
- Stuewig J, Tangney JP, Heigel C, Harty L, McCloskey L. Shaming, blaming, and maiming: Functional links among the moral emotions, externalization of blame, and aggression. Journal of Research in Personality. 2010;44:91–102. doi: 10.1016/j.jrp.2009.12.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Taft CT, Schumm JA, Marshall AD, Panuzio J, Holtzworth-Munroe A. Family-of-origin maltreatment, posttraumatic stress disorder symptoms, social information processing deficits, and relationship abuse perpetration. Journal of Abnormal Psychology. 2008;117:637–646. doi: 10.1037/0021-843X.117.3.637. [DOI] [PubMed] [Google Scholar]
- Taft CT, Vogt DS, Marshall AD, Panuzio J, Niles BL. Aggression among combat veterans: Relationships with combat exposure and symptoms of posttraumatic stress disorder, dysphoria, and anxiety. Journal of Traumatic Stress. 2007;20:135–145. doi: 10.1002/jts.20197. [DOI] [PubMed] [Google Scholar]
- Tangney JP, Dearing RL. Shame and guilt. New York, NY: Guilford Press; 2002. [Google Scholar]
- Vega EM, O'Leary KD. Test-retest reliability of the revised Conflict Tactics Scales (CTS2) Journal of Family Violence. 2007;22:703–708. [Google Scholar]
- Watson D. Rethinking the mood and anxiety disorders: A quantitative hierarchical model for DSM–V. Journal of Abnormal Psychology. 2005;114:522–536. doi: 10.1037/0021-843X.114.4.522. [DOI] [PubMed] [Google Scholar]
- Weathers FW, Keane TM, Davidson JRT. Clinician-Administered PTSD scale: A review of the first ten years of research. Depression and Anxiety. 2001;13:132–156. doi: 10.1002/da.1029. [DOI] [PubMed] [Google Scholar]
- Weathers FW, Litz BT, Herman DS, Huska JA, Keane TM. The PTSD Checklist: Reliability, validity, & diagnostic utility. Unpublished Paper presented at the Annual Meeting of the International Society for Traumatic Stress Studies.1993. [Google Scholar]
- Weathers FW, Ruscio AM, Keane TM. Psychometric properties of nine scoring rules for the Clinician-Administered Posttraumatic Stress Disorder Scale. Psychological Assessment. 1999;11:124–133. [Google Scholar]
- Whitaker DJ, Morrison S, Lindquist C, Hawkins SR, O'Neil JA, Nesius AM, et al. Reese L. A critical review of interventions for the primary prevention of perpetration of partner violence. Aggression and Violent Behavior. 2006;11:151–166. [Google Scholar]
- Widiger TA, Clark LA. Toward DSM–V and the classification of psychopathology. Psychological Bulletin. 2000;126:946–963. doi: 10.1037/0033-2909.126.6.946. [DOI] [PubMed] [Google Scholar]
- Williams JMG, Mathews A, MacLeod C. The emotional Stroop task and psychopathology. Psychological Bulletin. 1996;120:3–24. doi: 10.1037/0033-2909.120.1.3. [DOI] [PubMed] [Google Scholar]
- Wolfe DA, Wekerle C, Scott K, Straatman A, Grasley C. Predicting abuse in adolescent dating relationships over 1 year: The role of child maltreatment and trauma. Journal of Abnormal Psychology. 2004;113:406–415. doi: 10.1037/0021-843X.113.3.406. [DOI] [PubMed] [Google Scholar]