

1 Introduction
Japan is said to have eradicated filariasis some 25 years ago, but the exact time (and even the definition of eradication) is not clear. However, the results of successful control programs clearly indicate that the number of microfilaria carriers had been reduced to a very low level long before the “eradication”. As filariasis disappeared, the once stigmatized disease quickly lost clinical significance. At the same time, the number of parasitologists and researchers interested in filariasis dwindled quickly to only a handful in the whole country 10-15 years after the disappearance. Filariasis problems in Japan still remain as sequelae of the old infection. However, young clinicians have little knowledge of filariasis, and the rare, localized and non-lethal disease is disappearing also from the memory of doctors. On the other hand, some doctors continue to encounter cases of lymphedema, hydrocele and chyluria. Some of these are diagnosed as filarial in origin, and in most cases the diagnosis is based on the fact that the patients were born and brought up in the past endemic areas. Practically, there is no reliable way of diagnosing the old clinical filariasis. Some immunodiagnostic methods are available but they are not very specific.
The purpose of this review is to describe what is happening with filariasis in Japan about 25 years after its eradication. The review will highlight the situation of chyluria, the most common sequela, and its treatment, recent filarial infections in Japan including imported cases and zoonotic filariasis, and immunodiagnostic methods used for suspected clinical filariasis.
2 When did filariasis disappear from Japan?
In starting this review it will be necessary to address the question of when filariasis was “eradicated” in Japan. Experts agree that it disappeared sometime in the late 1970s, but nobody can pinpoint the exact year. It would seem that the filarial infection disappeared before anyone started to worry about the definition of eradication, or evaluation criteria for eradication. Thus, it is likely that little room was left for precise research on the “specific day” in the final stage of mop-up. The government of Japan initiated, in 1962, the National Filariasis Control Program in parts of Kyushu, Shikoku and Tokyo (Izu Islands) mainly based on chemotherapy with diethylcarbamazine (DEC). The program was very successful, and the number of microfilaria carriers decreased quickly. In a low-endemic area of Ehime prefecture (microfilaria rate: 1.01% in 1961), no microfilaremic case was detected by 1967 (Hatano, 1986) [1], though Sasa (1976) [2] recorded the last cases in 1969. In Kagoshima prefecture, the microfilaria rate of 6.6% in 1962 came down to 0 in 1975 (Fukushima, 1998) [3]. In highly endemic Okinawa, the former Ryukyu that was under U.S. occupation from 1945 to 1972, the eradication program was started in 1965 with the assistance of the U.S. Civil Administration of the Ryukyu Islands and the Japanese government. The last microfilaria carrier was reported there in 1978 (Yoshida, 1988) [4].
For the confirmation of microfilaremia at a low level, the nuclepore-filtration method with 1 ml of venous blood was introduced in 1979 at Bonotsu-cho, Kagoshima prefecture (Fukumoto, 1984) [5], and in 1980 at Kuroshima, Okinawa (Tada et al., 1982) [6]. No microfilaria-positive person was detected in these studies. However, Teruya et al. (1982) [7] wrote that two microfilaria carriers were reported after 1980 in Okinawa. Itoh et al. (1999) [8] reported one chyluria patient who showed a high level of filaria-specific IgG4, suggesting that adult worms had been surviving until recent years.
In conclusion, microfilaria carriers disappeared from Japan, most probably in the early 1980s. It was possible that adult worms, which are pathogenic, survived for some more years.
3 Chyluria
3.1 Occurrence of clinical cases after the interruption of filarial transmission
The number of case reports on chyluria in Japan is limited. We encountered only 14 full papers and 14 abstracts of oral presentations since 1982 by screening Igaku-Chuo-Zasshi (Japana Centra Revuo Medicina), which is the Japanese equivalent of Index Medicus, covering most medical and related journals published in Japan and records of medical conferences/meetings. A majority of case reports are made by doctors working in non- (or low-) endemic areas of Japan, where the disease is considered very rare, and therefore worthy of reporting. It is of interest to note that most reports mentioned Okinawa or Kyushu as a place of birth or residence of patients, suggesting that a history of residence in the past endemic areas is a key for the diagnosis of filarial origin.
Amami Oshima, Kagoshima prefecture (Kyushu) used to have a high prevalence of filariasis (microfilaria rate in 1962: 10.3%). It is interesting to look at what happened to clinical cases after filariasis transmission ceased completely. The clinical statistical data from the Urology Section of Kagoshima Prefectural Oshima Hospital will be informative in this regard (Kawahara et al., 1992; Kubo et al., 1992) [9, 10]. The yearly number of chyluria, scrotal elephantiasis and hydrocele cases from 1981 to 1990 is shown in Table 1 for outpatients and inpatients. During the 10 year-period, there were 15,225 outpatients, of which 382 cases (2.5%) had chyluria, 13 (0.09%) had scrotal elephantiasis and 527 (3.5%) had hydrocele testis. It is interesting to note that the annual occurrence of chyluria (30-45 cases) and hydrocele (38-64 cases) was almost the same during the 10 years, while the number of scrotal elephantiasis cases seemed to decrease (though not conclusive). For inpatients, the situation was basically the same. Among 1,701 inpatients in the 10-year period, chyluria and hydrocele accounted for 60 (3.5%) and 79 (4.6%) cases respectively, and there was no decrease in the occurrence by year. The authors specifically commented that newly-developed chyluria cases were encountered at a rate of about one case per month 10 years after the filariasis eradication. Contrary to this comment, Fukumoto (1984) [5], at Bonotsu-cho, Kagoshima prefecture, reported a steady decrease in elephantiasis, hydrocele and chyluria cases as the filariasis control program progressed. In 1965, there were 43 (4.0%) clinical cases out of 1,064 examined, which decreased to 5 cases (0.8%) out of 640 in 1980, and all of these 5 cases were people aged 54-75 years. (Note: The numbers examined (1,064 and 640) are an estimate made by the present reviewers.)
Table 1:
The number of possible clinical filariasis registered at Kagoshima Prefectural Oshima Hospital in 1981-1990
| 1981 | 1982 | 1983 | 1984 | 1985 | 1986 | 1987 | 1988 | 1989 | 1990 | Total | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Outpatients (n=15225*) | |||||||||||
| Chyluria | 43 | 31 | 36 | 43 | 40 | 38 | 38 | 38 | 30 | 45 | 382 |
| Scrotalelephantiasis | 1 | 1 | 5 | 2 | 1 | 2 | 0 | 1 | 0 | 0 | 13 |
| Hydrocele testis | 49 | 38 | 44 | 57 | 51 | 62 | 54 | 61 | 64 | 47 | 527 |
| Inpatients (n=1701*) | |||||||||||
| Chyluria | 7 | 7 | 4 | 7 | 6 | 11 | 1 | 3 | 3 | 11 | 60 |
| Hydrocele testis | 6 | 7 | 7 | 13 | 6 | 10 | 4 | 5 | 7 | 14 | 79 |
What will be the reasons for the continuing occurrence of new chyluria cases many years after the interruption of filarial transmission? There would be three possibilities: (1) permanent damage to the lymphatic tissues left by filarial infection was activated or worsened by bacterial infections, injuries, pregnancies, tumors, etc; (2) adult worms could survive longer than expected and continued damaging the lymphatic system; and (3) non-filarial chyluria might be incorrectly included in counting. With regard to the first possibility, there are some supporting reports: A case of chyluria was reported cured simply by treatment for concurrent renal tuberculosis (Kawakami et al., 1998) [11]. On the contrary, the treatment of tuberculosis was followed by fresh chyluria in another case (Nakao and Shiotani, 1985) [12], suggesting interaction between the two diseases. Koga et al. (1982) [13] reported that of 155 chyluria cases, 85 had complications of various types, the most common being genitourinal (71 cases), and that the treatment of complications alone improved chyluria in 59.5% of those treated. In other cases, chyluria started during pregnancy (Mandai et al.. 1990) [14] and was complicated with non-active adrenal tumor (Takeichi et al., 1989) [15].
The second possibility is supported by two facts: the very long life span of adult worms (up to 40 years!) (Carme and Laigret, 1979) [16], and the persistence of circulating filaria antigens, products of live adult worms, for years even after treatment had cleared microfilaremia (Zheng et al., 1990) [17].
The third possibility is without evidence. However, as the diagnosis of filarial chyluria is sometimes based simply on a history of residence in endemic areas, or a simplified criterion like “no obstruction of the thoracic duct is indicative of filarial chyluria,” misdiagnosis could indeed occur.
3.2 Does chyluria cause immunological incompetence?
Tamaki (1984) [18] showed that the number of peripheral T lymphocytes was significantly lower in chyluria patients than in healthy controls. The T cell reduction was particularly evident during the aggravation stage of chyluria (Fig. 1). Also, 3H-thymidine uptake by lymphocytes after phytohemagglutinin (PHA) stimulation revealed significantly lower uptake in chyluria patients. Koga et al. (1985) [19] reported that lymphopenia was observed in 63 of 124 (50.8%) chyluria patients, and Koyama et al. (1990) [20] showed a clear inhibition of PHA-induced blast formation of lymphocytes among chyluria cases.
Fig. 1.
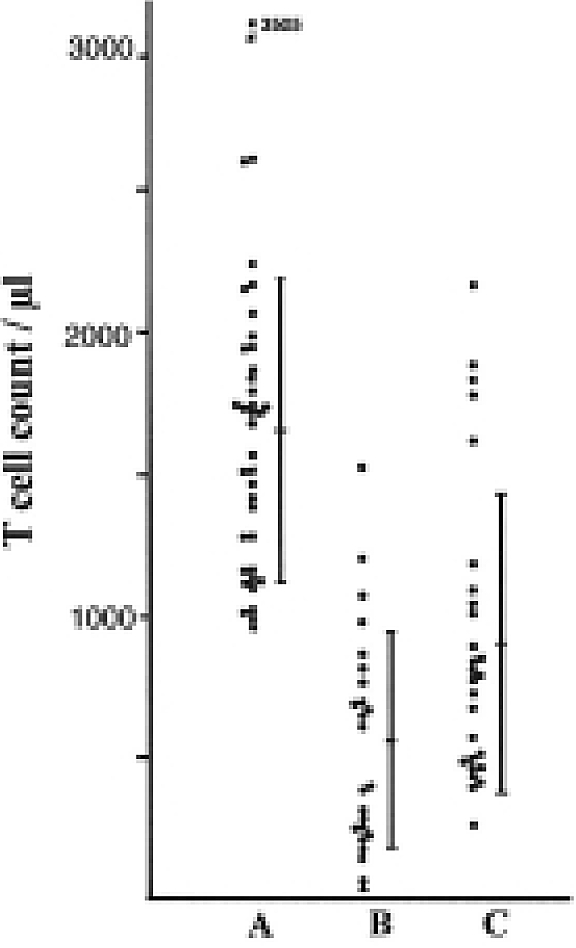
Comparison of T cell counts.
A: Control, B: Chyluria cases during aggravation, C: Chyluria cases in remission [Quoted from Tamaki, Trop Med [18]]
With regard to decreased cellular immunity, some reports suggested a higher occurrence of malignancies among filarial chyluria patients. For example, Koyama et al. (1989) [21] reported 26 malignancies out of 162 chyluria cases (16%) in Okinawa which was more than 25 times higher than the national average. Such observations have to be analyzed carefully, because malignancies could be the cause of chyluria. When chyluria patients were divided into 2 groups according to the positivity of toxoplasmosis indirect hemagglutination test (IHA), the IHA positive group had a significantly lower number of peripheral lymphocytes and T cells (Tamaki, 1984) [18]. A chyluria case with lymphopenia and reduced CD4+ cells complicated with cryptococcal infection was also reported (Honda et al., 2003) [22].
With regard to W. bancrofti infection (not necessarily to chyluria), a positive relationship between antibody levels to filarial antigen and positive rates of antibodies to adult T-cell leukemia (ATL) virus-associated antigen was reported (Tajima et al., 1983; Fujita et al., 1986) [23, 24]. It was supposed that filariae exerted a promoting effect on ATL virus infection and proliferation.
3.3 Treatments of chyluria
The treatments for chyluria employed in Japan after 1980 are basically the same classical methods: intrarenal pelvic instillation with silver nitrate (mostly 0.1-0.5%) by means of catheterization and then, if required, renal lymph vessel occlusion (Katamine, 1966) [25] or stripping and interruption (ligation) of the renal pedicle lymphatics. Of 47 cases reported at various institutions in Japan between 1984 and 2003, silver nitrate only was used in 15 cases. Six cases needed renal operation as the silver nitrate treatment was not successful. Ten cases were deemed to need surgery from the beginning. The operation, renal lymph vessel occlusion, is said to be very effective and safe (Okamoto and Ohi, 1983) [26]. However, a report by Takigawa et al. (1988) [27] showed a possibility of severe adverse reaction after the operation. A 57-year-old male suffered from renal arterial thrombosis after bilateral stripping and ligation, which resulted in complete loss of left renal function. Apparently, this rare operation provided a good subject for case reports and thus accounts for a large proportion of reported treatments. Treatments with low-fat diet and lymphangiography were also reported.
Several new attempts were made to treat chyluria. A 50-year-old woman received bilateral inguinal lymph nodesaphenous vein anastomosis and right inguinal lymphangiovenous anastomosis (Muguruma et al., 1994) [28]. The chyluria disappeared within 5 months after operation. The procedure, which had been tested successfully in China was recommended as an effective, simple and less invasive surgical method, suitable for aged patients. Endoscopic coagulation was utilized in 5 chyluria cases (Yagi et al., 1998) [29]. No recurrence occurred among the patients during the 16-34 month-period of observation.
4 Other clinical manifestations of bancroftian filariasis in Japan
Hydrocele used to be more common than chyluria in endemic areas (Katamine, 1966) [25]. The cases recorded at the Kagoshima Prefectural Oshima Hospital accounted for 3.5% of the total number of outpatients, and did not decrease during the 1981-1990 period (Kubo et al. 1992) [10]. However, it is interesting to find that hydrocele is rarely mentioned in relation to filarial infection in recent studies. Even Kubo et al. above, dealt with hydrocele separately from filariasis in their statistics. This is probably because of difficulty in determining the true cause of this clinical condition. Only 2 full papers (Sakurai et al., 1985; Matsui et al., 1995) [30, 31] and 3 abstracts on “filarial” hydrocele are found, including 11 cases. Suspecting filarial origin, Maeda et al. (2000) [32] mentioned that around 15 new hydrocele cases per year visited their hospital in Miyakojima, Okinawa.
Acquired lymphangioma of the scrotum, or lymphoscrotum, is a rare condition observed in lymphatic filariasis. Multiple papules, whitish to reddish in color, appear on the scrotal skin. They break easily and discharge often milky lymph fluid. Hagiwara et al. (1994) [33] compiled 6 cases of filarial lymphangioma, including lymphoscrotum and lesions on the vulva and penis. After 1994, 7 more cases were reported, 6 of which were treated successfully by resection of the affected lesion and a subsequent skin graft (Hannita et al., 1997; Takahata et al., 1998) [34, 35]. Yet another patient, who discharged more than 2,000 ml of lymph per day at one point, was treated with an anti-platelet drug, cilostazol, and showed clinical improvement (Masuzawa et al., 2001)[36].
5 Imported cases of filariasis
The first loiasis case in Japan was reported in 1985 (Tani et al., 1985) [37]. The patient was a 33-year-old male German, who had traveled for 2 months in Africa. Fugitive swelling was observed and microfilariae were positive, showing diurnal periodicity The second case was a 53-year-old Japanese man who had lived in Zaire. An adult worm was removed from the right ocular conjunctiva. Microfilariae were also positive (Ohtaki et al., 1988; Kamikawatoko et al., 1989) [38, 39]. The third case, reported in 1997, was a 28-year-old Gabonese male. Microfilariae were positive and a moving adult worm was noticed in the conjunctiva (Yara et al., 2001) [40]. A 29-year-old male Nigerian case was reported in 1998 (Yasuki et al., 1998) [41]. Adult worm was found moving in a conjunctival nodule and removed surgically. No microfilaria was found. Additionally, a 32-year-old Japanese woman, who had traveled in more than 40 countries in Africa was reported as a loiasis patient without parasitological confirmation (Yoshikawa et al., 2003) [42]. She experienced a subcutaneous nodule that showed repeated appearance and disappearance at intervals of about a week. The ELISA with Dirofilaria immitis antigen was positive. Yet another Japanese case was reported in 1984, but without confirmation.
The first Dipetalonema perstans infection was reported in a 34-year-old Japanese man who had worked in Zaire for a study on chimpanzees (Yoshida et al., 1983) [43]. A subcutaneous nodule was noticed, and microfilariae were positive in the blood. These were unsheathed and did not show periodicity. The second case was also a Japanese researcher on primates, a 40-year-old male, who had worked in Cameroon (Hioki et al., 1986) [44]. A 28-year-old male Nigerian with microfilariae was diagnosed as having D. perstans infection (Iiyama et al., 2000) [45].
Onchocerca volvulus infection was reported in a Japanese man (34 years) who had lived in Guinea, Gabon and Jordan (Yoshimura, 1983) [46]. A subcutaneous nodule was observed on the left buttock. The nodule was removed surgically and the pathological sections revealed an O. volvulus adult female.
A Japanese case of tropical pulmonary eosinophilia (52-year-old male) was reported (Oyamada et al., 1995) [47]. The patient, who had worked in Vietnam for about 3 years, experienced chest pain, wheezing, pleural effusion, eoshinophilia (59%), high serum IgE (708 IU) and positive antibody test against D. immitis antigen. DEC and steroid elicited a swift improvement. A Sri Lanlcan case, 21 year-old male, of tropical pulmonary eosinophilia was reported by Hayashi et al. (1996) [48].
Microfilariae of Wuchereria bancrofti and Brugia malayi were found in the hydrocele fluid of a 27-year-old Chinese man (1990) and a 36-year-old Sri Lankan man (1996), respectively. The latter case seems to be very rare, as it is generally believed that hydrocele associates with W. bancrofti, not B. malayi.
6 Zoonotic onchocerciasis in Japan
D. immitis infection of humans, which will be reviewed separately by Akao (Akao N. this issue: 65-71), is an important zoonotic filariasis in Japan. In addition, zoonotic onchocercal infections were reported in Oita prefecture, Kyu-shu. The first case was a 2-year-old girl with subcutaneous swelling on the sole of the left foot (Hashimoto et al., 1990) [49]. Biopsy specimens revealed a mature female parasite that was suspected to be O. gutturosa or O. cervicalis (Beaver et al., 1989) [50]. Two more cases were reported from Oita prefecture: A 57-year-old woman with a painful nodule on the wrist was suspected to be infected with O. gutturosa (Takaoka et al., 1996) [51], and a 52-year-old woman with subcutaneous swelling on the left retroauricular region was diagnosed as having a new subspecies, O. dewittei japonica (Takaoka et al., 2001) [52]. The authors raised the possibility that the 57-year-old case, was in fact O. dewittei japonica infection.
7 Immunodiagnoses
Without active filariasis in Japan, the definite diagnosis of filarial chyluria, hydrocele and lymphedema/elephantiasis is difficult and is therefore made by exclusion. The diagnosis of filariasis is often made or suspected when the cases are of old age and brought up in previously endemic areas. To distinguish filarial and non-filarial chyluria, several papers stress the importance of thoracic duct obstruction, the absence being evidence of filarial chyluria. Often, immunodiagnoses are the only way to discern past filarial infections. A gel double diffusion test and ELISAs, including dot ELISA, have been employed most frequently to detect antifilarial antibodies.
In most reports, anti-filarial antibodies were detected using D. immitis antigens. In zoonotic human onchocerciasis cases, ELISA was carried out with O. volvulus or O. gutturosa antigens (Takaoka et al., 1996; Korenaga et al., 1983) [51, 53]. In suspected bancroftian filariasis, the Department of Parasitology, Aichi Medical University has used, on request, Og4C3 ELISA or ICT card tests to detect W. bancrofti antigen and ELISA to detect filaria-specific IgG4. With the aim of detecting old infections, Itoh et al. (1999) [8] developed an IgG ELISA using B. pahangi adult female antigens. The ELISA was tested with microfilaria positives from Sri Lanka (positive control), normal Japanese (negative control), and 16 chyluria patients who were born and brought up in Okinawa. In order to increase specificity, sample sera were absorbed with several species of nematode antigens. The absorption with Anisakis larval antigens and D. immitis antigens produced satisfactory results (Fig. 2). With this ELISA, 5 of 16 chyluria cases were considered filarial. As for lymphedema cases, 34 suspected patients were examined between 1996 and June 2003, at the request of clinicians. A high IgG4 titer was obtained from 1 person aged 82 years, and high IgG titers from 3 persons.
Fig. 2.

Anti-B. pahangi IgG antibodies in serum samples. The samples were absorbed with D. immitis and/or Anisakis sp. antigens [Quoted from Itoh et al., Jpn J Trop Med Hyg [8]]
Serum samples without absorption (A). Samples absorbed with D. immitis antigens (B), Anisakis antigens (C), and both D. immitis and Anisakis antigens (D). Left column: chyluria patients, Middle column: Japanese healthy controls, Right column: Sri Lankan microfilaria positives.
Short horizontal bar: the mean of antibody titers. The means were compared before (A) and after absorption (B, C, D) with t-test; * for p<0.05, ** for p<0.0l. An arrow in panel (D) indicates a cut-off point.
Acknowledgement
This paper is revised from Asian Parasitology Vol. 3 Filariasis in Asia and Western Pacific Islands, 137-144 by The Federation of Asian Parasitologists in 2004.
References
(Paper titles with * are translated from Japanese by the present reviewers)
- 1.Hatano K. editor. Filaria-sho Kokufuku, Ehime-ken Filaria-Taisaku Kyougikai, 1986 (in Japanese).
- 2.Sasa M. Human Filariasis—a global survey of epidemiology and control, University of Tokyo Press: Tokyo, 1976.
- 3.Fukushima H. Achievement of filariasis prevention and control in Kagoshima (1962-1971), according to institution*. Kagoshimaken Naikai Kaiho. 1998; 30: 11-27 (in Japanese). [Google Scholar]
- 4.Yoshida C. Filaria Sousoukyoku. Okinawa Koshu-Eisei Kyokai, 1988 (in Japanese).
- 5.Fukumoto H. Follow-up study on the outcome of filarial mass treatment. Hukuoka Acta Medica 1984; 75: 484-495 (in Japanese). [PubMed] [Google Scholar]
- 6.Tada I, Otsoji Y, Harada R, Mimori T, Fukumoto H. Skin test study of bancroftian filariasis in Kuroshima Island, Okinawa: A 13-year longitudinal study during a control campaign. Am J Trop Med Hyg 1982; 31: 962-967 [DOI] [PubMed] [Google Scholar]
- 7.Teruya K, Taira K, Miyagi J. Change and development of health administration policy in the post-war Okinawa (4th report). Filariasis—the control and latest situation*. Minzoku-Eisei 1982; 48: 108-115 (in Japanese). [Google Scholar]
- 8.Itoh M, Qiu X-G, Koyama Y, Ogawa Y, Weerasooriya MV, Visanou H, Fojimaki Y, Kimura E. Detection of circulating Wuchereria bancrofti antigen, filaria-specific IgG and IgG4 in chyluria cases in Japan. Jpn J Ttop Med Hyg 1999; 27: 483-486 [Google Scholar]
- 9.Kawahara K, Kubo H, Kakinoki T, Chan YF, Saita H, Yamashita J, Shirahama T, Kayajima T, Kawahara M, Ikeda K, Makinose S, Matsusako T, Yagi S, Nishida M, Yamauchi D, Eta S. Statistical observations on inpatients and operations at the urological clinic of Kagoshima Prefectural Oshima Hospital from 1981 to 1990. Nishinihon Journal of Urology 1992; 54: 2283-2288 (in Japanese). [Google Scholar]
- 10.Kubo H, Kawahara K, Kakinoki T, Chan YF, Saita H, Yamashita J, Shirahama T, Kayajima T, Kawahara M, Makinose S, Ikeda K, Matsusako T, Yagi S, Nishida M, Yamauchi D, Eta S. Statistical observations on outpatients in the urological clinic of Kagoshima Prefectural Oshima Hospital from 1981 to 1990. Nishinihon Joumal of Urology 1992; 54: 2013-2018 (in Japanese). [Google Scholar]
- 11.Kawakami K, Kinjo T, Higa T, Kagawa M, Ooyama T. A case of chyluria cured by the treatment of renal tuberculosis*. Jpn Journal of Urological Surgery 1998; 11544 (abstract only, in Japanese). [Google Scholar]
- 12.Nakao M, Shiotani N. A suspected case of filarial chyluria*. Teishin Igaku 1985; 37: 509 (abstract only, in Japanese). [Google Scholar]
- 13.Koga N, Matsuoka M, Ooyama T. New understanding on chyluria*. Jpn J Urol 1982; 73: 1611-1612 (in Japanese). [Google Scholar]
- 14.Mandai M, Adachi N, Itoh H, et al. A case of suspected filarial chyluria that was induced during pregnancy*. Adv Obstet Gynecol 1990; 42: 746-748 (in Japanese). [Google Scholar]
- 15.Takeichi Y, Omae H, Hara S, et al. A case of adrenal tumor who visited hospital with a complaint of chyluria. Jpn J Urol 1989; 80: 468-469 (in Japanese). [Google Scholar]
- 16.Carme B, Laigret J. Longevity of Wuchereria bancrofti var. pacifica and mosquito infection acquired from a patient with low level parasitemia. Am J Trop Med Hyg 1979; 28: 53-55 [DOI] [PubMed] [Google Scholar]
- 17.Zheng H-J, Tao Z-H, Cheng W-F, Xu M, Fang R-L, Piessens WF. Parasite antigenemia in untreated and treated lymphatic filarial infections. A J Trop Med Hyg 1990; 43: 481-488 [PubMed] [Google Scholar]
- 18.Tamaki K. Clinico-immunological studies of filarial chyluria. Trop Med (Nagasaki) 1984; 26: 107-116 (in Japanese). [Google Scholar]
- 19.Koga S, Arakaki Y, Matsuoka M, Ohoyama C. Clinical study on chyluria. Jpn J Lymphol 1985; 8: 51-53 (in Japanese). [Google Scholar]
- 20.Koyama Y, Chinen Y, Ogura H, Shishido S, Higa I, Hatano T, Hayakawa M, Osawa A. Immunological study on chyluria. Jpn J Urol 1990; 81: 1212-1216 [DOI] [PubMed] [Google Scholar]
- 21.Koyama Y, Hayakawa M, Osawa A. Occurrence rate of malignancy and cellular immunity in chyluria patients*. Proceedings of the Japanese Cancer Association (48th Meeting) 1989; 82 (in Japanese).
- 22.Honda A, Furumoto A, Ikeda H, et al. A case of cryptococcal meningitis in a lymphopenic patient with fiIarial chyluria*. J J A Inf D 2003; 77: 389 (abstract only, in Japanese). [Google Scholar]
- 23.Tajima K, Fujita K, Tsukidate S, Oda T, Tominaga S, Suchi T, Hinuma Y. Seroepidemiological studies on the effects of filarial parasites on infestation of adult T-cell leukemia virus in the Goto Islands, Japan. Gann 1983; 74: 188-191 [PubMed] [Google Scholar]
- 24.Fujita K, Tsukidate S, Horii Y, Nakanishi H, Terashima K, Harada R, Otsuji Y. Influence of filaria and Strongyloides infection on the infestation of adult T-cell leukemia virus. Survey on Kikai-Island, Kagoshima Prefecture, endemic place of ATL virus and Strongyloides infection. Trop Med (Nagasaki) 1986; 28: 293-299 (in Japanese). [Google Scholar]
- 25.Katamine D. On the clinical and pathological problems of filariasis. In: Morishita K, Komiya Y, Matsubayashi H, editors. Progress of Medical Parasitology in Japan Vol. 3. Tokyo: Meguro Parasitological Museum, 1966: 441-466.
- 26.Okamoto K, Ohi Y. Recent distribution and treatment of filarial chyluria in Japan. Journal of Urology 1983; 129: 64-67 [DOI] [PubMed] [Google Scholar]
- 27.Takigawa H, Kagawa S, Aga Y, Uema K, Sumiyoshi Y, Inai T, Tamura M. Renal artery thrombosis following surgical treatment of chyluria. Acta Urologica Japonica 1988; 34: 1631-1634 (in Japanese). [PubMed] [Google Scholar]
- 28.Muguruma K, Matsuda T, Koyama Y, Komatsu Y. Chyluria treated with inguinal lymphangiovenous and lymph node-venous anastomosis: A case report. Jpn J Urol 1994; 85: 1571-1574 (in Japanese). [DOI] [PubMed] [Google Scholar]
- 29.Yagi S, Goto T, Kawamoto K, Miyawaki I, Tanaka I, Mori K, Hayami H, Ohi Y. Endoscopic treatment of refractory filarial chyluria: a preliminary report. J Urol 1998; 159: 1615-l618 [DOI] [PubMed] [Google Scholar]
- 30.Sakurai M, Yamasaki Y, Tsukamoto K, Yamakawa K, Nishii M, Tada S. A case of hydrocele testis secondary to filariasis. Jpn J Clin Urol 1985; 39: 621-623 (in Japanese). [Google Scholar]
- 31.Matsui M, Hirase Y, Yamamichi H. Case of a giant hydrocele testis believed caused by filariasis. J Jpn PRS 1995; 15: 818-823 (in Japanese). [Google Scholar]
- 32.Maeda H, Gakiya M. Seven cases of hydrocele/hematocele who had secondary infections*. Jpn Journal of Urological Surgery 2000; 13: 832 (abstract only, in Japanese). [Google Scholar]
- 33.Hagiwara K, Toyama K, Miyazato H, Nonaka S. A case of acquired lymphangioma due to a suspected old filariasis and a review of literature. J Dermatol 1994; 21: 358-362 [DOI] [PubMed] [Google Scholar]
- 34.Hannita Y, Nonaka S, Miyazato H. Acquired lymphangioma of the scrotum as a sequela of filariasis. Rinsho 62 Derma (Tokyo) 1997; 39: 1879-1882 (in Japanese). [Google Scholar]
- 35.Takahata H, Hamamoto Y, Nakano J, Muto M. A case of genital elephantiasis due to bancroftian filarial. Jpn J Clin Dermatol 1998; 52: 925-927 (in Japanese). [Google Scholar]
- 36.Masuzawa M, Hara H, Miyata T, Amano T, Asai T, Katoh I, Nishiyama S, Katsuoka K. Severe lymphorrhea and lymphedema caused by filariasis: The eflicacy of oral treatment with cilostazol. Jpn J Dermatol 2001; 111: 179-183 (in Japanese). [Google Scholar]
- 37.Tani S, Shibuya T, Beisler GK, Tanaka H, Paulisch FE. An imported case of human infection with Loa loa. Japan J Exp Med 1985; 55: 71-74 [PubMed] [Google Scholar]
- 38.Ohtaki N, Oka K, Kato T, Sugiyama E, Shinonaga S, Kamikawadoko S, Nawata H, Sazaki S. A case of loiasis*. Rinsho Derma 1988; 30: 1063-1067 (in Japanese). [DOI] [PubMed] [Google Scholar]
- 39.Kamikawatoko S, Sato A, Kamata K, Sugiyama E, Nawata H, Ohtaki N. A case of loiasis. Journal of the eye 1989; 6: 97-100 (in Japanese). [DOI] [PubMed] [Google Scholar]
- 40.Yara S, Higa F, Arakaki N, Ishimine T, Shinzato T, Toma H, Saito A. A case of loiasis. J J A Inf D 2001; 75: 151-154 (in Japanese). [DOI] [PubMed] [Google Scholar]
- 41.Yasuki K, Miyazaki S, Tabuchi A, Hatsushika R, Okino T, Akamatsu T. A case of loiasis in a Nigerian in Japan. Folia Ophthalmol Jpn 1998; 49: 620-623 (in Japanese). [Google Scholar]
- 42.Yoshikawa K, Sato F, Komatsuzaki M, et al. A case of loiasis treated with albendazole*. J J A Inf D 2003; 77 (suppl.): 264 (abstract only, in Japanese). [Google Scholar]
- 43.Yoshida Y, Shiota T, Yamada M, Matsumoto Y, Okabayashi K, Yoshikawa H, Takino T, Nakagawa Y, Yokota S. Report of an imported case of Dipetalonema perstans in Japan. Southeast Asian J Trop Med Pub Hlth 1983; 14: 341-344 [PubMed] [Google Scholar]
- 44.Hioki A, Kasuya S, Ito A, Ohtomo H. Status of imported parasitic infection in 34 cases and the problems in their diagnosis and treatment. Acta scholae medicinalis universitatis in Gifu 1986; 34: 1223-1228 (in Japanese). [Google Scholar]
- 45.Iiyama T, Sekine K, Itoh I, Kuwana B, Kobayashi M. A case of filariasis experienced at our clinic*. Jpn J Med Technol 2000; 49: 578 (abstract only, in Japanese). [Google Scholar]
- 46.Yoshimura H, Kondo K, Akao N, Ohnishi Y, Ikado S, Miyawaki H. An onchocercal nodule found in a Japanese infected in Africa. Japan J Trop Med Hyg 1983; 11: 243-248 [Google Scholar]
- 47.Oyamada Y, Funae O, Kamegaya Y, Soejima K, Nakamura H, Mori S, Yamaguchi K, Kanazawa M, Okusawa E, Yamasawa F. A case of tropical eosinophilia associated wit pleural effusion. Jpn J Thoracic Dis 1995; 33: 451-455 (in Japanese). [PubMed] [Google Scholar]
- 48.Hayashi K, Horiba M, Shindou J, Sumida T, Takekoshi A. Tropical eosinophilia in a man from Sri Lanka. Jpn J Thoracic Dis 1996; 34: 1411-1415 (in Japanese). [PubMed] [Google Scholar]
- 49.Hashimoto H, Murakami I, Fojiwara S, Takayasu S, Takaoka H, Uga S, Akao N, Kondo K, Yoshimura H. A human case of zoonotic onchocerciasis in Japan. J Dermatol 1990; 17: 52-55 [DOI] [PubMed] [Google Scholar]
- 50.Beaver PC, Yoshimura H, Takayasu S, Hashimoto H, Little MD. Zoonotic Onchocerca in a Japanese child. Am J Trop Med Hyg 1989; 40: 298-300 [DOI] [PubMed] [Google Scholar]
- 51.Takaoka H, Bain O, Tajima S, Kashima K, Nakayama I, Korenaga M, Aoki C, Otsuka Y. Second case of zoonotic Onchocerca infection in a resident of Oita in Japan. Parasite 1996; 3: 179-182 [DOI] [PubMed] [Google Scholar]
- 52.Takaoka H, Bain O, Uni S, Korenaga M, Tada K, Ichikawa H, Otsuka Y, Eshita Y. Human infection with Onchocerca dewittei japonica. a parasite from wild boar in Oita Japan. Parasite 2001; 8: 261-263 [PubMed] [Google Scholar]
- 53.Korenaga M, Tada I, Mimori T, Sakamoto M, Lujan TA, Zea FGE, Castro JC, Yarzabal L. Enzyme-linked immunosorbent assay (ELISA) in the detection of IgG antibodies in onchocerciasis using blood collected on filter paper. Jpn J Parasitol 1983; 32: 347-355 [Google Scholar]