

Abstract
The fasting of Ramadan is observed by a large proportion of Muslims with diabetes. Recommendations for the management of diabetes during Ramadan were last published in 2005 by the American Diabetes Association. Several studies in this field have since been published, some addressing the use of new pharmacological agents in managing diabetes during Ramadan. The incritin memetics are potentially safe during Ramadan; the DPP4 inhibitors vildagliptin and sitagliptin provide an effective and safe therapeutic option, administered either alone or in combination with metformin or sulfonylureas. There are no published studies on the use of GLP-1 receptor agonists during Ramadan. Among the sulfonylureas, gliclazide MR (modified release) and glimepride can be safely used during Ramadan, but glibenclamide should be avoided due to the associated risk of hypoglycemia. In selected patients with type 1 and type 2 diabetes, the long-acting insulin analogues glargine and detemir, as well as the premixed insulin analogues, can be used with minimal risk of metabolic derangement or hypoglycemia; the risk is higher in type 1 diabetes. Insulin pumps can potentially empower patients with diabetes and enable safe fasting during the month of Ramadan. Further clinical trials are needed to evaluate the safety and efficacy of new antidiabetic agents and new diabetes-related technologies during Ramadan.
It is estimated that around 40 to 50 million individuals with diabetes worldwide fast during Ramadan.1 During fasting, Muslims abstain from food and drinks (including oral medication) from dawn to dusk. The population-based Epidemiology of Diabetes and Ramadan, 1422/2001 (EPIDIAR), study conducted in 13 Islamic countries showed that 43% of patients with type 1 diabetes and 79% of patients with type 2 diabetes fast during Ramadan.1
In non-diabetic individuals, fasting is associated with improvement in several hemostatic risk markers for cardiovascular disease, including reduction in plasma triglyceride and plasma LDL-cholesterol level, as well as improvement in insulin sensitivity, leptin, adiponectin and HDL cholesterol.2–5 Ramadan fasting in non-diabetic individuals is also associated with reduction in plasma homocysteine, D-dimer level, C-reactive protein (CRP) and IL-6 and fibrinogen.6,7 Similar beneficial effects of fasting have been reported in diabetic individuals. In a cohort of 276 obese women with type 2 diabetes, fasting during Ramadan was associated with decreased total calorie intake, weight reduction8 and improvement in glucose homeostasis.9 However, another study failed to demonstrate a major effect on energy intake.10 Hypoglycemia and, to a lesser extent, hyperglycemia and diabetic ketoacidosis remain serious risks necessitating careful evaluation before contemplating fasting.
Recently, glycemic therapeutic options for diabetes have expanded, with the introduction of new therapeutic agents and new technologies; some of these have been used during Ramadan and have shown potential therapeutic benefit. In this review, we provide an update on the use of glycemic therapeutics during Ramadan, including the new glycemic options for both type 2 and type 1 diabetes.
Type 2 Diabetes and Ramadan
Since the publication of the EPIDIAR study in 2004,1 several reports on the safely, benefits and challenges of fasting in type 2 diabetes have been published.8–10 Individual assessment of the situation for each patient is essential, together with patient education and appropriate adjustment of antidiabetic therapy.10
Sulfonylureas
Zargar et al used gliclazide MR 60 mg as monotherapy during the month of Ramadan in 136 non-obese males [average BMI was 23 kg/m2] with type 2 diabetes. Their data showed no alteration of previously well-controlled diabetes, no weight gain and, importantly, few hypoglycemic events.11 M’guil et al reported similar findings with gliclazide MR during Ramadan.10 The GUIDE study (a double-blind comparison of once-daily gliclazide MR and glimepiride in type 2 diabetic patients, excluding patients who fasted) showed that gliclazide MR is at least as effective as glimepiride, either as monotherapy or in combination. In fact, gliclazide MR was significantly better, demonstrating approximately 50% fewer confirmed hypoglycemic episodes in comparison with glimepiride.12 The authors of Recommendations For Management Of Diabetes during Ramadan", published in 2005, recommended the use of gliclazide MR and to exercise caution with other sulfonylureas (chlorpropamide absolutely contraindicated during Ramadan due to risk of prolonged and unpredictable hypoglycemia).13 However, three studies have shown glimepiride to be effective and safe during Ramadan.14–16
Incritins
In recent years, new therapeutic options for treatment of type 2 diabetes have been introduced. Glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide are incritins secreted from enteroendocrine cells postprandially, in part, to regulate glucose homeostasis. Dysregulation of these hormones is evident in type 2 diabetes mellitus. Four new drugs — exenatide, liraglutide (GLP-1 memetics), sitagliptin, vildagliptin [dipeptidyl peptidase (DPP-4, inhibitor)] have been approved by regulatory agencies for treating type 2 diabetes.
GLP1 memetics
Exenatide and liraglutide injections have a potential for safe use during Ramadan, primarily because reduced or negligible risk of hypoglycemia. As yet, there are no published reports on the use of these agents during Ramadan. Three-year follow-up data on exenatide (2 injections per day) showed a sustained weight loss and decreased glycosylated hemoglobin (HbA1c), by 1%. Nausea and vomiting are common.17 Results from studies on liraglutide (1 injection a day) showed very few episodes of hypoglycemia, less nausea, better glycemic control (1.8% reduction in HbA1c) and weight loss of around 3 kg. In the LEAD-6 trial, liraglutide once a day provided greater improvements in glycemic control than did exenatide twice a day, and, importantly, with less incidence of hypoglycemia.18 Also, liraglutide versus glimepiride monotherapy for type 2 diabetes showed that the liraglutide group achieved better glycemic control with fewer episodes of hypoglycemica.19 Studies investigating the use of these agents during Ramadan would be welcome.
DPP-4 inhibitors
The DPP-4 inhibitors sitagliptin and vildagliptin are new oral hypoglycemic agents. In a 24-week study, sitagliptin as monotherapy reduced HbA1c by 0.6% to 0.8%. It reduced HbA1c by up to 1.8% when used in combination with metformin, while vildagliptin monotherapy lowered HbA1c by 1.0% to 1.4% after 24 weeks.17
In a recent report from northwest London,52 Muslim diabetic individuals already on 2 g daily metformin were studied during Ramadan. They were randomized to the addition of either vildagliptin 50 mg daily (26 individuals) or gliclazide 160 mg twice daily (26 individuals). At least one hypoglycemic event (defined as blood glucose <3.5 mmol/L with or without symptoms) was recorded in 2 patients receiving vildagliptin and 16 patients receiving gliclazide.20 Both gliclazide and vildagliptin were associated with similar reductions in HbA1c and a small, but insignificant, increase in weight. Thus the DPP-4 inhibitors provide a safe alternative therapeutic option during Ramadan.
Older oral agents
Other antidiabetic medicines have also be used during Ramadan, including repaglinide, acarbose metformin, glitazone and insulin (lispro and glargine).10–20 Al-Arouj et al recommended the use of glitazone without changing the dose; while for metformin, two-thirds of the dose was to be taken before sunset meal and the other third with pre-dawn meal.16 Bakiner et al reported that meal-time repaglinide three times a day plus single-dose insulin glargine was safe (no hypoglycemia, no change in glycemic control or weight gain) for low-risk type 2 diabetic individuals who insisted on fasting during Ramadan.21
Cesur et al compared the effects of glimepiride (n=21), repaglinide (n=18) and insulin glargine (n=10) in type 2 diabetic individuals during Ramadan; 16 non-fasting type 2 diabetic individuals matched for age, sex and body mass index were also included. Fasting blood glucose (FBG), postprandial blood glucose (PBG), HbA1c and fructosamine, as well as lipid metabolism, were evaluated at three points in time—pre-Ramadan, immediate post-Ramadan and 1 month post-Ramadan. There was no significant change in FBG, PBG and HbA1c in fasting diabetic individuals from pre-Ramadan to neither at immediate post-Ramadan nor 1 month post-Ramadan times. However, PBG was significantly higher in non-fasting diabetic control subjects at immediate post-Ramadan and 1 month post-Ramadan times (P<.05 and P<.001, respectively). The risk of hypoglycemia did not differ between fasting and non-fasting diabetics. There was no significant difference between the three therapies regarding glucose metabolism and rate of hypoglycemia.22
Belkhadir claimed that glibenclamide (Daonil) is effective and safe for type 2 diabetes during Ramadan.23 However, Mafauzy showed that repaglinide was associated with better glycemic control and a lower frequency of hypoglycemia in comparison with glibenclamide.24 While metformin, glitazones, repaglinide are safe options, the increased risk of hypoglycemia makes glibenclamide unattractive as a therapeutic agent during Ramadan.
Insulins and insulin regimens
Insulin can be safely used in type 2 diabetic individuals. Twice daily premixed insulins such as lispro mix 25/75 (25% insulin lispro and 75% neutral protamine lispro) and human insulin 30/70 have been used safely during Ramadan.25 It is recommended that the usual morning dose of this regimen be used with the sunset meal and half the usual evening dose be used with the pre-dawn meal.16 Insulin glargine is also effective and safe during Ramadan and can be given as single injection at 10 PM with or without mealtime short-acting analogues or other oral antidiabetic medication (repaglinide or metformin).21
Type 1 Diabetes and Ramadan
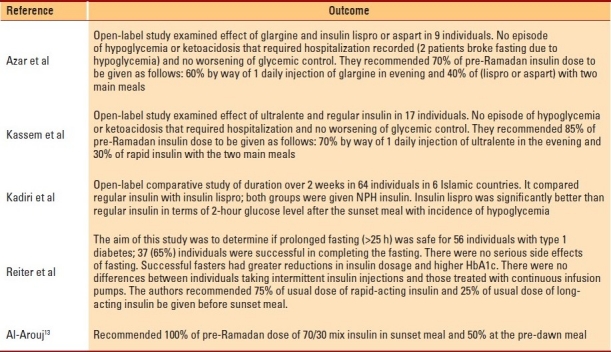
Fasting during Ramadan has been uniformly discouraged by the medical profession for individuals with type 1 diabetes (especially those with poor diabetes control, frequent and severe hypoglycemia and those with brittle diabetes). However, according to the Epidemiology of Diabetes and Ramadan study, 43% of individuals with type 1 diabetes do fast.1 Due to the long hours of fasting, the main concern is the associated increased risk of hypoglycemia, hyperglycemia and ketoacidosis.1,12 Patients with poorly controlled type 1 diabetes, those with unstable plasma glucose and those with significant complications are at higher risk and should be advised to avoid fasting. Furthermore, for individuals with type 1 diabetes, basal bolus insulin may be associated with a lower risk of hypoglycemia in comparison with conventional twice-daily insulin regime. Importantly, insulin glargine used as the basal insulin resulted in excellent control in 15 nonexercising individuals who fasted for 18 hours, with mean plasma glucose of 5.1 to 6.9 mmol/L during fasting.26 Al-Arouji et al recommended the use of 1 injection of glargine or 2 injections of detemir along with a pre-meal rapid-acting insulin analogue. Studies on the use of different types of insulin regimens in type 1 diabetes during Ramadan were recently reviewed by Kobeissy et al;27 a summary is provided in Table 1.
Table 1.
Different regimens of insulin therapy for type 1 diabetes during Ramadan.
Insulin pump
In a recent small study on five Saudi adolescents with type 1 diabetes (age range, 15-19 years; mean duration of diabetes, 7 years), the use of subcutaneous insulin infusion (CSII) during Ramadan was associated with improvement in glycemic control and less hypoglycemia in comparison with conventional insulin therapy.28 The insulin pump has the potential to be a safe and flexible method for insulin delivery during Ramadan for selected patients. Further larger studies on the use of insulin pump during Ramadan are needed. The insulin pump is currently not used widely due to associated high cost.
Glycemic management options during Ramadan
Careful and individual evaluation and open discussions are key measures for ensuring patient safety during the fasting of Ramadan. The physician is duty-bound to support diabetic individuals before and through Ramadan to enable safe fasting. It is also the responsibility of the physician to emphasize the fact that according to the principle of Fiqh (Islamic jurisprudence), exemption from fasting is allowed if in the opinion of a trusted doctor, fasting is expected to lead to “worsening of the disease or delay in healing.”10 An integrated algorithm addressing management of type 1 and type 2 diabetes during Ramadan is provided in Figure 1.
Figure 1.
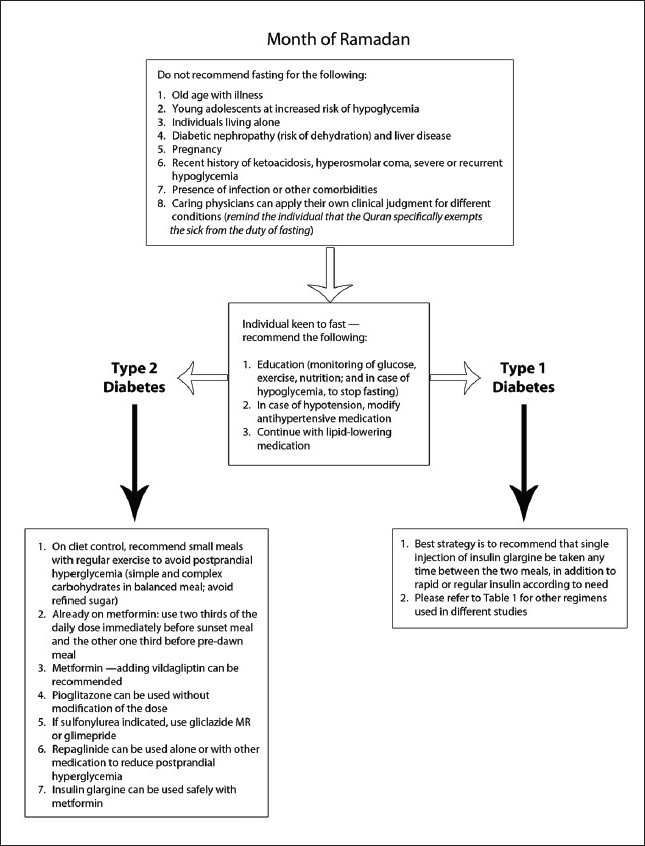
Integrated algorithm addressing management of type 1 and type 2 diabetes during Ramadan
Conclusion
In recent years, exciting new therapies and technologies have positively influenced the management of diabetes. Some of these have been investigated for use during the fasting of Ramadan. The DPP-4 inhibitors vildagliptin and sitagliptin provide an effective and safe therapeutic option during Ramadan, either alone or in combination with metformin or sulfonylureas. The incritin memetics liraglutide and exenatide are potentially safe therapies during Ramadan, but as yet there are no reports of using them during Ramadan. The newer sulfonylureas gliclazide MR and glimepride can be safely used during Ramadan, but glibenclamide should be avoided because of the increased risk of hypoglycemia. Administration of the long-acting insulins glargine and detemir; or the premixed insulin analogues has shown potential benefit in selected patients with type 1 and type 2 diabetes, with a guarded risk of hypoglycemia. The insulin pump can potentially empower patients with diabetes and enable safe fasting during the month of Ramadan. Clinical trials are needed in order to further evaluate the safety and efficacy of new hypoglycemic agents and new diabetes-treating technologies during Ramadan.
Footnotes
The authors received no funding and report no conflict of interest.
REFERENCES
- 1.Salti I, Benard E, Detournay B, Bianchi-Biscay M, Le BC, Voinet C, et al. A population-based study of diabetes and its characteristics during the fasting month of Ramadan in 13 countries: results of the epidemiology of diabetes and Ramadan 1422/2001 (EPIDIAR) study. Diabetes Care. 2004;27:2306–11. doi: 10.2337/diacare.27.10.2306. [DOI] [PubMed] [Google Scholar]
- 2.Shariatpanahi ZV, Shariatpanahi MV, Shahbazi S, Hossaini A, Abadi A. Effect of Ramadan fasting on some indices of insulin resistance and components of the metabolic syndrome in healthy male adults. Br J Nutr. 2008;100:147–51. doi: 10.1017/S000711450787231X. [DOI] [PubMed] [Google Scholar]
- 3.Bouhlel E, Denguezli M, Zaouali M, Tabka Z, Shephard RJ. Ramadan fastings effect on plasma leptin, adiponectin concentrations, and body composition in trained young men. Int J Sport Nutr Exerc Metab. 2008;18:617–27. doi: 10.1123/ijsnem.18.6.617. [DOI] [PubMed] [Google Scholar]
- 4.Haghdoost AA, Poorranjbar M. The interaction between physical activity and fasting on the serum lipid profile during Ramadan. Singapore Med J. 2009;50:897–901. [PubMed] [Google Scholar]
- 5.Lamri-Senhadji MY, El KB, Belleville J, Bouchenak M. Assessment of dietary consumption and time-course of changes in serum lipids and lipoproteins before, during and after Ramadan in young Algerian adults. Singapore Med J. 2009;50:288–94. [PubMed] [Google Scholar]
- 6.Aksungar FB, Eren A, Ure S, Teskin O, Ates G. Effects of intermittent fasting on serum lipid levels, coagulation status and plasma homocysteine levels. Ann Nutr Metab. 2005;49:77–82. doi: 10.1159/000084739. [DOI] [PubMed] [Google Scholar]
- 7.Aksungar FB, Topkaya AE, Akyildiz M. Interleukin-6, C-reactive protein and biochemical parameters during prolonged intermittent fasting. Ann Nutr Metab. 2007;51:88–95. doi: 10.1159/000100954. [DOI] [PubMed] [Google Scholar]
- 8.Khaled BM, Belbraouet S. Effect of Ramadan fasting on anthropometric parameters and food consumption in 276 type 2 diabetic obese women. Int J Diabetes Dev Ctries. 2009;29:62–8. doi: 10.4103/0973-3930.53122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Khaled BM, Belbraouet S. Ramadan fasting diet entailed a lipid metabolic disorder among type 2 diabetic obese women. Am J Appl Sci. 2009;6:471–7. [Google Scholar]
- 10.Suliman M, Abdu T, Elhadd T, Ibrahim S, Ahmed MH, Malik R. Diabetes and fasting in Ramadan: Can we provide evidence-based advice to patients? Sudan Med J. 2010;46(1):4–14. [Google Scholar]
- 11.Zargar AH, Siraj M, Jawa AA, Hasan M, Mahtab H. Maintenance of glycaemic control with the evening administration of a long acting sulphonylurea in male type 2 diabetic patients undertaking the Ramadan fast. Int J Clin Pract. 2010;64:1090–4. doi: 10.1111/j.1742-1241.2009.02262.x. [DOI] [PubMed] [Google Scholar]
- 12.Schernthaner G, Grimaldi A, Di MU, Drzewoski J, Kempler P, Kvapil M, et al. GUIDE study: double-blind comparison of once-daily gliclazide MR and glimepiride in type 2 diabetic patients. Eur J Clin Invest. 2004;34:535–42. doi: 10.1111/j.1365-2362.2004.01381.x. [DOI] [PubMed] [Google Scholar]
- 13.Al-Arouj M, Bouguerra R, Buse J, Hafez S, Hassanein M, Ibrahim MA, et al. Recommendations for management of diabetes during Ramadan. Diabetes Care. 2005;28:2305–11. doi: 10.2337/diacare.28.9.2305. [DOI] [PubMed] [Google Scholar]
- 14.Glimepiride in Ramadan (GLIRA) Study Group. The efficacy and safety of glimepiride in the management of type 2 diabetes in Muslim patients during Ramadan. Diabetes Care. 2005;28:421–2. doi: 10.2337/diacare.28.2.421. [DOI] [PubMed] [Google Scholar]
- 15.Anwar A, Azmi KN, Hamidon BB, Khalid BA. An open label comparative study of glimepiride versus repaglinide in type 2 diabetes mellitus Muslim subjects during the month of Ramadan. Med J Malaysia. 2006;61:28–35. [PubMed] [Google Scholar]
- 16.Sari R, Balci MK, Akbas SH, Avci B. The effects of diet, sulfonylurea, and Repaglinide therapy on clinical and metabolic parameters in type 2 diabetic patients during Ramadan. Endocr Res. 2004;30:169–77. doi: 10.1081/erc-200027375. [DOI] [PubMed] [Google Scholar]
- 17.Chia CW, Egan JM. Incretin-based therapies in type 2 diabetes mellitus. J Clin Endocrinol Metab. 2008;93:3703–16. doi: 10.1210/jc.2007-2109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Buse JB, Rosenstock J, Sesti G, Schmidt WE, Montanya E, Brett JH, et al. Liraglutide once a day versus exenatide twice a day for type 2 diabetes: a 26-week randomised, parallel-group, multinational, open-label trial (LEAD-6) Lancet. 2009;374:39–47. doi: 10.1016/S0140-6736(09)60659-0. [DOI] [PubMed] [Google Scholar]
- 19.Garber A, Henry R, Ratner R, Garcia-Hernandez PA, Rodriguez-Pattzi H, Olvera-Alvarez I, et al. Liraglutide versus glimepiride monotherapy for type 2 diabetes (LEAD-3 Mono): a randomised, 52-week, phase III, double-blind, parallel-treatment trial. Lancet. 2009;373:473–81. doi: 10.1016/S0140-6736(08)61246-5. [DOI] [PubMed] [Google Scholar]
- 20.Devendra D, Gohel B, Bravis V, Hui E, Salih S, Mehar S, et al. Vildagliptin therapy and hypoglycaemia in Muslim type 2 diabetes patients during Ramadan. Int J Clin Pract. 2009;63:1446–50. doi: 10.1111/j.1742-1241.2009.02171.x. [DOI] [PubMed] [Google Scholar]
- 21.Bakiner O, Ertorer ME, Bozkirli E, Tutuncu NB, Demirag NG. Repaglinide plus single-dose insulin glargine: a safe regimen for low-risk type 2 diabetic patients who insist on fasting in Ramadan. Acta Diabetol. 2009;46:63–5. doi: 10.1007/s00592-008-0062-7. [DOI] [PubMed] [Google Scholar]
- 22.Cesur M, Corapcioglu D, Gursoy A, Gonen S, Ozduman M, Emral R, et al. A comparison of glycemic effects of glimepiride, repaglinide, and insulin glargine in type 2 diabetes mellitus during Ramadan fasting. Diabetes Res Clin Pract. 2007;75:141–7. doi: 10.1016/j.diabres.2006.05.012. [DOI] [PubMed] [Google Scholar]
- 23.Belkhadir J, el GH, Klocker N, Mikou A, Nasciri M, Sabri M. Muslims with non-insulin dependent diabetes fasting during Ramadan: treatment with glibenclamide. BMJ. 1993;307:292–5. doi: 10.1136/bmj.307.6899.292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Mafauzy M. Repaglinide versus glibenclamide treatment of Type 2 diabetes during Ramadan fasting. Diabetes Res Clin Pract. 2002;58:45–53. doi: 10.1016/s0168-8227(02)00104-3. [DOI] [PubMed] [Google Scholar]
- 25.Mattoo V, Milicevic Z, Malone JK, Schwarzenhofer M, Ekangaki A, Levitt LK, et al. A comparison of insulin lispro Mix25 and human insulin 30/70 in the treatment of type 2 diabetes during Ramadan. Diabetes Res Clin Pract. 2003;59:137–43. doi: 10.1016/s0168-8227(02)00202-4. [DOI] [PubMed] [Google Scholar]
- 26.Mucha GT, Merkel S, Thomas W, Bantle JP. Fasting and insulin glargine in individuals with type 1 diabetes. Diabetes Care. 2004;27:1209–10. doi: 10.2337/diacare.27.5.1209. [DOI] [PubMed] [Google Scholar]
- 27.Kobeissy A, Zantout MS, Azar ST. Suggested insulin regimens for patients with type 1 diabetes mellitus who wish to fast during the month of Ramadan. Clin Ther. 2008;30:1408–15. doi: 10.1016/j.clinthera.2008.08.007. [DOI] [PubMed] [Google Scholar]
- 28.Bin-Abbas BS. Insulin pump therapy during Ramadan fasting in type 1 diabetic adolescents. Ann Saudi Med. 2008;28:305–6. doi: 10.5144/0256-4947.2008.305. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Azar ST, Khairallah WG, Merheb MT, Zantout MS, Fliti F. Insulin therapy during Ramadan fast for patients with type 1 diabetes mellitus. J Med Liban. 2008;56:46. [PubMed] [Google Scholar]
- 30.Kassem HS, Zantout MS, Azar ST. Insulin therapy during Ramadan fast for Type 1 diabetes patients. J Endocrinol Invest. 2005;28:802–5. doi: 10.1007/BF03347569. [DOI] [PubMed] [Google Scholar]
- 31.Kadiri A, Al-Nakhi A, El-Ghazali S, Jabbar A, Al AM, Akram J, et al. Treatment of type 1 diabetes with insulin lispro during Ramadan. Diabetes Metab. 2001;27:482–6. [PubMed] [Google Scholar]
- 32.Reiter J, Wexler ID, Shehadeh N, Tzur A, Zangen D. Type 1 diabetes and prolonged fasting. Diabet Med. 2007;24:436–9. doi: 10.1111/j.1464-5491.2007.02098.x. [DOI] [PubMed] [Google Scholar]