

Sir,
Prescribing drugs in elderly patients entails risks due to physiological alterations in drug handling as well as multiple prescriptions and co-morbidities. Inappropriate prescribing (IP) is a major public health problem and screening for IP is highly desirable since detection and correction are easy and worthwhile. The updated Beers criteria[1] are a set of explicit criteria widely used to detect Potentially Inappropriate Medication (PIM) in elderly. As the elderly population continues to rise, the need for improving the healthcare of these patients should be a priority of all nations. Most developed nations have formularies to provide therapeutic guidelines to prescribers and enhance rational use of drugs.[2] Unfortunately, in India, there is no updated National Formulary of India (NFI). The 3rd NFI was published in 1979 and is largely defunct, while the 4th NFI is to be out yet. In such scenario, most prescribers look upon other sources of drug information like Monthly Index of Medical Specialities (MIMS ), Current Index of Medical specialities (CIMS), Drugs Index, Drugs Today etc., for guidance on indication, dosage, contraindications, and other clinical aspects of drug use. These proprietary formularies may have shortcomings in terms of authenticity, accuracy of drug information in general, and a specific age group of patients, in particular.
This study was done to assess the appropriateness of information on prescribing in elderly patients given in a popular formulary, CIMS-India (January-April 2010), using the updated Beers criteria (2003)[1]. First described in 1991,[3] Beers criteria of PIM were a list of 30 drugs to be avoided in elderly population regardless of diagnosis. These are defined as medication in which risk of use in elderly substantially outweighs the benefit. The updated Beers list of 2003 has 48 drugs.
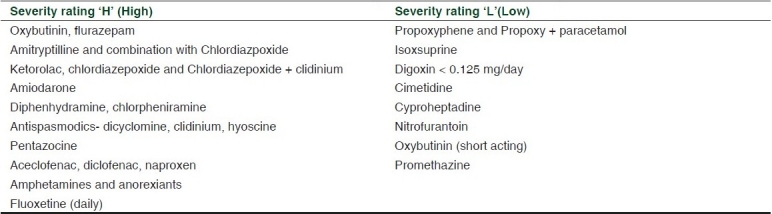
The study results showed that among 48 drugs included in Beers list of PIM in elderly, 8 drugs namely guanthedine, guanadrel, tripelenamine, trimethiobenzamide, chlorpropamide, ethacynic acid, meperidine, and meprobamate were not available in India. Out of remaining 40 drugs/drug classes of PIM, appropriate information was given for 4/40 (10%) drugs and included short-acting benzodiazepines (lorazepam ≤ 3 mg/day, oxazepam ≤ 60 mg/day temazepam ≤ 15 mg/day, alprazolam ≤ 2 mg/day), reserpine < 0.25 mg/day, skeletal muscle relaxants (methacarbomol and carisoprodol- half adult dose), and methyldopa (half adult dose). Further, there was no information or note of caution regarding the use of 14/40 (35%) which could pose increased risk if prescribed to elderly patients. These included indomethacin (produces most central nervous system effects of all nonsteroidal anti-inflammatory drugs, doxepin (strong anticholinergic and sedating properties), disopyramide (most potent negative inotrope and may induce heart failure in elderly patients, also strongly anticholinergic), ticlopidine (no better than aspirin), cyclandelate (lack of efficacy), doxazocin, clonidine, short -acting nifedipine and dipyridamole(potential for hypotension, dry mouth, constipation), chlorzoxazone (poorly tolerated in elderly, effectiveness doubtful), thioridazine, ergotamine, estrogens and ferrous sulphate > 325 mg/day. Information regarding remaining 22/40 (55%) drugs was ambiguous as these were assigned a “special precaution (S/P)”, for use in elderly [Table 1]. However, what “S/Ps” were to be taken was not mentioned anywhere. This implies that the prescribers would have to look for more information on these drugs elsewhere which is often tedious and time consuming. The clinical utility of the formulary in such instances thus seems limited, leaving the prescribers in a quandary, regarding the use of these drugs in elderly patients. Further analysis showed that 13/22 (59%) drugs were rated as having “high” severity in Beers criteria. This group of drugs could well contribute to large number of PIM in elderly patients. Studies across Europe have showed percentage of approved drugs for elderly patients in national formularies range from 32% in Norway to 71% in Italy.[4] This study estimates this figure as only 10% in the Indian formulary.
Table 1.
Drugs labeled with a S/P note for elderly and severity grade as per Beers criteria[1]
This study highlights the inadequacy of the Indian formulary in context of geriatric prescribing. There is an imminent need of a national formulary with due focus on guidelines for geriatric prescribing. This can justify the nation's commitment to healthcare of this frail but expanding group of senior citizens.
REFERENCES
- 1.Fick DM, Cooper JW, Wade WE, Waller JL, Maclean JR, Beers MH. Updating the Beers Criteria for potentially inappropriate medication use in older adults: Results of a US consensus panel of experts. Arch Intern Med. 2003;163:2716–24. doi: 10.1001/archinte.163.22.2716. [DOI] [PubMed] [Google Scholar]
- 2.Fiolova D, Onder G. Medication errors in elderly people: Contributing factors and future perspectives. Br J Clin Pharmacol. 2009;67:641–45. doi: 10.1111/j.1365-2125.2009.03419.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Beers MH, Ouslander JG, Rollingher I, Reuben DB, Brooks J, Beck JC. Explicit criteria for determining inappropriate medication in nursing home residents. Arch Intern Med. 1991;151:1825–32. [PubMed] [Google Scholar]
- 4.Fialová D, Topinková E, Gambassi G, Finne-Soveri H, Jónsson PV, Carpenter I, et al. AdHOC project research group.Potentially Inappropriate Medication use in elderly home care patients in Europe. JAMA. 2005;293:1348–58. doi: 10.1001/jama.293.11.1348. [DOI] [PubMed] [Google Scholar]