

Abstract
Background and Objectives:
Special concern is focused on the nutritional status of adolescent girls in order to avoid future health problems. The aim of this study was to determine the change in body mass index (BMI) among adolescent Saudi girls living in Al-Khobar between 1997 and 2007.
Materials and Methods:
A cross-sectional sample of adolescent Saudi girls, 15–19-years-old, living in Al-Khobar, Saudi Arabia, was analyzed through two data sets. The first data set (n = 400) was collected in 1997 and the second (n = 321) was collected in 2007. Both data sets used the same sampling method. Anthropometric measurements were made and the BMI was used to determine participants’ nutritional status. Statistical analysis was performed.
Results:
There was an increase in the median weight of Saudi adolescent girls from 1997 to 2007, but the change was not statistically significant. There was a statistically significant change, however, in adolescent girls’ height during the 10-year interval. Using BMI to determine the nutritional status of the sample, no statistically significant difference was found. Overweight and obesity remain prevalent in about 30% of the adolescent girls, and about 3.5% of the girls in both sets were underweight.
Conclusions:
This study concluded that there was no change in BMI among Saudi adolescent girls living in Al-Khobar during the 10-year span. Underweight is of low prevalence, and overweight and obesity are the critical nutritional problems that are faced by this population. Further research using time span comparisons is important to assess changes in maladaptive overweight and obesity.
Keywords: Adolescent girls, body mass index, obesity, overweight, Saudi Arabia
INTRODUCTION
With an eye on avoiding future health problems, public health authorities continue to cite overweight and obesity among children and adolescents as a leading concern in both developed[1–3] and developing countries.[4–6] Underweight is also an issue as it too becomes a health problem faced by some developing countries.[7–9]
The rapid rise in the prevalence of obesity and overweight among children portends a future epidemic of obesity-related medical conditions. These conditions include cardiovascular disease, type 2 diabetes and degenerative joint disease.[10] Overweight and obese children are likely to remain obese into adulthood[3,11] and have a shorter life span than their parents.[12]
Similar to other places throughout the world, Saudi Arabia faces the problem of obesity and overweight in children and adolescents.[4,13] There are limited time span studies indicating rising obesity levels among adolescent Saudi boys.[14,15] The prevalence of obesity among adolescent girls has been reported in many studies in Saudi Arabia[16–19] but, in our opinion, there has not been a comparative study. Therefore, the aim of the present study was to determine the change in body mass index (BMI) among adolescent Saudi girls living in Al-Khobar between 1997 and 2007. Two surveys were conducted during the time period to shed further light on any trends evidenced.
MATERIALS AND METHODS
In this study, two sets of data from Saudi adolescent girls, 15–19-years-old, living in Al-Khobar, Saudi Arabia, were analyzed. The first set (n = 400) was conducted in 1997. We performed a study titled “Nutritional status of adolescent girls in the Eastern Province of Saudi Arabia” that has been published elsewhere.[16] That study was used as the first data set in the present study. The second data set (n = 321) was collected in 2007. The sample was taken from the same geographic areas to ensure a truly comparable group with no sociodemographic differences. Both data sets used the same sampling methods and data collection procedures. A multistage random sample was drawn from secondary schools in three geographical areas in Al-Khobar city. Two schools were selected using a random method from each area. One class from each grade level was then selected from each school, and all the girls in the selected classes were included in the survey.
Because the original study was conducted with a larger age range, girls younger than 15 years and older than 19 years were excluded from the current analysis (they constituted only 5.7%). This provided a good age range matching between the two data sets.
Anthropometric measurements were made in both the studies. Height was measured to the nearest 0.1 cm using a measuring rode with sliding head piece attached to the scale. Weight was measured without shoes to the nearest 0.5 kg.[20] The scale was zeroed before each session and was frequently calibrated with a known weight.
The BMI (weight [kg]/height [m]2) was used to determine participants’ nutritional status. Because the National Health and Nutrition Examination Survey 1 (NHANES1) reference data[21] was used in the first study,[16] it was also used in the second data set. The girls were considered underweight with BMI less than 5 percentile of reference data, while normal girls were those with BMI ≥5 and <85 percentile. Overweight was defined as a BMI of ≥85th percentile but <95th percentile and obesity was defined as a BMI of ≥95th percentile.
The mean, median and standard deviation of weight, height and BMI were calculated. Recent Saudi growth charts were also used for further comparison.[22]
Statistical analysis was performed using SPSS version 15 software. Comparisons for the values of BMI and the percentages of obese, overweight, normal and underweight girls were taken from the first set (1997) and the second set (2007). Data were reported as means and standard deviations or as percentages. The Student t-test was used for comparing the two studies. Differences between anthropometric data were considered significant when P <0.05. Permission to conduct each study was sought from the Ministry of Education in the Eastern Province, the General Directorates of Female Education and School Health Services for females in Al-Khobar.
RESULTS
Comparisons of the height and weight of adolescent Saudi girls with the National Centre for Health Statistics (NCHS) standard show that the median height fluctuated between the 50th and 10th percentiles of the standard. The median weight in both studies (1997 and 2007) fell between the 75th and 50th percentiles of reference data. When recent Saudi reference growth charts were consulted, the same results were found for weight (between the 75th and 50th percentiles), but height fluctuated between the 50th and 75th percentiles.
Table 1 shows the distribution of the mean, standard deviation and median for weight, height and BMI from the 1997 and 2007 data sets. There was an increase in the median weight in kilograms relative to age group in the 2007 samples. Although there was an increase in participant weight, the change was not statistically significant, as shown in Table 2, in which the mean values for anthropometric parameters (weight, height and BMI) from the two data sets are displayed.
Table 1.
Mean, standard deviation and median for weight, height and body mass index by age of Saudi adolescent girls in the two data sets, 1997 and 2007
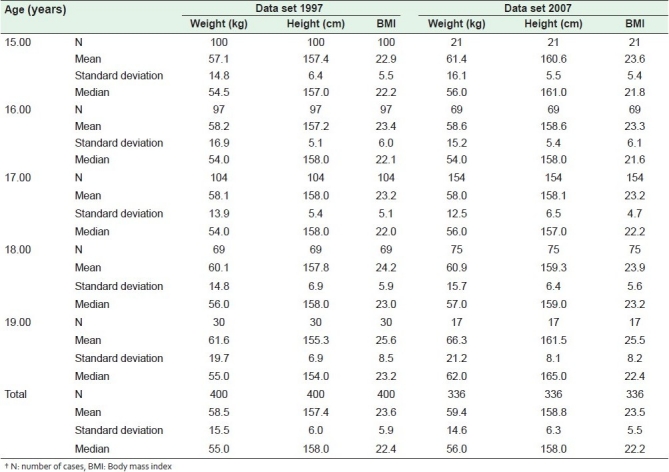
Table 2.
Comparison of anthropometric data between the first (1997) and the second (2007) samples. Data are mean ± standard deviation
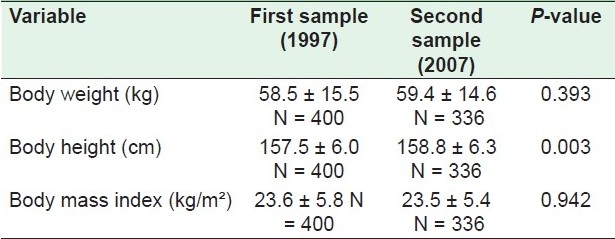
There was also an increase in the median height between the 1997 and 2007 samples. Girls in the second data set were taller compared with the first data set. Table 2 shows that there was a statistically significant change in the overall height of adolescent girls during the 10-year interval.
Table 1 further illustrates that there was a steady increase in the mean BMI of adolescent Saudi girls with increasing age in both data sets. No significant difference was noted [Table 2].
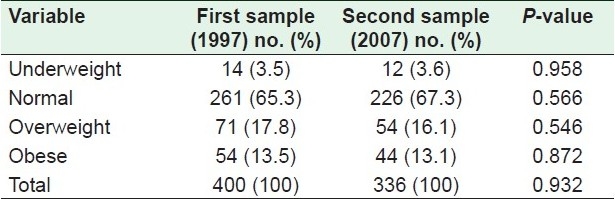
Using BMI to determine the nutritional status of Saudi adolescent girls, the results show that the proportion of girls with under-nutrition ranged from 21 to 28% between the ages of 15 and 18 years in the 1997 data set, while it was markedly more notable at ages 16 and 17 years in 2007. Both data sets show trends of an increasing proportion of overweight and obesity with increasing age from ages 15–17 years, which then decreases afterwards. During the 10-year span in both sets, about 30% of the adolescent girls were overweight or obese and about 3.5% were underweight. Table 3 shows the nutritional status relative to age in the two data sets. No statistically significant differences between the two data sets were found, as illustrated in Table 4.
Table 3.
Nutritional status of Saudi adolescent girls by age in two data sets, 1997 and 2007 (based on percentiles of body mass index)
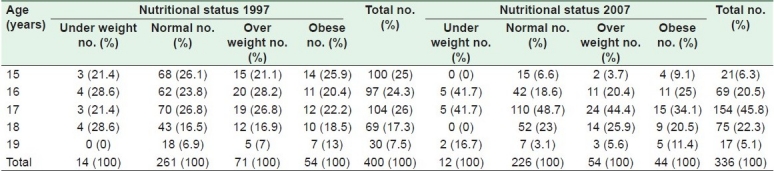
Table 4.
Nutritional status of adolescents in the two data sets
DISCUSSION
In the current analysis, Saudi adolescent girls were found to be slightly shorter than their counterparts in Western countries when using international growth charts, but that was not the case when using the recent Saudi growth charts. The growth deficits in Saudi children compared with international references may be attributable to genetic and environmental factors.[22–24]
Under-nutrition is a major health issue in developing countries. A significant finding from the current study is that only 3.5% of the Saudi adolescent girls were underweight during the 10-year span investigated. This is less than the levels reported in other developing countries.[8,9] Underweight status noted among Saudi girls by the age of 16–17 years merits further investigation. This is consistent with another study performed in India.[9]
The results of this study show another significant finding – a slight increase in the number of normal-weight girls. A steady increase in the proportion of overweight and obese girls with age observed in the current study is similar to other studies conducted in Saudi Arabia.[5,17,18,25] Interestingly, the results of this study reported that overweight and obesity, which are considered to be a serious health problem, affect about 30% of the adolescent girls across the 10-year span.
The minimal change in BMI and a trend toward a slow increase in weight among Saudi adolescent girls between 1997 and 2007 that were observed in the present study may be due to an increasing public focus on obesity and the spread of the internet, increasing girls’ awareness about their weight.[26] Our findings differ from earlier studies indicating rising trends in overweight and obesity among Saudi schoolboys.[14,15] This may be due to gender and age sample differences. The fact that girls are more aware about body appearance than boys may be attributed to gender differences.[27,28]
Education is the only course of action that health providers in girls’ school clinics can undertake, and education is not sufficient. This has been evident in other studies, which have reported that a low proportion of overweight and obese children are diagnosed as such, and that they need to be treated and need to follow the recommended guidelines for all co-morbid conditions.[3,29]
This study has highlighted the problem of the high prevalence of overweight and obesity among schoolgirls over a 10-year span that did not change. This is probably an indication of greater morbidity from diseases in the absence of a strategy in the health plan to prevent and control the problem of obesity in most Eastern Mediterranean countries.[30] We think that, to address the obesity problem in our community, a partnership should be established between different sectors. Schools, school health services, parents and health-care providers are the main domains. Foremost among the initiatives are “school-based initiatives.” Girls and their parents can be engaged through schools. Schools have been the central focus of most studies on nutrition and physical education in childhood and adolescence.[12] Health-promoting schools are one of the World Health Organization's initiatives.[30] School-based obesity prevention efforts take many forms, including the promotion of healthy foods and restriction of less-healthy foods in cafeterias as well as expanded and intensified health curricula regarding the importance of nutrition and physical activity. It is also evident that school-based overweight preventive intervention lowers the incidence of disordered weight-control behaviors in early adolescent girls.[31]
School health services should play a more effective role regarding this problem. Successful experiences in other countries dealing with this health problem should be considered. One project that school health services should start with is the implementation of electronic medical records (EMRs).[3] This will help to identify students’ nutritional status. BMI and BMI percentiles are automatically calculated in the EMRs and can be flagged when the BMI is ≥85th or ≤5th percentile. This will help to diagnose obesity. Additional methods include automatic electronic alerts or BMI report cards sent to families about adolescents’ nutritional status.[12,3] Other polices and programs that promote healthy diets and increase the levels of physical activity should be implemented, such as the “Global Strategy on Diet, Physical Activity and Health” (DPAS), which was adopted by WHO in May 2004.[32]
Families play a critical role in influencing children.[12] They should be aware of the seriousness of overweight and obesity for their children's near and distant futures. They should encourage healthy behaviors such as presenting and eating a balanced, age-appropriate diet rich in calcium and fiber, getting exercise and limiting the TV viewing and sedentary lifestyle patterns associated with obesity in children and adolescents.[33,34]
Another sector that can play a central role in helping obese children is that comprising primary health-care providers, whose thorough medical evaluation begins with an appropriate identification of overweight children. The next step is to identify current medical problems and risk factors for future disease. This evaluation may lead to additional diagnostic tests. At the end of the evaluation, the clinician will be in a position to outline the need for any immediate therapies and to begin to educate the patient and family about the risk factors for cardiovascular disease, diabetes and other obesity-related problems.[10,27]
In conclusion, this study did not find a change in BMI among Saudi adolescent girls living in Al-Khobar over a 10-year span. The low prevalence of underweight and high prevalence of overweight and obesity that were observed are regarded as a major nutritional problem. School health services should play a more effective role in caring for obese and overweight girls. Diagnosis of overweight and obesity is the first step toward treatment. Further research using time-span comparisons are important to assess changes in maladaptive overweight and obesity.
Footnotes
Source of Support: Nil
Conflict of Interest: Nil
REFERENCES
- 1.Report of WHO consultation on Obesity. Geneva, Switzerland: World Health Organization; 2000. World Health Organization. Obesity: Preventing and managing the Global Epidemic. [PubMed] [Google Scholar]
- 2.Ogden CL, Carroll MD, Curtin LR, McDowell MA, Tabak CJ, Flegal KM. Prevalence of overweight and obesity in the United States, 1999-2004. JAMA. 2006;295:1549–55. doi: 10.1001/jama.295.13.1549. [DOI] [PubMed] [Google Scholar]
- 3.Benson L, Bear H, Kaelber D. Trends in the diagnosis of overweight and obesity in children and adolescents:1999-2007. Pediatrics. 2009;123:153–8. doi: 10.1542/peds.2008-1408. [DOI] [PubMed] [Google Scholar]
- 4.Musaiger AO. Recommendation of the first conference on obesity and physical activity in the Arab Countries. Nutr Health. 2003;17:117–21. doi: 10.1177/026010600301700202. [DOI] [PubMed] [Google Scholar]
- 5.El-Hazmi MA, Warsy AS. The prevalence of obesity and overweight in 1-18 years old Saudi children. Ann Saudi Med. 2002;22:303–7. doi: 10.5144/0256-4947.2002.303. [DOI] [PubMed] [Google Scholar]
- 6.Ramachandran A, Snehalatha C, Vinitha R, Thayyil M, Kumar CK, Sheeba L, et al. Prevalence of overweight in urban Indian adolescent school children. Diabet Res Clin Pract. 2002;57:185–90. doi: 10.1016/s0168-8227(02)00056-6. [DOI] [PubMed] [Google Scholar]
- 7.Kruz KM. Adolescent nutritional status in developing countries. Proc Nutr Soc. 1996;55:321–31. [PubMed] [Google Scholar]
- 8.Monteiro CA, Benicio MH, Konno SC, Feldenheimer da Silva AC, Lovadino de Lima AC, Wolney Lisboa CondeI WL. Causes for the decline in child under-nutrition in Brazil, 1996-2007. Saúde Pública. 2009;43:1–8. doi: 10.1590/s0034-89102009000100005. [DOI] [PubMed] [Google Scholar]
- 9.Prashant K, Shaw C. Nutritional status of adolescent girls from an urban slum area in South India. Indian J Pediatr. 2009;76:501–4. doi: 10.1007/s12098-009-0077-2. [DOI] [PubMed] [Google Scholar]
- 10.Barlow SE, Dietz WH, William JK, Trowbridge FL. Medical evaluation of overweight children and adolescents: Reports from Pediatricians, Pediatric Nurse Practitioners, and Registered Dietitians. Pediatrics. 2002;110:222–8. Available from: http://www.pediatrics.org/cgi/content/full/110/1/S1/222 . [PubMed] [Google Scholar]
- 11.Freedman DS, Khan LK, Serdula MK, Dietz WH, Srinivasan SR, Berenson GS. The relation of childhood BMI to adult adiposity: The Bogalusa heart study. Pediatrics. 2005;115:22–7. doi: 10.1542/peds.2004-0220. [DOI] [PubMed] [Google Scholar]
- 12.Davis MM, Gance-Cleveland B, Hassink S, Johnson R, Paradis G, Resnicow K. Recommendations for prevention of childhood obesity. Pediatrics. 2007;120:s229–53. doi: 10.1542/peds.2007-2329E. [DOI] [PubMed] [Google Scholar]
- 13.Al-Naim AR, Bamgboye EA, Al-Herbish A. The pattern of growth and obesity in Saudi Arabian male school children. Int J Obes Relat Metab Disord. 1996;20:1000–5. [PubMed] [Google Scholar]
- 14.Al-Hazzaa H. Prevalence and trends in obesity among school boys in Central Saudi Arabia between 1988 and 2005. Saudi Med J. 2007;28:1569–74. [PubMed] [Google Scholar]
- 15.Al-Hazzaa H. Rising trends in BMI of Saudi adolescents: Evidence from three cross sectional studies. Asia Pac J Clin Nuutr. 2007;16:462–6. [PubMed] [Google Scholar]
- 16.Abahussain NA, Musaiger AO, Nicholls PJ, Stevens R. Nutritional status of adolescent girls in the Eastern Province of Saudi Arabia. Nutr Health. 1999;13:171–7. doi: 10.1177/026010609901300305. [DOI] [PubMed] [Google Scholar]
- 17.Abalkhail B, Shawky S. Comparison between body mass index, Triceps, skin fold thickness, and mid-arm muscle circumference in Saudi adolescents. Ann Saudi Med. 2002;22:324–8. doi: 10.5144/0256-4947.2002.324. [DOI] [PubMed] [Google Scholar]
- 18.Alalmai SM. Prevalence of obesity and underweight among Saudi adolescents in Eastern Saudi Arabia. SMJ. 2005;6:607–11. [PubMed] [Google Scholar]
- 19.A-Saeed WY, Al-Dawood KM, Bukhari IA, Bahnassy A. Prevalence and socioeconomic risk factors of obesity among urban female in Al-Khobar city, eastern Saudi Arabia. Obesity Rev. 2006;8:93–8. doi: 10.1111/j.1467-789X.2006.00287.x. [DOI] [PubMed] [Google Scholar]
- 20.Jelliffe DB, Jelliffe EFP. Community nutritional assessment. Oxford, UK: Oxford University Press; 1989. [Google Scholar]
- 21.Must A, Dallal G, Dietz W. Reference data for obesity: 85th and 95th percentiles of body mass index (wt/ht2) and triceps skinfold thickness. Am J Clin Nur. 1991;53:839–46. doi: 10.1093/ajcn/53.4.839. [DOI] [PubMed] [Google Scholar]
- 22.El-Mouzan M, Al-Herbish A, Al-Salloum A, Qurashi M, Al-Omar A. Growth charts for Saudi children and adolescents. Saudi Med J. 2007;28:1555–68. [PubMed] [Google Scholar]
- 23.Al-Frayh A, Bamgboye E, Moussa M. The standers physical growth chart for Saudi Arabian preschool children. Ann Saudi Med. 1993;13:155–9. doi: 10.5144/0256-4947.1993.155. [DOI] [PubMed] [Google Scholar]
- 24.AlSekait MA, Nasser AN, Bamgboye EA. The growth pattern of school children in Saudi Arabia. Saudi Med J. 1992;13:14. [Google Scholar]
- 25.El-Hazmi MA, Warsy AS. Prevalence of obesity in the Saudi population. Ann Saudi Med. 1997;17:302–6. doi: 10.5144/0256-4947.1997.302. [DOI] [PubMed] [Google Scholar]
- 26.Tucci S, Peters J. Media influences on body satisfaction in female students. Psicothema. 2008;20:521–4. [PubMed] [Google Scholar]
- 27.Lawlor DA, Mamun AA, O’Callaghan MJ, Bor W, Williams GM, Najman JM. Is being overweight associated with behavioural problems in childhood and adolescence? Findings from the Mater-University study of pregnancy and its outcomes. Arch Dis Child. 2005;90:692–7. doi: 10.1136/adc.2004.062919. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Al Sabbah H, Vereecken C, Elgar F, Nansel T, Aasvee K, Abdeen Z, et al. Body weight dissatisfaction and communication with parents among adolescents in 24 countries: International cross-sectional survey. BMC Public Health. 2009;9:52. doi: 10.1186/1471-2458-9-52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.O’Brien SH, Holubkov R, Reis EC. Identification, evaluation, and management of obesity in an academic primary care center. Pediatrics. 2004;114:e154–9. doi: 10.1542/peds.114.2.e154. [DOI] [PubMed] [Google Scholar]
- 30.Musaiger AO. Overweight and obesity in the Eastern Mediterranean Region: Can we control it? East Mediterr Health J. 2004;10:789–93. [PubMed] [Google Scholar]
- 31.What is a health promoting school? School and youth health. World health organization site. [accessed on 2009 Aug 8]. Available from: http://www.who.int/school_youth_health/gshi/hps.html .
- 32.SB inAust, Kim J, Wiecha J, Troped PJ, Feldman HA, Peterson KE. School based overweight preventive intervention lower incidence of disordered weight control behaviors in early adolescent girls. Arch Pediat Adolesc Med. 2007;161:865–9. doi: 10.1001/archpedi.161.9.865. [DOI] [PubMed] [Google Scholar]
- 33.School policy framework: Implementation of the WHO global strategy on diet, physical activity and health. Geneva, Switzerland: World Health Organization; 2008. World Health Organization. [Google Scholar]
- 34.Rey-Lopez J, Rodriguez M, Moreno L. Sedentary behavior and obesity development in children and adolescents. Nutr Metab Cardiovasc Dis. 2008;18:242–51. doi: 10.1016/j.numecd.2007.07.008. [DOI] [PubMed] [Google Scholar]