

Abstract
Nasopalpebral lipoma–coloboma syndrome is characterized by nasopalpebral lipoma and eyelid coloboma. We report a case of a 16-year-old Indian girl who reported to us with this rare syndrome. Computed tomography scan showed a significantly hypodense lesion on the right side of nose which was confirmed to be a lipoma on histopathological examination. This condition should be included in differential diagnosis of conditions with congenital eyelid coloboma.
Keywords: Lid coloboma, limbal dermoid, nasopalpebral lipoma–coloboma syndrome
Nasopalpebral lipoma–coloboma syndrome is an autosomal dominant condition characterized by upper eyelid and nasopalpebral lipomas, colobomas of upper and lower eyelids, telecanthus, and maxillary hypoplasia. Two families and one sporadic case with this condition have been described in the literature.[1] We report a 16-year-old female with the typical features of the nasopalpebral lipoma–coloboma syndrome. To the best of our knowledge, this is the fourth report of this syndrome in the literature.
Case Report
A 16-year-old Indian female came with a growth on the right side of the nose which was increasing in size, and a lesion on the right eye, both of which were present since birth. She was born of a non consanguineous marriage to a 36 year old lady at full term and the parents noticed a growth on the right side of face near medial canthus of the right eye of the child since birth.
On examination, a soft lobulated mass was noted on the right side of the nose, measuring 5 × 3.5 cm, with normal overlying skin [Fig. 1]. On ophthalmological examination, the best corrected visual acuity was counting fingers 1/2 m in the right eye and 20/20 in the left eye. A notch was noted at the medial end of the right lower lid measuring 7 mm at the base, the medial margin of the notch being formed by the nasal lesion [Fig. 2]. The right lower punctum was normal but the canaliculus ended blindly at the lateral margin of the lid coloboma. A limbal dermoid measuring 8 mm was noted at the right nasal limbus [Fig. 1], and an iris coloboma was noted at the 11 o’clock position. The remainder of the anterior segment and fundus examination was unremarkable. The left eye was within normal limits. An otorhinolaryngological opinion was sought, which did not reveal any significant abnormality other than the nasal lesion. A thorough systemic examination revealed no systemic anomalies. There were no other mass lesions anywhere else on the body. A computed tomographic scan was ordered, which showed a significantly hypodense lesion on the right side of the nose that was highly suggestive of a lipoma [Fig. 3].
Figure 1.

Clinical photograph of the patient showing a soft lobulated mass on the right side of nose measuring 5 × 3.5 cm with normal overlying skin
Figure 2.

Clinical photograph of the patient showing a notch on the medial end of the right lower lid measuring 7 mm at the base. The medial margin of the notch is formed by the nasal lesion. An 8 × 5 mm limbal dermoid covering nasal half of the cornea is also seen
Figure 3.

Computed tomographic scan (axial view) of the patient showing a significantly hypodense lesion on the right side of the nose highly suggestive of lipoma
The patient underwent an uneventful excision surgery under general anesthesia, through a lateral rhinostomy incision. Histopathological examination of the mass revealed a typical lipoma [Fig. 4]. Direct closure of the eyelid coloboma was also performed. The patient is awaiting excision of the limbal dermoid for cosmetic reasons.
Figure 4.
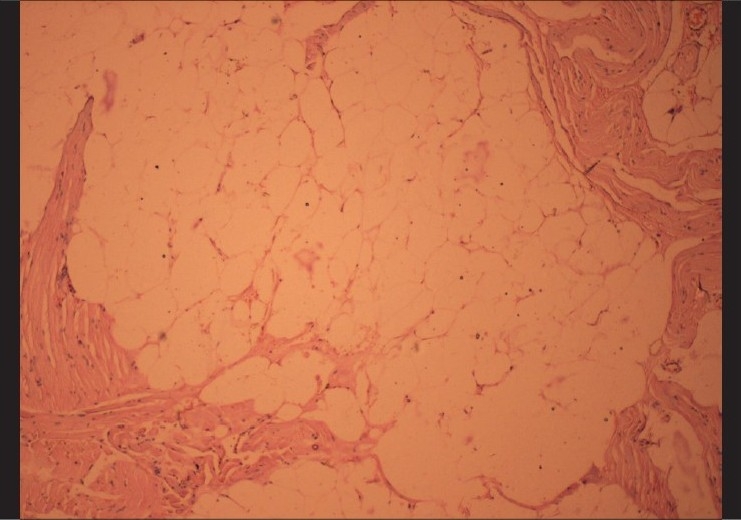
Histopathological picture of nasopalpebral lipoma showing lobules of mature adipose tissue separated by the fibrous septa H&E, ×40).
Discussion
To the best of our knowledge, this is the fourth report of lipoma-coloboma syndrome. In addition to the typical findings previously described (nasopalpebral lipoma and eyelid coloboma), our patient also had a limbal dermoid, a feature that has not been previously described in this syndrome. Limbal dermoids are choriostomas which recapitulate tissues of skin and contain dermal, epidermal, and adenexal structures with or without kerainization.
While this syndrome was first described as a familial disorder, our case, like that of Bock-Kunz et al., was sporadic.[1] In addition, all previously described cases of this condition have been bilateral, whereas our patient only had unilateral involvement.[1,2]
The differential diagnosis includes other syndromes associated with eyelid coloboma such as Goldenhar syndrome, Treacher Collins syndrome, frontonasal dysplasia, and Delleman syndrome. Characteristic features of these syndromes include preauricular tags, vertebral anomalies, epibulbar dermoid, and eyelid coloboma (Goldenhar syndrome); antimongoloid slant, colobomas of lateral lower eyelids, cataract, microphthalmos, and atresia of lacrimal passages (Treacher Collins syndrome); orbital hypertelorism, bifid nose and median facial cleft (frontonasal dysplasia); and agenesis of corpus callosum, orbital cysts, and punched out defects of lip and philtrum (Delleman syndrome). Interestingly, our patient had a limbal dermoid, a finding commonly seen in Goldenhar syndrome, but in the absence of any other features of Goldenhar syndrome, this is probably coincidental.
Management is essentially for cosmetic purposes and good results can be obtained by surgical excision of the lipoma and direct closure of the eyelid coloboma, as reported previously. The poor vision in our patient was most likely secondary to amblyopia caused by the limbal dermoid. As we have noted, the nasopalpebral lipoma–coloboma syndrome is a rare congenital disorder that can be unilateral and sporadic, and may be associated with other eye abnormalities such as limbal dermoid. It should be included in the differential diagnosis of conditions having congenital eyelid colobomas.
Acknowledgments
We would to thank Late Dr. CP Venkatesh for his guidance in diagnosing, managing, and reporting this case.
References
- 1.Bock-Kunz AL, Lyon DB, Singhal VK, Grin TR, Park O. Nasopalpebral lipoma-coloboma syndrome. Arch Ophthalmol. 2000;118:1699–701. [PubMed] [Google Scholar]
- 2.Seah LL, Choo CT, Fong KS. Congenital upper lid colobomas: Management and visual outcome. Ophthal Plast Reconstr Surg. 2002;18:190–5. doi: 10.1097/00002341-200205000-00007. [DOI] [PubMed] [Google Scholar]