

Abstract
We report a rare presentation of an initially misdiagnosed case of a pseudotumor, which on histopathology was diagnosed as bilateral breast metastases of lobular carcinoma involving multiple extraocular muscles. A 61-year-old lady presented with external ophthalmoplegia and diplopia. Incisional biopsy was performed using a lid crease approach and the patient received radiotherapy and hormonal therapy. Following prolonged hormonal therapy, complete remission was achieved, with improvement in ocular motility and resolution of diplopia, about 18 months after the initial presentation. Multiple extraocular muscle involvement by breast carcinoma metastasis is very rare and should be considered in the differential diagnosis, especially in patients with a prior history of breast carcinoma.
Keywords: Bilateral, breast metastasis, extraocular muscle
Metastases to the orbit occurs in 2-3% of the patients with systemic cancer.[1] Metastatic breast carcinoma is the most common primary tumor metastasizing to the ocular structures and accounts for 10-61% of the metastasis to the orbit.[2] However, bilateral metastases of breast carcinoma to the extraocular muscles is very rare.[2] We report a case of bilateral metastases of breast carcinoma to the extraocular muscles, and review the literature.
Case Report
A 61-year-old lady presented with diplopia of three months’ duration, in March 2008. She had been treated elsewhere with steroids for pseudotumor of the orbit. A detailed history revealed that she had undergone modified radical mastectomy with axillary clearing of the lymph nodes for right breast carcinoma (T4N2M0) in March 2006. Histopathology was suggestive of lobular carcinoma (Grade 3). She had also received radiotherapy (54 Gy) and chemotherapy. Following treatment, she had been declared to have complete clearance of the tumor, without any metastases, which was confirmed by a whole body positron emission tomography (PET) scan and negativity on testing for oestrogen and progesterone receptors. When she presented to us, her visual acuity was 20/30 in both eyes with normal anterior and posterior segments. There was restriction of extraocular movements in both eyes, right more than left. There was right upper lid retraction [Fig. 1]. Hertel's exophthalmometry revealed bilateral reading of 18 mm (base reading 106 mm). Magnetic resonance imaging demonstrated a thickening of the right superior, lateral and inferior recti, and the left superior rectus on T1, and heterogenous hyperintensity on T2 [Fig. 2]. Mild gadolinium enhancement was noticed. The tendons were seen to be spared. The PET scan revealed bulky, nodular muscles, with increase in activity. Hyperactive nodules were also noticed in the right upper lobe and left lower lobe of the lung. Biopsy of the superior rectus of the right eye was performed by a lid crease incision. On histopathology, this was confirmed as metastasis from the lobular carcinoma of the breast [Fig. 3]. At this time oestrogen and progesterone receptors were strongly positive. The ultrasound of the abdomen and bone scan were normal.
Figure 1.
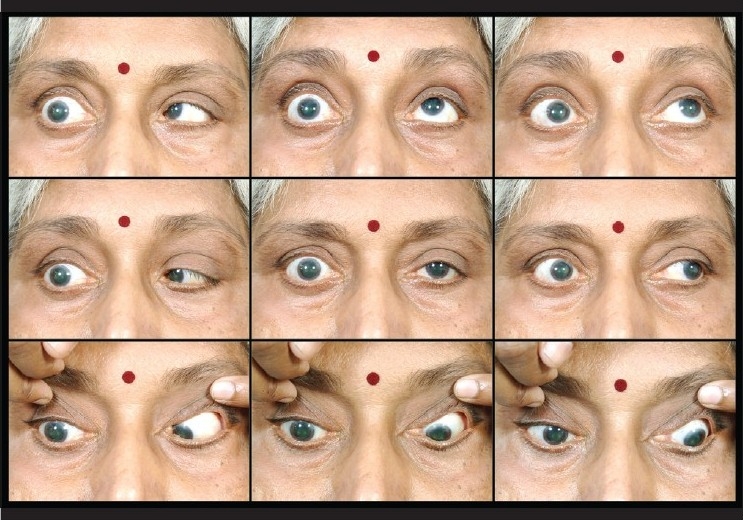
Nine gaze view at presentation revealed the presence of right upper lid retraction and limitation of ocular movements of the right eye in all directions of gaze and the left eye on depression
Figure 2.
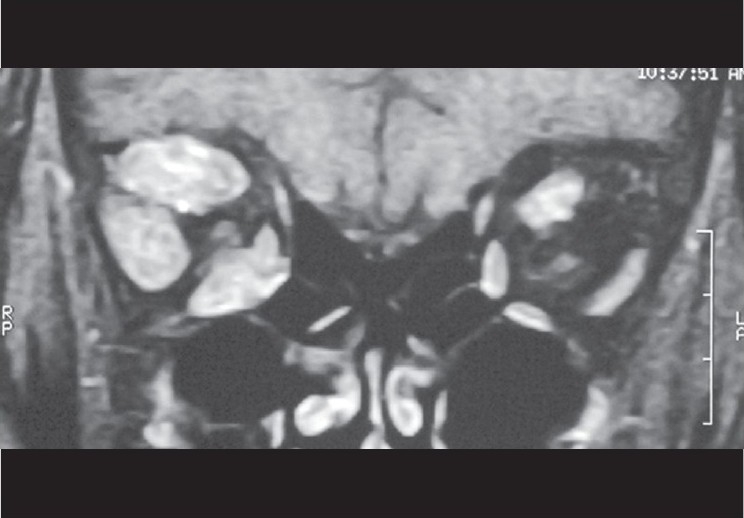
Coronal section through the orbits (T1 weighted gadolinium enhanced image) with fat suppression, showing enlargement of the right superior, lateral, and inferior recti and the left superior rectus
Figure 3.
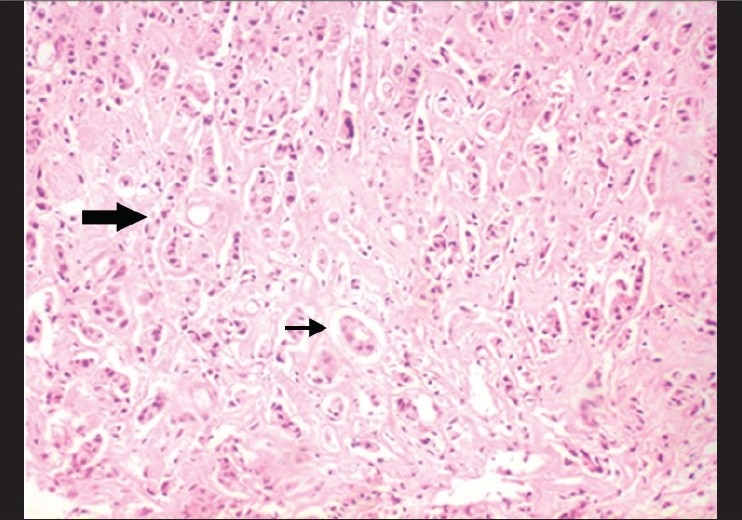
Histopathology revealed the presence of tumor cells arranged in an Indian file arrangement (bold arrow) and glandular pattern (other arrow) suggestive of lobular carcinoma of the breast, (H&E, 100×)
She was administered radiotherapy (5400 Gy to the orbit and 5000 Gy to the chest wall) and hormone therapy (Tamoxifen) for six months. After completion of the radiotherapy, there was a marked reduction in the amount of diplopia and improvement in the extraocular muscle motility. At the last follow-up, 18 months after presentation, the PET scan revealed no abnormality. She had remarkable improvement of the ocular motility and resolution of diplopia [Fig. 4], however, she developed mild bilateral ptosis.
Figure 4.
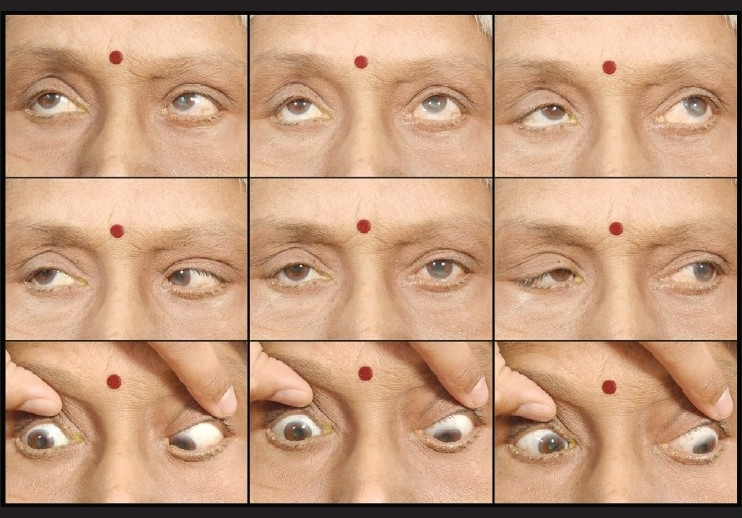
Nine-gaze view at last follow-up, there was presence of mild upper lid ptosis of the right eye and improvement of ocular movements, with the absence of any diplopia
Discussion
Bilateral metastases affecting the extraocular muscles following breast carcinoma is extremely rare, especially involvement of more than two muscles.[3,4] Constant movement of the muscles or unfavorable chemical environment has been proposed as the cause for this rarity of metastases to the extraocular muscles.[1] Clinical presentation is usually with orbital pain, decreased vision or diplopia.[5] These tumors usually respond to radiotherapy, as they are radiosensitive.
There have been only two case reports of lobular carcinoma metastasizing to the extraocular muscles, given by Toller et al.[3] and Kouvaris et al.[6] Our patient had complete resolution of the lobular carcinoma metastasis following treatment with radiotherapy and hormonal therapy with complete remission at 18 months of follow-up. Tamoxifen is a safe, selective oestrogen receptor modulator, which can reduce the incidence of contralateral breast cancer. Our case was initially treated elsewhere as a pseudotumor, with oral steroids. A high index of suspicion is needed especially in cases that present with ocular motility restriction and multiple muscle involvement. Late metastasis, even after complete remission of the primary cancer, has also been reported, with the duration between treatment and metastasis ranging from three months to 28 years.[3,7] Appropriate diagnosis by biopsy and aggressive management with radiotherapy and hormonal therapy can be effective in the management of bilateral breast cancer with multiple extraocular muscle metastases.
References
- 1.Bloch RS, Gartner S. The incidence of ocular metastatic carcinoma. Arch Ophthalmol. 1971;85:673–5. doi: 10.1001/archopht.1971.00990050675005. [DOI] [PubMed] [Google Scholar]
- 2.Bedford PD, Daniel PM. Discrete carcinomatous metastases in the extrinsic ocular muscles: A case of carcinoma of the breast with exophthalmic ophthalmoplegia. Am J Ophthalmol. 1960;49:723–6. doi: 10.1016/0002-9394(60)92047-x. [DOI] [PubMed] [Google Scholar]
- 3.Toller KK, Gigantelli JW, Spalding MJ. Bilateral orbital metastases from breast carcinoma. Ophthalmology. 1998;105:1897–901. doi: 10.1016/S0161-6420(98)91037-5. [DOI] [PubMed] [Google Scholar]
- 4.Spitzer SG, Bersani TA, Mejico LJ. Multiple bilateral extraocular muscle metastases as the initial manifestation of breast cancer. J Neuroophthalmol. 2005;25:37–9. doi: 10.1097/00041327-200503000-00010. [DOI] [PubMed] [Google Scholar]
- 5.Peckham EL, Giblen G, Kim AK, Sirdofsky MD. Bilateral extraocular metastasis from primary breast cancer. Neurology. 2005;65:74. doi: 10.1212/01.WNL.0000156359.93206.99. [DOI] [PubMed] [Google Scholar]
- 6.Kouvaris JR, Gkongkou PV, Papadimitrou CA, Papacharalampous XN, Antypas CE, Balaforta MJ, et al. Bilateral metastasis to extraocular muscles from lobular breast carcinoma. Onkologie. 2008;31:387–9. doi: 10.1159/000129689. [DOI] [PubMed] [Google Scholar]
- 7.Milman T, Pliner L, Langer PD. Breast carcinoma metastatic to the orbit: An unusually late presentation. Ophthal Plast Reconstr Surg. 2008;24:480–2. doi: 10.1097/IOP.0b013e31818b6adc. [DOI] [PubMed] [Google Scholar]