

Abstract
Objective
The purpose of the present study was to determine the incidence of dural tears and predictable factors suggesting dural tears in patients who had lumbar burst fractures with vertical laminar fractures.
Methods
A retrospective review was done on thirty-one patients who underwent operative treatment for lumbar burst fractures with vertical laminar fractures between January 2003 and December 2008. All patients were divided into two groups according to existence of dural tears, which were surgically confirmed; 21 patients with dural tears and 10 patients without dural tears. Clinical and radiographic findings were analyzed for their association with dural tears.
Results
Among a total of 31 patients, dural tears were detected in 21 (67%) patients. A preoperative neurological deficits and mean separation distances of the edges in laminar fractures were found to be the reliable factors of dural tears (p=0.001 and 0.002, respectively). Decreased ratio of the central canal diameter and interpedicular distance were also the reliable factors suggesting dural tears (p=0.006 and 0.015, respectively). However, dural tears showed no significant association with age, sex, level of injury, absence of a posterior fat pad signal, the angle of retropulsed segment, or site of laminar fracture.
Conclusion
Our study of lumbar burst fracture combined laminar fracture revealed that dural tears should be ruled out in cases of a preoperative neurological deficits, wide separation of the laminar fracture, severe canal encroachment, and wider interpedicular distance.
Keywords: Burst fracture, Dural tear, Laminar fracture
INTRODUCTION
Burst fracture is an unstable compression fracture, which includes at least the anterior and middle columns of vertebral segments, secondary to axial loading, usually with some flexion. It can cause lamina fracture, paraspinal tissue injury, hematoma, and dural tears. In the report by Ozturk et al.21), dural tears were detected in 25% of all low lumbar burst fractures. Burst fracture with dural tears can cause neural entrapment in itself, and cerebrospinal fluid (CSF) leakage leading to meningitis and posttraumatic meningocele can occur. However, determination of their existence by clinical and radiological methods prior to surgical treatment is very difficult. Some studies have suggested that change of the retrospinal soft tissue signal in T1- and T2-weighted images in magnetic resonance (MR) imaging or document sites of CSF leakage in myelography can be helpful in diagnosis of dural tears16,23). However, myelography is associated with difficulties regarding patient's tolerance and complications, such as infection or nerve injury. MR can detect spinal fractures, paraspinal soft tissue edema, and other injuries; however, detection of small dural tears <1 cm is difficult13,21). Beyond these images some studies of other predictable factors associated with dural tears have been conducted2,7,16). Lee et al.16), suggested the strong possibility of dural tear when there is a severely narrowed central canal with a more acute angle, more unstable laminar fracture, and wider interpedicular distance at the level of burst fracture. Cammisa et al.7) insisted on the importance of lamina fracture, reporting that dural tears occurred only in the presence of a lamina fracture. Atlas et al.2) reported on a strong association of burst fractures with laminar fracture. However, we have not encountered any clear guidelines for prediction of dural tears associated with lamina fractures.
The aim of this retrospective study was to determine the incidence of dural tears in patients who had lumbar burst fractures with vertical laminar fractures, and to determine whether or not specific clinical and radiographic factors might be predictive of dural tears.
MATERIALS AND METHODS
From January 2003 to December 2008, we performed surgery on 123 patients at our institute in patients with lumbar burst fractures. Among them, a retrospective analysis was performed in 31 patients who had combined laminar fractures at the same level. Patients with multi-level fractures, combined disk herniation, absence of lamina fractures, or fracture/dislocation were excluded. A review of all hospital clinical records and radiographs for these patients was conducted. Neurological status was assessed using Frankel's scale at the time of injury and follow-up evaluations were obtained. Plain X-rays, computed tomography (CT) including sagittal reconstruction, and MR imaging were obtained in all cases. Review of CT and magnetic resonance imaging (MRI) images was performed by a musculoskeletal radiologist.
Indications for surgery included neurological impairment and/or instability. Surgery was performed in patients with 50% or greater vertebral body compression and/or kyphosis measuring at least 20°. All patients had undergone surgery using the midline posterior approach within one week after injury; any dural tears or nerve root entrapment was replaced and repaired. All patients underwent posterior stabilization of their spine using transpedicular screw rod systems. A total of 28 patients underwent treatment with the posterior approach only, and 3 patients underwent treatment with the combined posterior/anterior approach due to progression of kyphotic deformity after posterior instrumentation and fusion.
All patients with lumbar burst fracture with vertical lamina fracture were divided into two groups according to existence of dural tears, which was surgically confirmed (Table 1). Group A consisted of 21 patients who had burst fractures and laminar fractures with dural tears, which was confirmed during surgery; group B consisted of 10 patients who had burst fractures and laminar fractures without dural tears. We investigated preoperative neurological status, absence of posterior fat pad signal, and site of the laminar fracture, and analyzed separation distance of the laminar fracture, degree of neural canal encroachment, interpedicular distance, vertebral compression percentage, and the angle of retropulsed segment for their association with dural tears. Degree of neural canal encroachment was measured by the ratio of retropulsed bony fragment anteroposterior diameter and central canal anteroposterior diameter (Fig. 1); interpedicular distance was measured at the level of the widest point of fracture in anteroposterior (AP) view (Fig. 2). The angle of retropulsed segment was measured by the most acute angle of the retropulsed segment in the sagittal plane (Fig. 3). Sites of laminar fractures were divided into midline and lateral positions. Laminar fractures involving the spinous process were regarded as midline laminar fractures. Also, distance of separated of lamina was measured in axial plane of CT (Fig. 4).
Table 1.
Data on the patients who had lumbar burst fracture with vertical lamina fracture

*according to the classification of Frankel (initial examination at follow-up). a : anterior surgery, p : posterior surgery, + : occurred, - : not occurred, M : midline, L : lateral
Fig. 1.
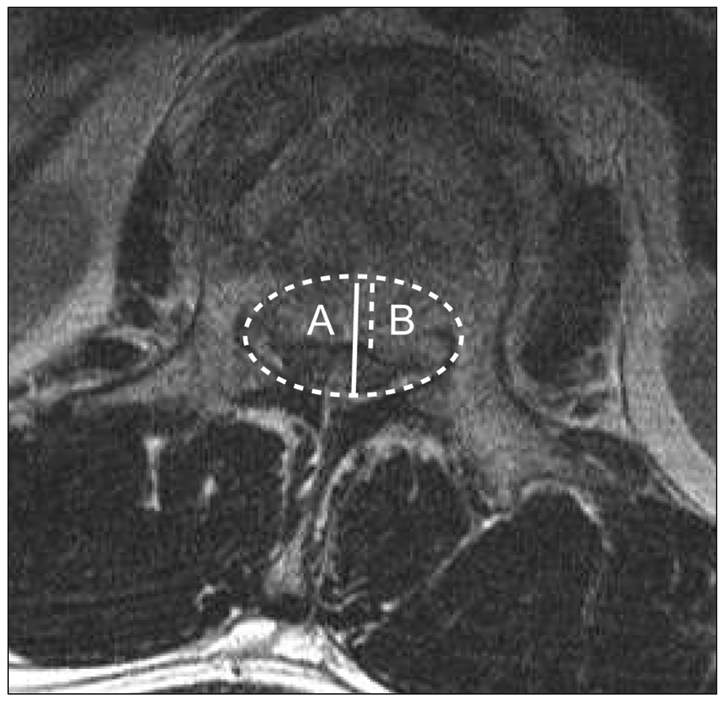
The degree of neural canal encroachment. The neural canal was measured with AP diameter of normal central canal (A) and encroached portion of central canal (B). The ratio of central canal encroachment was measured dividing B by A.
Fig. 2.
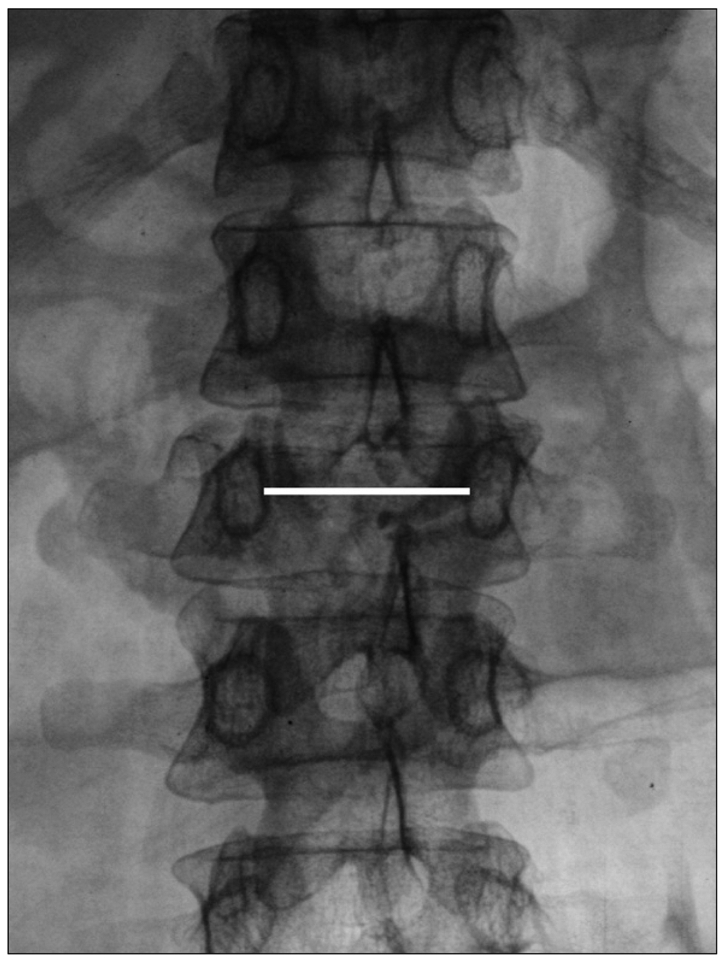
The interpedicular distance. The interpedicular distance was measured between the pedicles on an anteroposterior radiograph.
Fig. 3.

The angle of retropulsed segment. The angle of retropulsed segment was measured by the most acute angle of the retropulsed segment in the sagittal plane.
Fig. 4.
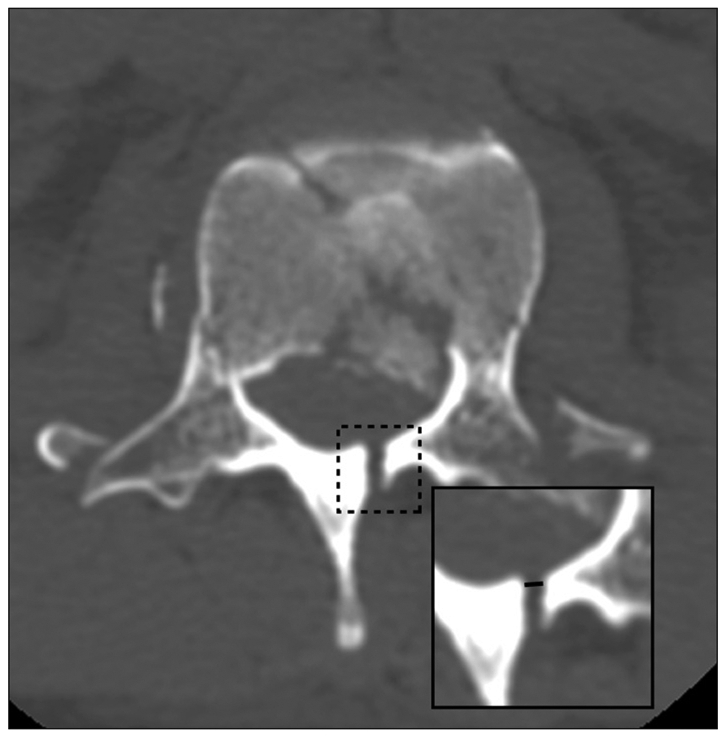
The distance of separated lamina. The distance of separated of lamina was measured by gap of fractured lamina in axial plane.
Chi-square test for neurological status, absence of a posterior fat pad signal, site of the laminar fracture, and two sample t-test for separation distance of the laminar fracture, IP distance, degree of neural canal encroachment, the angle of retropulsed segment, and vertebral compression percentage were used for statistical analysis using the Statistical Package for the Social Sciences for windows 17.0. The level of statistical significance was set at p-value <0.05.
RESULTS
We performed a retrospective analysis of 31 patients who had lumbar burst fractures with combined laminar fractures. There were 21 males and 10 females enrolled in the study ranged in age from 23 to 64 (mean 43±9.9) years. Average follow-up period was 44 (range 6-69) months. Twenty-one (67.7%) of all patients had been confirmed to have associated dural tears (group A) and the remaining 10 patients not associated dural tears (group B). The clinical characteristics and each MR imaging findings of two groups were summarized in Table 1.
All patients (100%) in group A had a neurological deficit prior to surgical treatment, whereas, in group B, the percentage of patients with a neurological deficit was 30% before surgery. A preoperative neurological deficit in the presence of a burst fracture and an associated laminar fracture was a statistically significant predictable factor of dural tears (p=0.001). Although 24 patients (77.4%) had a preoperative neurological deficit, Frankel's grade D or E results were obtained in twenty-nine (93%) of thirty-one patients after surgery.
Absence of a posterior fat pad signal was detected in 20 patients (95%) in group A and 7 patients (70%) in group B (p=0.087). Mean separation distances of the edges in laminar fractures in groups A and B were 2.4±1.2 mm and 1.0±0.6 mm, and were predictable factors of dural tear (p=0.002). In group A, mean decreased ratio of the central canal diameter was 61.9±17.0% and inter pedicular distance was 32.4±3.9 mm. On the other side, the parameters were 43.8±12.0% and 28.4±3.8 mm in group B (p=0.006 and 0.015). These factors were suggestive of dural tears. Ratio of vertebral body compression was 47.5±14.7% for group A and 40.0±12.0% for group B (p=0.183), and the angle of retropulsed segment was 37.2±13.1° for group A and 39±8.0° for group B (p=0.708).
Dural tears showed no significant association with age, sex, level of injury, absence of a posterior fat pad signal, the angle of retropulsed segment, or site of laminar fracture. According to logistic regression, the preoperative neurological deficit was the most reliable factor, suggesting dural tears, compared with other factors (Odds ratio=19.0, 95% confidence interval=1.4-248.4).
DISCUSSION
In the operative field of thoracolumbar burst fracture, dural tear is not an uncommon finding9). It can cause CSF leakage and this in turn can lead to pseudomeningocel, infection, meningitis, or damage to neural structure. These are related to prognosis of patients. Furthermore, inappropriate spinal reductions without identification of dural tear can result in additional dural tears and injury of neural structures. When we knows about the presence of dural tears preoperatively, operating time and efforts to find out and treat dural tears will significantly decreased, and the frequency of missing dural tear also be decreased. A number of studies have been conducted for evaluation of many factors that can be considered in prediction of the incidence of dural tear; however, there are some controversies.
Argenson et al. reported greater frequency of dural tears in the lumbar area6). However, clinical or radiological diagnosis of dural laceration prior to surgery is very difficult. Identification of dural tears before surgery is important for prevention of further neurologic injury and for promotion of neurological recovery during treatment of burst fractures.
In our study, we conducted a review of 31 patients who had a lumbar burst fracture with a vertical laminar fracture. Pre-operative neurologic deficit, distance of separated lamina, ratio of central canal encroachment, and interpedicular distance were significant factors suggestive of dural tears.
Miller et al.18) reported the presence of dural tears and entrapment of cauda equina in thoracolumbar fractures and advised surgical replacement of the roots and repair of the dura in order to prevent complications. They documented the presence of dural tears and herniation of the nerve root in patients with thoracolumbar burst fractures associated with separation of pedicles, pointing out that neural elements were often entrapped between fracture fragments of lamina.
Neurological injury has been reported to occur in 30-60% of patients with thoracolumbar burst fractures13). A significant association between dural tears and neurological deficit has been reported1,7,12,18,23). Cammisa et al.7) reported that a preoperative neurological deficit in association with a lumbar burst fracture and laminar fracture was a sensitive (100%) and specific (74%) predictable factor of dural tears. They concluded that patients with neurological deficit and lamina fracture associated with a lumbar bursting fracture have an increased risk of dural tears and entrapment of neural elements. Kahamba et al.12) also suggested a significant association between the presence of dural tears and a severe neurological deficit. They emphasized that for patients who have lamina fractures with neurological deficit, the possibility of dural tears with the aforementioned complication should be a major concern. Neurologic dysfunction in the lumbar area simulates peripheral nerve injury with the potential for spontaneous recovery with proper treatment. In our series, Frankel's grade D or E neurological outcomes were obtained in 29 (93%) of 31 patients. Patients with neurological deficits and a laminar fracture associated with a lumbar burst fracture are at increased risk for dural tears in addition to the possibility of nerve root entrapment. Neurological deficit can occur with related displacement of the nerve root. In our series, neurological deficit was a sensitive (100%) and specific (78%) predictable factor of dural tears.
Ozturk et al.21) reported on treatment of 28 patients with low lumbar burst fractures. All of their patients had greenstick lamina fractures. Dural tear was detected in 25% of these patients. Mean distance of separated laminas with and without dural tear was 4.35 mm and 1.89 mm. In our study, the distance of the lamina was 2.4±1.2 mm and 1.0±0.6 mm between the 2 groups (p=0.002). It showed statistically significant difference in 2 groups. With an increased gap between lamina and sharp edges, the chance of damage caused by a displaced duramater will be increased. Although the result revealed statistical significance, the difference of two groups were only 1.4 mm. So, we could not exclude the errors in measuring distance of separated lamina. However, considering the results of previous study of Ozturk and ours, we may assume that increased fracture gap of lamina was related to the greater incidence of dural tears. Therefore, patients with a wide distance of separated lamina may have an increased risk of dural tears.
Atlas et al.2) reported that burst fractures were combined with laminar fracture in 85.3% of their patients with burst fractures. Posterior dural tears in lumbar burst fractures are always associated with laminar fractures. Many investigators have found that a burst fracture with an associated laminar fracture was very sensitive and specific for the presence of dural tears7,18). Of the thirty-one patients in our series who had a burst fracture with a vertical laminar fracture, twenty-one (67%) had dural tears.
Under axial loading, pedicles and posterior elements splay laterally, and bone is retropulsed from the vertebral body, which can cause narrowing of the spinal canal. Direct contact with a fragmented vertebral body and disc can result in development of a dural tear. Lee et al.16) suggested the strong possibility of dural tears when MRI findings show a central canal severely narrowed to less than one half by displaced bone fragments. In our study, ratio of central canal encroachment (p=0.006) was also a significant parameter representing dural tears in spinal burst fracture with laminar fracture.
There were some controversies over interpedicular distance. According to Cammisa et al., there was no statistical significance between dural tear and interpedicular distance18). However, Lee et al.16) suggested a strong possibility of dural tear when there was a wider IP distance (>28 mm). Interpedicular distance was also an important predictable factor of dural tear in our study. Mean interpedicular distance was 32.4±3.9 mm in patients with dural tears and 28.4±3.8 mm in those who did not have dural tears (p=0.015).
In our study, dural tears showed no significant association with age (p=0.332), sex (p=0.222), level of injury (p=0.406), absence of a posterior fat pad signal (p=0.087), or site of laminar fracture (p=0.441). Ozturk et al.21) reported on disappearance of signals in axial MRI posterior fat pads when there was a laminar fracture and nerve root entrapment. In our series, twenty of 21 patients with dural tears showed loss of posterior fat pad signals. However, seven of 10 patients without dural tears also showed absence of posterior fat pad signals. Contrary to our statistical results, several studies have shown that positive relation about fat pad signal and dural tears. Our study result did not reveal statistical significance like other previous studies. It may be due to small number of study group. Nevertheless, our result may reflect the tendency of relationship (p=0.087).
CONCLUSION
The result of this study revealed that dural tear might be suggestive in cases of a preoperative neurological deficit, wide separation of the laminar fracture, severe canal encroachment, and wider interpedicular distance. If radiologic findings and predictive factors strongly suggest possibility of a dural tear, surgeons will make an effort to find out the presence or absence of a true dural tear, even very small size around fracture sites. And, it may be helpful to decrease the frequency of missing a small size dural tear in operative field.
Table 2.
The values of each parameter and the statistical significance

M : midline, L : lateral, + : occurred
References
- 1.Andreychik DA, Alander DH, Senica KM, Stauffer ES. Burst fractures of the second through fifth lumbar vertebrae. Clinical and radiographic results. J Bone Joint Surg Am. 1996;78:1156–1166. doi: 10.2106/00004623-199608000-00005. [DOI] [PubMed] [Google Scholar]
- 2.Atlas SW, Regenbogen V, Rogers LF, Kim KS. The radiographic characterization of burst fractures of the spine. AJR Am J Roentgenol. 1986;147:575–582. doi: 10.2214/ajr.147.3.575. [DOI] [PubMed] [Google Scholar]
- 3.Aydinli U, Karaeminoğullari O, Tişkaya K, Ozturk C. Dural tears in lumbar burst fractures with greenstick lamina fractures. Spine. 2001;26:E410–E415. doi: 10.1097/00007632-200109150-00012. [DOI] [PubMed] [Google Scholar]
- 4.Bohlman HH, Eismont FJ. Surgical techniques of anterior decompression and fusion for spinal cord injuries. Clin Orthop Relat Res. 1981:57–67. [PubMed] [Google Scholar]
- 5.Bosacco SJ, Gardner MJ, Guille JT. Evaluation and treatment of dural tears in lumbar spine surgery : a review. Clin Orthop Relat Res. 2001:238–247. doi: 10.1097/00003086-200108000-00033. [DOI] [PubMed] [Google Scholar]
- 6.Bridwell KH. Low lumbar (L3-L4-L5) burst fractures. In: Floman Y, Farcy JPC, Argenson C, editors. Thoracolumbar spine fracture. New York: Raven; 1993. pp. 223–234. [Google Scholar]
- 7.Cammisa FP, Jr, Eismont FJ, Green BA. Dural laceration occurring with burst fractures and associated laminar fractures. J Bone Joint Surg Am. 1989;71:1044–1052. [PubMed] [Google Scholar]
- 8.Carl AL, Matsumoto M, Whalen JT. Anterior dural laceration caused by thoracolumbar and lumbar burst fractures. J Spinal Disord. 2000;13:399–403. doi: 10.1097/00002517-200010000-00005. [DOI] [PubMed] [Google Scholar]
- 9.Choe IS. Therapeutic results of CSF leakage due to unintended incidental durotomy in spine surgery. J Korean Neurosurg Soc. 2004;35:574–578. [Google Scholar]
- 10.Denis F, Burkus JK. Diagnosis and treatment of cauda equina entrapment in the vertical lamina fracture of lumbar burst fractures. Spine. 1991;16:S433–S439. [PubMed] [Google Scholar]
- 11.Jelsma RK, Kirsch PT, Rice JF, Jelsma LF. The radiographic description of thoraco-lumbar burst fractures. Surg Neurol. 1982;18:230–236. doi: 10.1016/0090-3019(82)90328-7. [DOI] [PubMed] [Google Scholar]
- 12.Kahamba JF, Rath SA, Antoniadis G, Schneider O, Neff U, Richter HP. Laminar and arch fractures with dural tear and nerve root entrapment in patients operated upon for thoracic and lumbar spine injuries. Acta Neurochir (Wien) 1998;140:114–119. doi: 10.1007/s007010050071. [DOI] [PubMed] [Google Scholar]
- 13.Keene JS, Fischer SP, Drummond DS. The neurological consequences of post traumatic impingement; Presented at the 52nd Annual Meeting of American Academy of Orthopaedic Surgeons; Las Vegas, Mevada. [Google Scholar]
- 14.Keenen TL, Antony J, Benson DR. Dural tears associated with lumbar burst fractures. J Orthop Trauma. 1990;4:243–245. doi: 10.1097/00005131-199004030-00001. [DOI] [PubMed] [Google Scholar]
- 15.Krudy AG. MR myelography using heavily T2-weighted fast spin-echo pulse sequences with fat presaturation. AJR Am J Roentgenol. 1992;159:1315–1320. doi: 10.2214/ajr.159.6.1442408. [DOI] [PubMed] [Google Scholar]
- 16.Lee IS, Kim HJ, Lee JS, Kim SJ, Jeong YJ, Kim DK, et al. Dural tears in spinal burst fractures: predictable MR imaging findings. AJNR Am J Neuroradiol. 2009;30:142–146. doi: 10.3174/ajnr.A1273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Marciello MA, Flanders AE, Herbison GJ, Schaefer DM, Friedman DP, Lane JI. Magnetic resonance imaging related to neurologic outcome in cervical spinal cord injury. Arch Phys Med Rehabil. 1993;74:940–946. [PubMed] [Google Scholar]
- 18.Miller CA, Dewey RC, Hunt WE. Impaction fracture of the lumbar vertebrae with dural tear. J Neurosurg. 1980;53:765–771. doi: 10.3171/jns.1980.53.6.0765. [DOI] [PubMed] [Google Scholar]
- 19.Morris RE, Hasso AN, Thompson JR, Hinshaw DB, Jr, Vu LH. Traumatic dural tears: CT diagnosis using metrizamide. Radiology. 1984;152:443–446. doi: 10.1148/radiology.152.2.6739812. [DOI] [PubMed] [Google Scholar]
- 20.Osaka K, Handa H, Watanabe H. Traumatic intrathoracic meningocele (Traumatic subarachnoid-pleural fistula) Surg Neurol. 1981;15:137–140. doi: 10.1016/0090-3019(81)90033-1. [DOI] [PubMed] [Google Scholar]
- 21.Ozturk C, Ersozlu S, Aydinli U. Importance of greenstick lamina fractures in low lumbar burst fractures. Int Orthop. 2006;30:295–298. doi: 10.1007/s00264-005-0052-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Pau A, silvestro C, Carta F. Can lacerations of the thoraco-lumbar dura be predicted on the basis of radiological patterns of the spinal fractures? Acta Neurochir (Wien) 1994;129:186–187. doi: 10.1007/BF01406502. [DOI] [PubMed] [Google Scholar]
- 23.Pickett J, Blumenkopf B. Dural lacerations and thoracolumbar fractures. J Spinal Disord. 1989;2:99–103. [PubMed] [Google Scholar]
- 24.Schmidek HH, Gomes FB, Seligson D, McSherry JW. Management of acute unstable thoracolumbar (T-11-L-1) fractures with and without neurological deficit. Neurosurgery. 1980;7:30–35. doi: 10.1227/00006123-198007000-00005. [DOI] [PubMed] [Google Scholar]