

Abstract
Objective
Compared to non-bingers, binge drinkers are more likely to drive while intoxicated. The extent to which binge frequency impacts confidence in driving and subsequent driving impairment is unknown. This study compared the effects of an experimenter-delivered alcohol binge on subjective impairment and simulated driving ability in female High and Low Frequency bingers.
Methods
Female drinkers were assigned to High Frequency (n=30) or Low Frequency (n=30) binge groups based on their Alcohol Use Questionnaire responses. At 30-minute intervals within a two-hour period, participants received either a placebo drink (n=15 per group) or a 0.2 g/kg dose of alcohol (n=15 per group; cumulative dose 0.8 g/kg). Self-reported impairment, driving confidence, and simulated driving were then measured.
Results
Self-reported confidence in driving was significantly lower after alcohol than after placebo in Low Frequency but not High Frequency bingers. Self-reported impairment and collisions during simulated driving were significantly greater after alcohol than after placebo in both Low Frequency and High Frequency bingers.
Conclusions
The impairing effects of a single alcohol binge on driving ability in females are not influenced by binge frequency. However, high binge frequency may be associated with a less cautious approach to post-binge driving.
Keywords: alcohol, automobile driving, binge drinking, subjective effects
Introduction
Binge drinking is a hazardous behavior that is steadily increasing within the United States (Naimi et al., 2003). It has been linked to unsafe sexual behavior, assaults, falls, injuries, and automobile crashes (Wechsler et al., 1994, 1998). Binge drinking is a common occurrence on college campuses, with 44% of college students identifying themselves as binge drinkers (Wechsler et al., 2000). Though generally associated with college-aged individuals, binge drinking extends well into adulthood, with a reported 75% of binge episodes involving adults over 25 years of age (Naimi et al. 2003).
According to the National Institute on Alcohol Abuse and Alcoholism (NIAAA; 2004), an alcohol “binge” is a pattern of drinking that produces a blood alcohol concentration of 0.08%, typically corresponding to five drinks for men and four drinks for women, consumed within a 2-hour period. Binge drinking differs from regular drinking in that it is characterized by the consumption of large amounts of alcohol within a short time, followed by any length of abstinence (Townshend and Duka, 2005). However, there is no consensus in the epidemiological data on the definition of a “binge drinker” (Herring et al., 2008). Recent studies have typically characterized binge drinkers according to their frequency of binge episodes, defining a binge drinker as an individual who has consumed 5 or more drinks in one sitting at least once in the past two weeks (Wechsler and Nelson, 2006) or 30 days (Marczinski and Fillmore, 2009).
Much criticism surrounds the NIAAA definition's ability to differentiate social and potentially problematic drinking (DeJong, 2003; Dimeff et al., 1995; Perkins, 2002). Some researchers argue that the purpose of a binge measure is for “public health surveillance” (i.e. categorizing a behavior but not labeling a behavior) and not to diagnose alcohol use disorders (Wechsler and Nelson, 2006). Individuals who begin drinking early in adolescence and continue to escalate their binge intake and frequency are most at risk for abuse and dependence (Chassin et al., 2002). The frequency of binges may influence not only the trajectory leading to alcohol misuse, but may also lead to increases in risk-taking behavior following drinking. Reporting frequent patterns of bingeing coincides with a greater incidence of alcohol-related negative consequences, including driving while intoxicated and DUI arrests, compared to reports by non-bingers (Presley and Pimentel, 2006). A binge score (i.e., a measure designed to look at the pattern of drinking) may be a more accurate way of linking alcohol use to future abuse and dependence (Townshend and Duka, 2002), as the act of engaging in an NIAAA defined alcohol binge in itself is not adequate to develop alcohol use and abuse problems.
Binge drinking has long been a behavior associated with males, but recent data show binge drinking is steadily increasing in females. From 1993-2001, there was a 4% increase in American college-aged women reporting frequent binges. During this time period females reported significant increases in excessive binge intake, intoxication, and episodes of drinking with the intention to become intoxicated (Wechsler et al., 2002). Women experience greater impairment as a result of alcohol consumption than men (Witt, 2007). This greater impairment may be accounted for by less body water available for alcohol distribution in women, and lower levels of alcohol dehydrogenase (Perkins, 2002). These differences account for women experiencing more rapid intoxication and higher blood alcohol levels than males consuming the same amount of alcohol (Ham & Hope, 2003). Thus, the risks and impairments associated with binge drinking may be relatively greater in women than in men.
Binge drinking leads to impaired driving in an estimated 80% of cases (Quinlan et al., 2005). According to the National Highway and Safety Administration (1998), approximately two thirds of traffic fatalities due to alcohol intoxication were caused by drivers with breath alcohol concentrations greater than 0.08%. Thus, drinking alcohol in a binge manner (i.e. consuming alcohol in a short amount of time and reaching a blood alcohol concentration of ≥ 0.08%) may be a predominant cause of driving related accidents. A recent survey found that 88% of respondents who reported alcohol-impaired driving engaged in binge drinking in the past 30 days (Flowers et al., 2008). Additionally, binge drinkers are 14 times more likely to drive while under the influence of alcohol than nonbingeing individuals (Naimi et al. 2003).
Despite evidence linking binge drinking to alcohol-impaired driving, the reason why binge drinkers are more likely to drive while intoxicated is poorly understood. One possible explanation for driving while intoxicated is underestimation of intoxication by the driver (Beirness, 1987), a phenomenon characteristic of binge drinkers. When compared to non-bingers, individuals bingeing once per week report feeling less impaired by alcohol, despite no significant group differences in alcohol-induced impairment on psychomotor tasks (Brumback et al., 2007). Other studies have found that compared to non-binge drinkers, binge drinkers reported a greater willingness to drive following an acute dose of alcohol (Marczinski et al., 2008; Marczinski and Fillmore, 2009), though both groups exhibited the same amount of alcohol-induced simulated driving impairment. These differences between regular binge drinkers and individuals with a rare or non-existent binge history suggest that an increased frequency of binge drinking episodes coincides with reduced feelings of intoxication after alcohol consumption.
The goal of the present study was to determine the influence of binge frequency on simulated driving behavior and subjective ratings of impairment and driving confidence in females after consumption of alcohol. The study used a randomized, between subjects, placebo-controlled design to compare the behavioral effects of an experimenter-controlled alcohol binge in High Frequency versus Low Frequency binge drinkers. Participants received either placebo or an alcohol dose of 0.8 g/kg, administered in a binge-like manner (i.e., four 0.2 g/kg drinks over a 2-hour time period) to assess impaired driving at a breath alcohol concentration (BrAC) of 80mg/100ml (0.08%), the legal limit for impaired driving in each of the United States. We hypothesized that Low and High Frequency binge drinkers would be similarly impaired by alcohol on a task of simulated driving, but the High Frequency binge drinkers would report feeling less impaired and more confident in driving after a simulated binge.
Methods
Participants
Sixty healthy women between the ages of 21 and 29 years participated in this study (mean age = 23.8, SD = 2.4). This sample included 9 African-Americans, 1 Asian, 1 Native-American, and 49 Caucasians. Participants were recruited from the community via television, radio, and internet networking site advertisements soliciting females who drank alcohol at least once per month. Exclusion criteria included current illicit or psychoactive drug use within the past six months, self-reported Axis I psychiatric disorder, IQ less than 80, recent head trauma, and pregnancy. Hazardous drinkers were excluded as determined by a score greater than 12 on the Alcohol Use Disorders Identification Test (AUDIT; Babor et al., 2001). During the initial phone screen, participants were classified as either High Frequency or Low Frequency binge drinkers by the numerical score derived from their responses to the final three questions of the Alcohol Use Questionnaire (Mehrabian and Russell, 1978). These questions quantify the number of drinks consumed per hour, the number of times drunk (loss of coordination, nausea, and/or ability to speak clearly) in the past 6 months, and the percentage of times that drinking leads to intoxication. High Frequency binge drinkers were defined by a score ≥ 24 (Townshend and Duka, 2002). Low Frequency binge drinkers had scores < 24 and reported only one NIAAA defined binge session per month in the past three months. After phone screening procedures, participants were invited to the laboratory for a screening visit. The study protocol was approved by the Wake Forest University School of Medicine Institutional Review Board and all participants gave informed consent.
General Procedure
The screening visit and testing visit were held on two consecutive days for the majority of participants. During the first visit, participants were administered the modified Structured Clinical Interview for DSM-IV Axis I Disorders (SCID; First el al., 2001) and the Wechsler Abbreviated Scale for Intelligence (WASI; Psychological Corporation, 1999). Additionally, urine samples were collected to test for the presence of illicit drugs (Multi-drug 6 line urine screen; Innovacon, Inc, San Diego, CA) and pregnancy (QuickVue; Quidel, San Diego, CA). A positive test result for either drug use or pregnancy excluded the individual from participation. All participants were given instructions in completing the test battery, and practiced each of the tasks (described below).
All Low and High Frequency binge drinkers eligible for participation following the screening visit returned to the laboratory for the second testing day. Upon arrival, a urine sample was collected and tested for the presence of illicit drugs and for pregnancy. Additionally, an expired air sample was collected and tested to verify the absence of alcohol (Intoxilyzer SD-5; CMI Inc., Owensboro, KY). Each participant was randomly assigned to either the placebo or alcohol group. This randomization yielded four groups: 1) High Frequency binge drinkers receiving placebo (n=15); 2) High Frequency binge drinkers receiving alcohol (n=15); 3) Low Frequency binge drinkers receiving placebo (n=15); and 4) Low Frequency binge drinkers receiving alcohol (n=15). The study design was double blinded. Participants were administered placebo or alcohol beverages and then completed the test battery. All subjects completed the entirety of the screening and testing visit alone, to minimize any influence of peers on behavior and to maintain participant confidentiality.
Alcohol Administration
All participants were informed that they would be receiving a total of four beverages, either placebo or alcohol, over a two-hour period. Beverages containing alcohol were composed of 0.2 g/kg (adjusted for specific gravity) of 95.0% alcohol added to tonic water for a total volume of 8 oz; all beverages were delivered in opaque Styrofoam cups covered with an opaque lid and were consumed through a straw. All alcohol concentrations were reduced by 8% to adjust for alcohol metabolism in females (Hindmarch et al., 1991). Placebo beverages were of equal volume but consisted only of tonic water, with alcohol on the lid and straw to provide olfactory and gustatory cues of alcohol. Each participant was allowed 10 minutes to drink each beverage and 20 minutes for absorption. After the 20 minute absorption period, a new beverage was delivered by the experimenter. After delivery of the final beverage, expired breath alcohol measurements were taken (INTOXILYZER 5000, CMI, Inc., Owensboro, KY) and the testing battery was administered. Expired-air samples were taken before the cognitive test battery and every 20 minutes after testing to monitor BrAC levels. After completion of the test battery, participants reaching an expired breath alcohol level of <0.03% and satisfactorily completing a field sobriety test were allowed to leave the laboratory with a previously appointed designated driver.
Test Battery
Visual Analog Scale (VAS)
Each visual analog scale consisted of a question below which a 100-mm horizontal line indicated a range of responses from “not at all” to “extremely.” Questions included: “I feel impaired” and “I am confident in operating a vehicle.” Participants indicated their answer to each question by drawing a vertical line perpendicular to the horizontal line. Scores were calculated as the distance in millimeters from the left edge of the scale to the intersecting line drawn by the participant (0-100).
Simulated Driving Task
The STISIM DriveTM (Systems Technology, Inc., Hawthorne, CA) is a personal computer-based interactive driving simulator designed to represent a range of psychomotor, divided attention, and cognitive tasks involved in driving. Participants drive through a nine mile course encompassing urban and rural areas with moderate to high traffic while obeying all traffic laws. To provide performance contingencies and motivation for attentive driving, a $20 bonus was given to participants who finished the course in 16.5 minutes or less. However, $2 was subtracted from this bonus for each error. Errors were defined as off-road accidents, collisions, pedestrians hit, speed exceedances, speeding tickets, traffic light tickets, stop sign tickets, centerline crossings, and road edge excursions.
Data Analysis
Age, IQ, and average drinks per week were analyzed using 2 × 2 analyses of variance (ANOVA) with binge frequency (Low/High) and dose assignment (alcohol/placebo) as factors. Chi Square analysis (white vs. nonwhite) was used to compare racial distribution across the High and Low Frequency groups. Within each binge frequency category, Mann-Whitney Rank Sum tests were used to compare the alcohol and placebo groups' median drinks per hour, total times drunk in the past six months, and percent of drinking episodes leading to intoxication. Breath alcohol concentrations were analyzed using a 2 × 2 mixed model ANOVA with binge frequency (Low/High) as a between-subjects factor and time (pre/post testing) as a repeated factor. VAS scores, driving bonus earned, and selected driving errors were analyzed using 2 × 2 ANOVAs with binge frequency (Low/High) and dose (alcohol/placebo) factors. To minimize the number of tests while allowing for identification of specific behavioral impairments, only the four most frequently occurring simulated driving errors across all subjects were selected for analyses. One participant's data was not included in driving data analyses due to experimenter error. Bonferroni post hoc pair-wise comparisons were made after each significant interaction and considered significant at p = 0.05.
Results
Group Demographics
A main effect of binge frequency on age revealed that the High Frequency group was significantly older than the Low Frequency group, F(1,56) = 8.41, p < 0.01 (Table 1). There was neither a significant main effect of dose assignment nor a significant binge frequency/dose assignment interaction effect on age. There were no significant main effects or interactions of binge frequency or dose assignment on IQ or drinks consumed per week. Chi Square analysis found no significant differences in racial distribution between the High and Low Frequency groups. Within the Low Frequency binge group, mean drinks per hour, total times drunk in the past six months, and percent of drinking episodes leading to intoxication did not differ as a function of dose assignment. Within the High Frequency binge group, mean drinks per hour and total times drunk in the past six months did not differ as a function of dose assignment. However, the High Frequency bingers assigned to the placebo group reported a significantly higher percentage of drinking episodes leading to intoxication (median = 50%) than the High Frequency bingers assigned to the alcohol group (median = 20%), U=53.5, n1 = n2 = 15, p < 0.05 (Table 1).
Table 1. Demographic and Questionnaire Measures for Low- and High-Frequency Binge Drinkers.
| Low Frequency (n=30) | High Frequency (n=30) | ||
|---|---|---|---|
| Mean (SD) | Mean (SD) | p value | |
| Age (years) | 23.0 (1.8) | 24.7 (2.6) | <0.01 |
| Race (Non-Caucasian) | 7 African-American, 1 Asian | 2 African-American, 1 Native American, 1 Hispanic | 0.18 |
| I.Q. | 114.0 (2.8) | 113.6 (2.2) | 0.91 |
| Average drinks/week | 6.1 (5.0) | 8.4 (4.2) | 0.07 |
| Average drinks/hour | 1.8 (0.8) | 1.9 (1.0) | 0.78 |
| Times drunk/past 6 months | 2.1 (2.1) | 9.0 (6.9) | <0.001 |
| Percent drinking episodes leading to intoxication | 6.7 (4.9) | 38.1 (22.8) | <0.001 |
| Cumulative binge score | 10.7 (5.8) | 49.0 (24.7) | <0.001 |
Breath Alcohol Concentrations
Breath alcohol concentrations (BrACs) were significantly lower after simulated driving than before simulated driving, F(1,28) = 11.00, p < 0.01. There was no significant main effect of binge frequency on breath alcohol concentrations. However, there was an interaction effect, F(1,28) = 11.26, p < 0.01, with a significant decrease in BrAC over time in the High Frequency binge group but not in the Low Frequency binge group (Figure 1).
Figure 1.

Mean expired breath alcohol levels, before and after behavioral testing, of the 30 participants (15 Low Frequency Bingers, 15 High Frequency Bingers) who received alcohol. * Significant difference pre- vs. post-testing within High Frequency Bingers, p < 0.05
Subjective Effects (VAS)
There were no main effects of binge frequency on any scale. On the impairment scale, mean (± SD) scores after alcohol (60±24 in Low Frequency group, 49±25 in High Frequency group) were significantly greater than scores after placebo (9±9 in Low Frequency group, 24±14 in High Frequency group, F(1,56) = 57.51, p < 0.001. There was a significant binge frequency/dose interaction, F(1,56) = 6.64, p < 0.05, but post hoc analyses found results no different from the main effect of dose. Ratings of confidence in driving were significantly lower after alcohol than after placebo, F(1,56) = 21.94, p < 0.001. There was an interaction of binge frequency and dose, with significantly lower ratings after alcohol vs. placebo only in the Low Frequency binge drinkers, F(1,56) = 4.40, p < 0.05 (Figure 2).
Figure 2.

Participants' responses to Visual Analog Scales administered after alcohol. Among Low Frequency but not High Frequency bingers, confidence in driving was significantly lower after alcohol than after placebo (*p < 0.05).
Simulated Driving
The four most common errors were speed exceedances (40% of errors), speeding tickets (17%), collisions with other vehicles (15%), and centerline crossings (12%). There were neither significant main effects of binge frequency nor interactions of binge frequency and dose on these measures or on driving bonus earned. Alcohol increased collisions with other vehicles, F(1, 55) = 4.48, p < 0.05, and centerline crossings, F(1, 55) = 10.38, p < 0.01, regardless of binge frequency (Figure 3). The main effect of dose on driving bonus earned approached statistical significance, F(1, 55) = 3.56, p = 0.06. That is, across binge frequency conditions, the mean (± SD) driving bonus earned was lower after alcohol ($1.10±$3.95) than after placebo ($3.60±$6.02).
Figure 3.
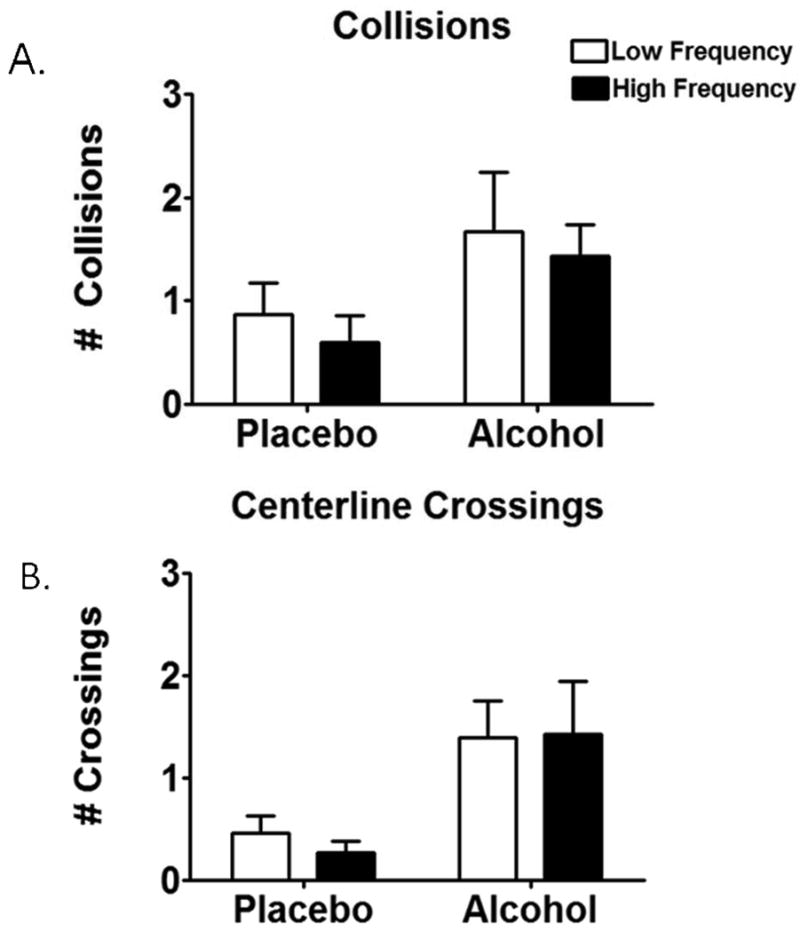
Driving errors after alcohol and placebo. Alcohol increased collisions (A) and centerline crossings (B) in both the High and Low Frequency groups (main effect of alcohol, p < 0.05).
Discussion
This study aimed to clarify the risks of binge drinking by quantifying behavioral differences between High and Low Frequency binge drinkers after an alcohol binge or placebo. The data supported the hypothesis that compared to placebo, High and Low Frequency binge drinkers would make a similar number of errors on a test of simulated driving after an alcohol binge. Furthermore, the Low Frequency group reported feeling less confidence in their simulated driving after alcohol than after placebo. However, contrary to our hypotheses, High Frequency binge drinkers did not report less subjective impairment than Low Frequency bingers after alcohol nor did they report feeling more confident in operating a vehicle.
These findings may have specific relevance to traffic safety, as driving while intoxicated remains a prevalent problem. Compared to Low Frequency bingers who received placebo, Low Frequency bingers who received alcohol reported significantly less confidence in operating a vehicle. However, in High Frequency binge drinkers, there was no significant difference in driving confidence between placebo and alcohol conditions. Given this finding, individuals in the Low Frequency group may have been sensitive to the subjective impairing effects of alcohol and thus reported feeling significantly less confident in operating a vehicle. Conversely, the High Frequency binge drinkers may not be sensitive to the impairing effects at a breath alcohol level of 0.08% that would normally signal an inability to operate a vehicle.
The availability of a $20 driving bonus and time limit served to simulate a rushed commute. Although the time limit may have encouraged speeding, participants were penalized $2 for each error. Thus, while participants in this paradigm may drive in a rushed manner, they must simultaneously drive as safely as possible to avoid being penalized for any errors. Alcohol use is associated with increased driving speed (Stoduto et al., 1993; McGwin and Brown, 1999). However, moderate drinkers administered a dose of alcohol producing a BrAC of 0.08% may display some caution in driving, compared to individuals receiving a lower dose of alcohol (Burian et al., 2002). The present results are consistent with other evidence that binge drinkers underestimate intoxication (Beirness, 1987) and may be more likely than moderate drinkers to choose to drive—and drive rapidly—after drinking.
The discrepancy in reported driving confidence between the High and Low Frequency binge groups after alcohol may be related to differences in breath alcohol levels. Comparisons of the two groups at pre and post-testing (approximately 45 minutes apart) showed no significant change in expired breath alcohol levels for the Low Frequency binge group. The High Frequency group, by comparison, experienced a significant drop from 0.09% mean breath alcohol to 0.07%. These data suggest that the observed decrease in driving confidence in Low Frequency binge drinkers after alcohol may be associated with their sustained breath alcohol from pre to post-testing. In contrast, the High Frequency group's significant drop in breath alcohol levels may account for the lack of significant change in driving confidence between placebo and alcohol conditions. Given that they report greater instances of being drunk (a perceptual state that would normally require a breath alcohol level of 0.08% or above; Kerr et al., 2006) than the Low Frequency group, the High Frequency group may be more tolerant to the impairing effects felt at this level of alcohol intoxication.
Moreover, differences in the frequency of binges between groups may help clarify the dissimilar subjective effects observed after alcohol. Although both the High and Low Frequency groups reported equal weekly alcohol consumption, they are likely consuming the alcohol in different patterns, reflected in the differences in the binge scores between the groups. High Frequency binge drinkers report a greater number of instances drunk in the past 6 months and a higher percentage of instances of drinking to intoxication. It is possible that the Low Frequency group is spreading their alcohol consumption out so that they are consuming moderate levels across several days, while limiting their binge episodes to once per month. These findings support previous research suggesting that the pattern of drinking is important in determining alcohol risk, including driving after drinking (Midanik, 1999; Presley and Pimentel, 2006).
Several limitations of the experimental design warrant discussion. First, we did not recruit a comparison group of males. Binge frequency may not influence the behavioral effects of alcohol in men in the same manner, based on differences in alcohol metabolism that cause females to reach higher breath alcohol levels from consumption of an equal amount of alcohol as men and research that suggests differences in negative behaviors between genders post-alcohol consumption (Kelly-Weeder, 2008). However, a recent study including both genders revealed the same disconnect between subjective intoxication and simulated driving performance when comparing binge and non-binge drinkers (Marczinski and Fillmore, 2009). Future research should compare the behavioral effects of alcohol on males with low and high frequency of binge drinking.
The second limitation involves the alcohol delivery schedule. The current study controlled for the rate and amount of alcohol consumption. Each subject was given 10 minutes to consume the drink, with 20 minutes for absorption before delivery of the next drink. This delivery schedule may not accurately portray the bingeing habits of the subjects, particularly college-aged participants. Other studies acknowledge that college students notably drink well above the NIAAA-defined “binge” threshold by using higher drink-per-session cutoff points to distinguish binge drinkers from social drinkers. These high cutoff points (males/females) include 7/6, 10/8, and 15/12 drinks per occasion (Read et al., 2008; White et al., 2006). Allowing ad libitum consumption of alcohol in a controlled environment may reveal additional group differences, as High and Low Frequency bingers may consume alcohol in a differing manner in an effort to control intoxication level.
Finally, the role of neurobiological effects of binging was not directly quantified in this study. Several studies have suggested that the frequency of binges may lead to alterations in neurobiology and, subsequently, behavior. Repeated exposure to ethanol is associated with a wide range of neurological detriments, most notably of the prefrontal cortex. For example, compared to nonbinge drinkers, binge drinkers have shown impairment on such prefrontal tasks as Tower of London (Hartley et al., 2004), Spatial Working Memory (Townshend and Duka, 2005), and the Iowa Gambling Task (Goudriaan et al., 2007). Thus, differences observed between the High and Low Frequency binge groups may be related to alcohol-induced deficits of the prefrontal cortex.
Conclusion
Longitudinal studies suggest that repeated binges result in deficits in decision making in tasks such as the Iowa Gambling Task (Goudriaan et al., 2007). The present study suggests that these deficits may manifest in instances where individuals choose whether to drive after drinking. The implication is that repeated binge exposure leads to changes in the perception of impairment that would normally signal an inability to drive, while actual behavioral tolerance to alcohol does not develop. This constitutes a hazard not only to the intoxicated drivers, but also to members of the public who may be driving alongside them.
Acknowledgments
This study was supported by National Institute on Alcohol Abuse and Alcoholism grants T32 07565 and P01 17056. The authors report no conflict of interest. All authors contributed to the design, data analysis, and preparation/revision of this manuscript.
References
- Babor TF, Higgins-Biddle JC, Saunders JB, Monteiro MG. The Alcohol Use Disorders Identification Test (AUDIT) Manual. World Health Organization; Geneva: 2001. [Google Scholar]
- Beirness DJ. Self-estimates of blood alcohol concentration in drinking-driving context. Drug Alcohol Depend. 1987;19:79–90. doi: 10.1016/0376-8716(87)90089-5. [DOI] [PubMed] [Google Scholar]
- Brumback T, Cao D, King A. Effects of alcohol on psychomotor performance and perceived impairment in heavy binge social drinkers. Drug Alcohol Depend. 2007;91:10–17. doi: 10.1016/j.drugalcdep.2007.04.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burian SE, Liguori A, Robinson HJ. Effects of alcohol on risk-taking during simulated driving. Hum Psychopharmacol Clin Exp. 2002;17:141–150. doi: 10.1002/hup.384. [DOI] [PubMed] [Google Scholar]
- Chassin L, Pitts SC, Prost J. Binge drinking trajectories from adolescence to emerging adulthood in a high-risk sample: predictors and substance abuse outcomes. J Consult Clin Psychol. 2002;70:67–78. [PubMed] [Google Scholar]
- Dejong W. Definitions of binge drinking. JAMA. 2003;289:1635. doi: 10.1001/jama.289.13.1635. [DOI] [PubMed] [Google Scholar]
- Dimeff LA, Kilmer J, Baer JS, Marlatt GA. Binge drinking in college. JAMA. 1995;273:1903–1904. doi: 10.1001/jama.1995.03520480021022. [DOI] [PubMed] [Google Scholar]
- First MB, Spitzer RL, Gibbon M, Williams JBW. Biometrics Research. New York State Psychiatric Institute; New York: 2001. Structured Clinical Interview for DSM-IV-TR Axis I Disorders, Research Version, Patient Edition (SCID-I/P) [Google Scholar]
- Flowers NT, Naimi TS, Brewer RD, Elder RW, Shults RA, Jiles R. Patterns of alcohol consumption and alcohol-impaired driving in the United States. Alcohol Clin Exp Res. 2008;32:936–644. doi: 10.1111/j.1530-0277.2008.00622.x. [DOI] [PubMed] [Google Scholar]
- Goudriaan AE, Grekin ER, Sher KJ. Decision making and binge drinking: a longitudinal study. Alcohol Clin Exp Res. 2007;31:928–938. doi: 10.1111/j.1530-0277.2007.00378.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ham LS, Hope DA. College students and problematic drinking: a review of the literature. Clin Psychol Rev. 2003;23:719–759. doi: 10.1016/s0272-7358(03)00071-0. [DOI] [PubMed] [Google Scholar]
- Hartley DE, Elsabough A, File SE. Binge drinking and sex: effects on mood and cognitive function in healthy young volunteers. Pharmacol Biochem Behav. 2004;78:611–619. doi: 10.1016/j.pbb.2004.04.027. [DOI] [PubMed] [Google Scholar]
- Herring R, Berridge V, Thom B. Binge drinking: an exploration of a confused concept. J Epidemiol Community Health. 2008;62:476–479. doi: 10.1136/jech.2006.056721. [DOI] [PubMed] [Google Scholar]
- Hindmarch I, Kerr JS, Sherwood N. The effects of alcohol and other drugs on psychomotor performance and cognitive function. Alcohol. 1991;26:71–79. [PubMed] [Google Scholar]
- Kelly-Weeder S. Binge drinking in college-aged women: framing a gender-specific prevention strategy. J Am Acad Nurse Pract. 2008;20:577–584. doi: 10.1111/j.1745-7599.2008.00357.x. [DOI] [PubMed] [Google Scholar]
- Kerr WC, Greenfield TK, Midanik LT. How many drinks does it take you to feel drunk? Trends and predictors for subjective drunkenness. Addiction. 2006;101:1428–1437. doi: 10.1111/j.1360-0443.2006.01533.x. [DOI] [PubMed] [Google Scholar]
- Marczinski CA, Harrison EL, Fillmore MT. Effects of alcohol on simulated driving and perceived driving impairment in binge drinkers. Alcohol Clin Exp Res. 2008;32:1329–1337. doi: 10.1111/j.1530-0277.2008.00701.x. [DOI] [PubMed] [Google Scholar]
- Marczinski CA, Fillmore MT. Acute alcohol tolerance on subjective intoxication and simulated driving performance in binge drinkers. Psychol Addict Behav. 2009;23:238–247. doi: 10.1037/a0014633. [DOI] [PubMed] [Google Scholar]
- McGwin G, Brown D. Characteristics of traffic crashes among young, middle-aged, and older drivers. Accid Anal Prev. 1999;31:13–30. doi: 10.1016/s0001-4575(98)00061-x. [DOI] [PubMed] [Google Scholar]
- Mehrabian A, Russell JA. A questionnaire measure of habitual alcohol use. Psychol Rep. 1978;43:803–806. doi: 10.2466/pr0.1978.43.3.803. [DOI] [PubMed] [Google Scholar]
- Midanik LT. Drunkenness, feeling the effects and 5+ measures. Addiction. 1999;94:887–897. doi: 10.1046/j.1360-0443.1999.94688711.x. [DOI] [PubMed] [Google Scholar]
- Naimi TS, Brewer RD, Mokdad A, Denny C, Serdula MK, Marks JS. Binge drinking among US adults. JAMA. 2003;289:70–75. doi: 10.1001/jama.289.1.70. [DOI] [PubMed] [Google Scholar]
- National Highway Traffic and Safety Administration . 0.08 BAC Illegal Per Se Level. U.S. Department of Transportation, National Highway Traffic and Safety Administration; Washington, DC: 1998. [Google Scholar]
- NIAAA council approves definition of binge drinking. 2004. [Google Scholar]
- Perkins HW. Surveying the damage: a review of research on consequences of alcohol misuse in college populations. J Stud Alcohol Suppl. 14:91–100. doi: 10.15288/jsas.2002.s14.91. [DOI] [PubMed] [Google Scholar]
- Presley CA, Pimentel ER. The introduction of the heavy and frequent drinker: a proposed classification to increase accuracy of alcohol assessments in postsecondary educational settings. J Stud Alcohol. 2006;67:324–331. doi: 10.15288/jsa.2006.67.324. [DOI] [PubMed] [Google Scholar]
- Psychological Corporation . Wechsler Abbreviated Scale of Intelligence (WASI) Manual. The Psychological Corporation; San Antonio, TX: 1999. [Google Scholar]
- Quinlan KP, Brewer RD, Siegel P, Sleet DA, Mokdad AH, Shults RA, Flowers N. Alcohol-impaired driving among U.S. adults, 1993-2002. Am J Prev Med. 2005;28:346–350. doi: 10.1016/j.amepre.2005.01.006. [DOI] [PubMed] [Google Scholar]
- Read JP, Beattie M, Chamberlain R, Merrill JE. Beyond the “Binge” threshold: heavy drinking patterns and their association with alcohol involvement indices in college students. Addict Behav. 2008;33:225–234. doi: 10.1016/j.addbeh.2007.09.001. [DOI] [PubMed] [Google Scholar]
- Stoduto G, Vingilis E, Kapur BM, Sheu WJ, McLellan BA, Liban CB. Alcohol and drug use among motor vehicle collision victims admitted to a regional trauma unit: Demographic, injury, and crash characteristics. Accid Anal Prev. 1993;25:411–420. doi: 10.1016/0001-4575(93)90070-d. [DOI] [PubMed] [Google Scholar]
- Townshend JM, Duka T. Patterns of alcohol drinking in a population of young social drinkers: a comparison of questionnaire and diary measures. Alcohol. 2002;37:187–192. doi: 10.1093/alcalc/37.2.187. [DOI] [PubMed] [Google Scholar]
- Townshend JM, Duka T. Binge drinking, cognitive performance and mood in a population of young social drinkers. Alcohol Clin Exp Res. 2005;29:317–325. doi: 10.1097/01.alc.0000156453.05028.f5. [DOI] [PubMed] [Google Scholar]
- Wechsler H, Davenport A, Dowdall G, Moeykens B, Castillo S. Health and behavioral consequences of binge drinking in college. A national survey of students at 140 campuses. JAMA. 1994;272:1672–1677. [PubMed] [Google Scholar]
- Wechsler H, Dowdall GW, Maenner G, Gledhill-Hoyt J, Lee H. Changes in binge drinking and related problems among American college students between 1993 and 1997. Results of the Harvard School of Public Health College Alcohol Study. J Am Coll Health. 1998;47:57–68. doi: 10.1080/07448489809595621. [DOI] [PubMed] [Google Scholar]
- Wechsler H, Lee JE, Kuo M, Lee H. College binge drinking in the 1990s: a continuing problem. Results of the Harvard School of Public Health 1999 College Alcohol Study. J Am Coll Health. 2000;48:199–210. doi: 10.1080/07448480009599305. [DOI] [PubMed] [Google Scholar]
- Wechsler H, Lee JE, Kuo M, Seibring M, Nelson TF, Lee H. Trends in college binge drinking during a period of increased prevention efforts. Findings from 4 Harvard School of Public Health College Alcohol Study surveys: 1993-2001. J Am Coll Health. 2002;50:203–217. doi: 10.1080/07448480209595713. [DOI] [PubMed] [Google Scholar]
- Wechsler H, Nelson TF. Relationship between level of consumption and harms in assessing drink cut-points for alcohol research: Commentary on “Many college freshmen drink at levels far beyond the binge threshold” by White et al. Alcohol Clin Exp Res. 2006;30:922–927. doi: 10.1111/j.1530-0277.2006.00124.x. [DOI] [PubMed] [Google Scholar]
- White AM, Kraus CL, Swartzwelder H. Many college freshmen drink at levels far beyond the binge threshold. Alcohol Clin Exp Res. 2006;30:1006–1010. doi: 10.1111/j.1530-0277.2006.00122.x. [DOI] [PubMed] [Google Scholar]
- Witt ED. Puberty, hormones, and sex differences in alcohol abuse and dependence. Neurotoxicol Teratol. 2007;29:81–95. doi: 10.1016/j.ntt.2006.10.013. [DOI] [PubMed] [Google Scholar]