

Abstract
The study of anatomy in England during the 18th and 19th century has become infamous for bodysnatching from graveyards to provide a sufficient supply of cadavers. However, recent discoveries have improved our understanding of how and why anatomy was studied during the enlightenment, and allow us to see the context in which dissection of the human body took place. Excavations of infirmary burial grounds and medical school cemeteries, study of hospital archives, and analysis of the content of surviving anatomical collections in medical museums enables us to re-evaluate the field from a fresh perspective. The pathway from a death in poverty, sale of the corpse to body dealer, dissection by anatomist or medical student, and either the disposal and burial of the remains or preservation of teaching specimens that survive today in medical museums is a complex and fascinating one.
Keywords: anatomy, body snatching, dissection, enlightenment, medical history
Introduction
In the late mediaeval period anatomical knowledge in Britain and Europe was largely based on manuscripts from classical Greece and mediaeval Italy, the dissection of animals such as pigs, and the intermittent dissection of a condemned criminal (Park, 1994; Olry, 1997; French, 1999). However, by the 17th century, the situation changed as printed books of anatomical texts from Italy and France became more widely available (Vesalius, 1543; Cunningham, 1997). Judges passing sentences on criminals could recommend anatomical dissection after their death from hanging (Bailey, 1989, p. 22; Richardson, 2001, p. 32) and William Harvey (1578–1657) performed many dissections on hanged criminals in London (Payne, 2002). Following the Murder Act of 1752, the Company of Surgeons in London was obliged to conduct public dissections of convicted murders, and to expose the corpse to general view (Anonymous, 1752). By the 18th century, charitable hospitals were being set up across Britain to care for the poor who became sick (Woodward, 1974). Closely associated with many of these charitable hospitals were the independently run anatomy schools, where those training in anatomy and surgery dissected human cadavers (Cope, 1961, p. 62–86; Knapman, 1999–2000; Richardson, 2001, p. 287) (Fig. 1).
Fig. 1.
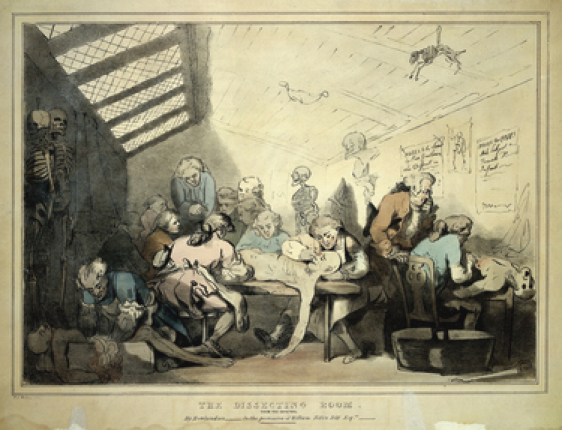
The interior of a dissecting-room, probably based on that of William Hunter, ca. 1780. Lithograph after an original drawing by Thomas Rowlandson. Wellcome Library, London.
Sourcing cadavers for anatomical dissection
Hardly any of the bodies needed for dissection were voluntarily donated for this purpose. While criminals hung for murder were available for anatomical dissection, even by the 17th century there were not enough eligible hangings to accommodate the demand for bodies. For example, in 1636 a charter of King Charles expanded the number of hanged criminals available for dissection at Oxford University from those who died within the city to those hung within 21 miles of Oxford (Sinclair & Robb-Smith, 1950, p. 2). In the 18th century there was major concern amongst the general public about crime increasing, due to regular newspaper coverage. The government's response was to increase the number of crimes punished by hanging to over 200 separate offences. However, there was reluctance to execute more than a few as examples, so the number of executed criminals actually declined. By the early 19th century, 90% of those sentenced to death later had their sentences reduced (Hitchcock & Shoemaker, 2006, p. 238). There were often fights and sometimes riots when family and friends of the deceased tried to prevent the delivery of corpses from the scaffold to the anatomists, such as the Tyburn riot of 1749 (Linebaugh, 1975). In the 18th century a good proportion of the required cadavers were exhumed during the night from churchyards by men known as resurrectionists, who sold them on to the anatomy schools (Durey, 1976; Bhanji, 1995; Burch, 2007).
The expansion in anatomical and medical training continued into the 19th century. Many surgeons were required by the army and navy for the Napoleonic wars in the first two decades of the century, and private medical schools reached their zenith in the third decade with at least 10 founded outside London between 1824 and 1834 (Loudon, 1986, p. 49). Prior to 1832 the relative shortage of bodies for the number of anatomists and medical students meant that corpses were always in demand, and the trade in body snatching was lucrative. Occasionally, as with the infamous case of Burke and Hare in Edinburgh, people were murdered for the value of their corpse (Townsend, 2001). It was argued at the time that it was better to use corpses for dissection than for the living to suffer the consequences of ignorant doctors, and that using unclaimed bodies for dissection would prevent grave robbing (Southwood-Smith, 1824). In 1828 the Report from the Select Committee on Anatomy suggested that there were around 800 students at medical schools in London, of whom around 500 practised dissection (Bailey, 1896). There were apparently around 450–500 corpses available to them each year, so clearly a significant demand. Following the Anatomy Act of 1832 (Anonymous, 1832), body snatching from graves became unnecessary, as the dead bodies of all unclaimed poor from workhouses and charitable hospitals could legally undergo dissection. In fact, one of the principal reasons for introducing the Act was to prevent body snatching from graves. This practice continued throughout the century, and even in the late 19th century those running poor houses could sell corpses of their unclaimed inmates after death to teaching hospitals to recoup the expenses of poor relief in their parish (Hurren, 2007, p. 192). Other corpses were sold directly by desperately poor and grieving relatives to corpse dealers who worked in deprived areas of cities. Some corpses were sold on whole to the anatomy schools, but a higher price could be obtained by dividing up the body into its constituent parts to sell separately. Attitudes to the practice of dissection varied significantly between the rich and the poor. The wealthy who determined the law were happy for dissection to continue because scientific research was regarded as worthy at that time. Furthermore, it was not the rich who were dissected but the poor, either voluntarily when a corpse was sold by a desperately poor family, or against their wishes when death occurred in the workhouse or a charitable hospital and the body was unclaimed (Richardson, 2001, p. 221).
Between the 1820s and the 1860s there was a dramatic shift in the provision of anatomical teaching, from the dominance of the independent anatomical schools to the hospital medical schools. In 1826 there were eight independent anatomy schools and just four hospital anatomy schools in London. By 1871 there were 11 hospital anatomy schools and no independent schools still in existence (Richardson, 2001, p. 287). With the rise of the medical schools, the independent anatomy schools either merged with the local voluntary hospitals or went out of business (Durey, 1976). They then sold their collections at auction to the interested general public, to the Royal College of Surgeons, or to the medical schools themselves.
Archaeological evidence for dissection
Recent excavation of pauper hospital burial grounds, workhouse cemeteries, and the refuse dumps of institutions teaching anatomy in the 18th century and 19th century have demonstrated how these dissections took place. The vast majority of these discoveries have never been published before.
The former Newcastle Infirmary was founded in 1751 to treat the poor of Newcastle upon Tyne, Northumberland and Durham, and patients were admitted from 1753 (Miller, 1986). It initially had 90 beds, expanded in size twice during the 19th century, and then finally closed as a hospital in 1906. Doctors working in the infirmary were accompanied by students who paid to watch and learn the art of medicine. Infirmaries such as this were funded by wealthy philanthropists to provide some level of medical care to the poor who were unable to afford it themselves (Porter, 1989). Restrictions upon entry included children under 7 years old, pregnant women, the mentally ill, certain infectious diseases, and cancers that science of the time could not cure. The infirmary's burial ground was excavated in 1996, and produced extensive evidence of dissection, autopsies and the use of cadavers in the teaching of surgical techniques (Chamberlain, 1999; Start, 2002). The excavations revealed a total of 210 articulated skeletons together with charnel deposits containing the disarticulated skeletal remains of a further 407 individuals. Although the infirmary burial ground had been used for unclaimed deceased patients from 1753, it had been closed to further interments in 1845 (Miller, 1986).
Evidence for post-mortem dissection and autopsy included 61 craniotomies, transected clavicles and ribs from thoracotomy procedures, and transection of the spine in the sagittal plane (Chamberlain, 1999; Start, 2002). Craniotomy was noted in 11% of skulls from articulated burials and 18% of skulls from disarticulated burials. The osteotomy had been performed using a hand saw, as indicated by the markings on the cut bone edges, perhaps guided by a metal brace clamped to the cranial vault. Thoracotomies were performed by sawing through the midshaft of both clavicles, and cutting through the ribs of both hemithoraces. The fact that a midline cut through the sternum was not performed, and bilateral osteotomies in the mid-clavicular plane preferred, suggests that the sternum and anterior part of the ribs were probably removed to visualise the thoracic organs. In four instances saw cuts were noted through the thoracic and lumbar vertebral and the pelvis in the sagittal plane, suggesting these individuals had been prepared as prosection specimens (Fig. 2). Twenty-one further disarticulated bones also showed evidence of similar saw cuts. The burial of some disarticulated bone within regular graves inside the burial ground shows that some effort had been made to dispose carefully of dissected remains, probably to avoid drawing unwanted attention to a clandestine activity. Some burials comprised body parts of different individuals in the coffin, and one upper torso was buried with a paving slab in the lower part of the coffin, presumably to approximate the weight and balance of a complete corpse in the coffin.
Fig. 2.

Sacrum and lumbar vertebrae from the Newcastle Infirmary burial ground, transected in the sagittal plane suggesting their earlier use in anatomical dissection.
Bones from 200 amputated limbs in commingled charnel pits, mainly distal limb segments discarded after successful surgery, were studied to determine the nature of surgical procedures. In several instances it could be demonstrated that the amputations were performed as training exercises using cadavers, rather as a treatment for disease in living individuals. In some there were multiple parallel saw cuts through the bones, and in one instance multiple amputations involving different limbs of the same cadaver that also had craniotomy and thoracotomy cuts. Although few of the burials can be dated precisely, it is clear that much of the evidence for anatomical dissection at the Newcastle Infirmary is likely to pre-date the passing of the Anatomy Act of 1832, as the cemetery was not used after 1845.
Oxford Castle served as the county prison for much of the post-mediaeval period, and public hangings were carried out at the gallows in front of the prison. Prior to the passing of the Anatomy Act of 1832, the bodies of executed felons were the only legally acquired cadavers available to anatomists for dissection. Marked antipathy to dissection was widespread at this time, and a number of historical accounts describe the Oxford Castle gallows as being the site of violent struggles between relatives and body dealers for possession of the corpse following a hanging. Many such criminals did undergo dissection nevertheless, principally those guilty of murder, but at least three of theft (Davies, 2005). However, they were never in sufficient numbers to adequately supply the needs of the Oxford University medical school. The university was responsible for providing the dissected with decent burials (Sinclair & Robb-Smith, 1950), and it would appear that many such individuals were returned to Oxford Castle for burial. A good deal of anatomical research was undertaken during the 16th and 17th centuries at Oxford based in part on these dissections. Thomas Willis wrote the neuroanatomy work Cerebri Anatome, illustrated by Christopher Wren (Willis, 1664). William Harvey worked here, as did George Joyliffe, who discovered the lymphatic system, and Richard Lower, who dissected the heart, discovered the colour change in blood passing through the lungs from its contact with the air, and undertook an early blood transfusion (Sinclair & Robb-Smith, 1950, p. 14).
In 2002, Oxford Archaeology undertook extensive excavation within the castle precincts in advance of redevelopment. Sixty-two burials were discovered in the backfill of the moat of the Norman motte. The majority were adolescent or young adult males, and many had been buried within plain undecorated wooden coffins. They are believed to be the remains of executed criminals and prisoners who had died at the castle. Dating is uncertain but ranges from the 16th to early 19th centuries, with the bulk probably dying in the late 17–18th centuries. Osteological evidence for dissection was found in at least five skeletons. Two had undergone craniotomy, with saw cuts being symmetric and neatly made. In both cases, further vertical cuts extended distally from the craniotomies giving access to the middle ear and other structures of anatomical interest. Fine cut marks over the scalp were compatible with the removal of muscles from the cranium. In various individuals such cuts were also noted at the temporomandibular joint, scapula, cervical spine or limbs. One had been decapitated through the cervical spine with a saw. Several of these skeletons were incomplete, suggesting that their dissected limbs were buried elsewhere, perhaps if dissected at a different time to the head. Some dissected human remains from Oxford Castle were not reburied at all, however, but were retained as specimens for teaching or display. One such skeleton that was articulated for display is that of Giles Covington, executed at Oxford Castle for murder in 1791, and is currently on display in the Museum of Oxford.
The workhouse on Rats and Mice Hill in Oxford was excavated in 1994. The institution was built in 1771, was in use throughout the 19th century, and often held over 200 poor and destitute (Crossley et al. 1979). Due to disturbance of burials in modern times it has not been possible to determine how many people were originally buried there. However, eight individuals were recovered that did show evidence of anatomical dissection. One of these was a child and the rest adults. All but two had craniotomies, and there were cut marks on the skulls, vertebrae and elsewhere. This demonstrates how a proportion of those who died at the workhouse were taken for dissection, presumably at the university, and their remains later returned to the workhouse cemetery for burial. In view of the historical evidence, it is presumed that these individuals were dissected after the Anatomy Act of 1832.
The Old Ashmolean Museum in Oxford was the location of anatomical dissections held in its basement from 1683 (Hull, 2003). Dissection was undertaken there throughout the late 17th and early 18th centuries, despite complaints from readers in the adjacent Bodleian Library who objected to the smells of the decomposing corpses (Sinclair and Robb-Smith, 1950, p. 21). In later times the Museum of the History of Science was located there, and in 1999 Thames Valley Archaeological Services (TVAS) performed excavation prior to renovation works at the museum. Chemistry equipment including crucibles and other earthenware vessels, dating from the late 17th to early 18th centuries, were recovered alongside a considerable amount of bone. The human osteoarchaeologist Bill White identified over 26 kg of disarticulated human bone, comprising 2050 skeletal elements and representing a minimum number of individuals numbering 18. There was also a large amount of animal bone recovered, including the skeletal remains of 24 dogs. This dump is thought to be the consequences of a spring-cleaning event in 1781, when the basement changed use from anatomical dissection room to a new chemistry laboratory (Bennett et al. 2000; Hull, 2003). The contents of the dump suggest that the university students were dissecting both humans and dogs in order to learn their anatomy.
London has provided good archaeological evidence for anatomical dissection and medical training during the 18th century and 19th century on a unique scale. In the summer of 2006, Museum of London Archaeology (MOLA) undertook excavation within the grounds of the Royal London Hospital, Whitechapel, East London. Construction of this hospital began in 1752, and the premises were opened in 1757 (Clark-Kennedy, 1962, p. 123–135). There is compelling textual evidence for the scale and process of dissection at the Royal London Hospital in the 1820s from the accounts of Ann Millard, wife of a ‘Resurrection Man’. William Millard was apprehended in the London Hospital burial ground in dubious circumstances, and later died in Coldbath Fields prison from a fever. Ann wrote of the regular disinterment of patients by her husband for dissection at the school, and also for sale to other anatomists (Millard, 1825). Dated plans of the hospital show that the archaeologically recovered human remains in this particular area date to around 1825–54. This time period also spans the introduction of the Anatomy Act. The skeletal remains appear to be derived from a combination of anatomical dissection of corpses for research and teaching, autopsy to identify the cause of death, and surgery carried out while the patients were alive.
Of the 273 graves excavated, 144 coffins contained body portions from numerous individuals (at present, a maximum of 500 individuals is postulated). There was a preponderance of men but women and children had also been dissected, including a very small number of neonates/foetal remains. Evidence for dissection included craniotomies, vertebral transection at the neck or lumbar spine as if to divide the corpse into separate sections, pelvic hemisection in the sagittal plane, and thoracotomies performed with clavicle and rib transactions. Some coffins contained dissected animals, such as dogs, rabbits, cats, cattle and horses. They also included exotic species such as two tortoises and two mona monkeys, which are native to sub-Saharan Africa. Dissection of different species to study comparative anatomy was popular at that time (Richardson, 2008). The animal dissections were noted to have saw cuts in very similar positions to those found in the human skeletons, highlighting the quest to understand comparative anatomy at that time.
In some cases the human remains clearly formed part of a preserved teaching collection. A number of bones were held in reasonable anatomical alignment by copper alloy wires and iron pins, suggesting their prior use in anatomical teaching. Several skulls had red staining at the location where soft tissue structures lay during life, showing that the red dye had probably been painted on the bone for anatomical teaching purposes. Blood vessels had been cast in wax and fragments found in at least seven different coffins. This demonstrates the early use of wax casts to highlight the anatomy of hollow soft tissue structures such as blood vessels for teaching purposes.
These archaeological excavations at Newcastle, Oxford and London give evidence from a perspective quite different from those of the written texts. They provide physical evidence of what was actually done, in contrast to the texts that describe the author's experiences or the public perception of dissection. Saw marks demonstrate where the skull, spine and limbs were divided and allocated to different students, while cut marks on bone from knives show how the soft tissue was removed. In consequence, the eventual burial often involved a non-matching combination of torso and limbs placed together in a coffin. Practice operations were also noted at a number of medical schools across the country, with multiple cranial trepanations and serial amputations of the same limb at slightly different heights. This tangible evidence provides a vivid image of what it must have been like to cut up a corpse in order to study its constituent parts.
Anatomical collections in museums
Specimens of anatomy or pathology obtained from these dissections and thought to be of special interest by these anatomists were preserved in teaching collections and became the core of the various royal college and medical school collections preserved today in Britain (Richardson, 2000). Medical museums gave credibility to individuals and institutions and were perceived to indicate expertise. The larger the collection, the greater the perceived expertise. In early collections, curiosities made up the majority of specimens (Alberti, 2011). However, when doctors realised the importance of correlating symptoms with anatomical lesions during autopsy, normal anatomy and more common pathological specimens were added to these collections (Reinarz, 2005).
One of the most famous of the collectors of anatomical specimens during the enlightenment was John Hunter (1728–93) (Chaplin, 2005, 2008). In 1788, a correspondent to London's General Evening Post reported that ‘Mr John Hunter opened his very curious, extensive and valuable museum’ to ‘a considerable number of the literati’ (Chaplin, 2008). His museum (Fig. 3) was an extraordinary collection of over 13 000 preparations of human and animal anatomy and pathology built up over the course of Hunter's 30-year career as London's leading practitioner of dissection. It was located within his own home/anatomy school in Leicester Square in central London, and remained open to the public until his death in 1793. In the eyes of the non-medical spectator, the ranks of anatomical specimens in Hunter's museum invited neither distaste, nor disquiet, but instead served as a physical manifestation of ‘Mr Hunter's genius and ardent zeal in his profession’. The relationship between the practice of human dissection and the manufacture, accumulation and display of the preserved parts of human bodies in late 18th century London is fascinating. Study of the ‘anatomical museum’, and relating it to the specific sites in which dissection was performed and preparations manufactured and exhibited, allows us not only to demonstrate the crucial role of these museums in London's rising prominence as a centre for anatomical teaching, but also to situate them within broader histories of the museum and of anatomy (MacGregor, 2007; Cunningham, 2010).
Fig. 3.
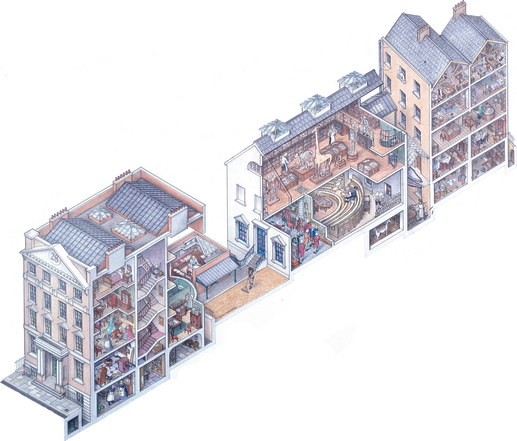
Reconstruction of the interior of John Hunter's house and anatomy school in Leicester Square, London, ca. 1790, by John Ronayne (2005). The Royal College of Surgeons of England.
There was an extraordinary degree of investment, both economic and epistemic, made in such museums by a range of practitioners linked to the teaching of anatomy, surgery and midwifery in London between the early 1750s and the end of the century. Despite the considerable attention paid to the development of London as a centre for medical education in this period (Lawrence, 1996), the importance of what can be termed a ‘museum economy’ to dissection-based teaching and research has been largely overlooked. John Hunter and his brother, the anatomist and man-midwife William Hunter, are the best-known members of Georgian London's circle of extra-mural anatomy teachers and are the only ones whose collections have survived, respectively, at the Royal College of Surgeons in London and the University of Glasgow (Anonymous, 1830–31; Marshall, 1970). However, there is ample evidence to suggest that their work as collectors and exhibitors was mirrored by contemporaries such as John Sheldon, John Heaviside and Joshua Brookes (Chaplin, 2008). Their collections served as valuable resources for teaching and research, and the didactic value of their museums was heavily promoted in adverts and prospectuses for their courses (e.g. Perry, 1782). Yet the sheer scale of their collections, the costs involved in their maintenance and care, and the zeal applied the preparation and display of preparations suggest that these museums were not solely seen as assets connected to the business of teaching, or as spaces for research. Instead, the example of John Hunter points to a further and important role for the anatomical museum as a ‘public’ space within the ‘private’ anatomy schools of Georgian London (Chaplin, 2005; Alberti, 2007).
Rackstrow's Museum was a commercial institution functioning in the late 18th century. Benjamin Rackstrow (1707–72) was a showman who put together the museum in Fleet Street in London. It included displays of preserved human organs and wax anatomical models for the general public to view for a fee. After Rackstrow's death in 1772 it was run by a midwife named Catherine Clark and her son Benjamin, who was a surgeon who had trained with John Hunter (Craske, 2010).
Joshua Brookes was a former student of John Hunter who established an anatomical museum in Great Marlborough Street in the mid 1780s. It was said by visitors to rank second only to that of John Hunter in terms of scale (Jerdan, 1834, p. 8). The museum was open not only to his students, scientific foreigners and private gentlemen, but also to the general public at least on the Saturday of every month. It contained over 6000 anatomical preparations of human and animal specimens, including elephants, rhinos and hippos in the comparative osteology collection.
John Heaviside's museum was located behind his house in Hanover Square in London (Peachey, 1931). He was a surgeon who was able to purchase the anatomical collections of others with the inheritance left to him when his father died. He regularly opened his collection to medical guests and ‘respectable strangers’, and although he never taught the subject the museum gained him a reputation as an anatomist. One consequence of this was his election to the Royal Society in 1797. This shows how the display of anatomical collections was perceived as a sign of scientific authority at the national level.
St. Bartholomew's Hospital, founded in 1123, was reputedly the first hospital in London to establish a medical museum, in contrast to the privately owned anatomical collections that preceded it. The earliest reference to a museum was in 1726 when the hospital governors provided a room to serve as a repository for anatomical and surgical preparations that were put in charge of the hospital's surgeon, John Freke (1688–1766) (Medvei & Thornton, 1974). The original collection was small and largely comprised urinary calculi. Most of the specimens in the museum were obtained directly from the hospital, but others were donated as individual specimens or as a collection. In 1828 the Medical College of St. Bartholomew's Hospital acquired the personal collection (amounting to several thousand specimens) of John Abernethy (1764–1830). Abernethy was lecturer in anatomy and surgery there from 1788–1829, and founder of Barts Medical College (Medvei & Thornton, 1974; Waddington, 2003). The prime function of the museum was for teaching, and its development owed much to Abernethy's work. The obstetric section of the museum expanded when John Conquest and James Matthews Duncan, both lecturers on midwifery, presented their collections of obstetric specimens to the museum in 1829 and 1879 (Medvei & Thornton, 1974).
The London Infirmary (later to evolve into the Royal London Hospital) was founded in 1740 as a charitable hospital for the poor and destitute sick. In 1746 the House Committee of the hospital decreed that ‘a room be built in order to open such extraordinary bodies as are directed by the physicians’ (Royal London Hospital Archives, 1746). This dissection room seems to have been for staff education, to view both normal anatomy and also pathology. Later, at the London Hospital Medical College, founded in 1785, Sir William Blizard, who co-founded the college, maintained a museum collection of anatomical and surgical specimens for the education of his pupils (Auden, 1978). However, these were subsequently placed at the College of Surgeons and no permanent collection was assembled until 1853, when Sir Andrew Clark (1826–93) was appointed Curator of the Museum (Nunn, 1975). A new medical school building in Turner Street opened in 1854 and included a museum. The collection subsequently developed under the curatorship of the Henry Gawen Sutton (ca. 1836–91) and Sir Jonathan Hutchinson (1828–1913). During the 1880s the museum had both an anatomical and pathological curator and was managed by a Library and Museum Committee (London Hospital Medical College Board, 1880–96). The surgeon Sir Frederick Treves (1853–1923), as anatomical curator, developed the museum's collection of anatomical models, acquiring wax models from France and, as Prosector of London Zoo, donated various zoological specimens for use in comparative anatomy (Trombley, 1989).
Medical museums were also set up in the provinces, the Birmingham School of Medicine being a good example. The anatomical collections facilitated the recognition of courses at the school by members of the London examination bodies. After 1832 the museum was opened to the public to allay their fears as to how an anatomical museum could be of benefit to society. The museum also assisted in the transformation of the medical school into a university, as such museums were perceived to indicate academic excellence, teaching expertise, and authority (Reinarz, 2005). The museum was not just a place for teaching anatomy and pathology, but also a badge that stated the importance of an institution.
Preservation of specimens
The development of techniques for the preservation of specimens in museums was a complex learning curve. In most museums across Europe in the 17th century anatomical specimens in cabinets were generally dried. At Leiden in the Netherlands there were attempts in the mid 17th century to preserve the soft tissues with oils and resins to mimic Egyptian mummies, known as balsaming. By the 1660s the Dutch were also experimenting with the use of wax to inject organs to preserve their structure before the tissue decomposed (Haviland & Parish, 1970; Cook, 2002). Initially, the wax was injected to keep the organ's shape once it had dried. Later red, yellow and green dyes were added to the wax to allow better perception of different anatomical structures. Mercury was also injected into fine vessels and lymphatics to demonstrate the anatomy for the purposes of research and teaching, but this was not used to preserve them. By the 1770s John Hunter was using spirit to preserve soft tissue specimens. John Sheldon (1752–1808) dried specimens and made them transparent with turpentine to see the mercury injections on the blood vessels more clearly. Mercury injection of blood vessels started to go out of fashion by the 1790s when longer-lasting wax injections had improved in quality (Cole, 1921).
Manuals were published in England explaining how to preserve anatomical specimens for display in museums. Thomas Pole published The Anatomic Instructor in 1790 (Pole, 1790). This explained in detail how to dry specimens, and also how to preserve soft tissue organs in spirits of wine and turpentine. These could then be suspended in glass jars using thread attached to the lid of the jar. The techniques for injecting coloured wax or mercury for anatomic research and teaching students was also detailed. This ties in well with the archaeological evidence for the use of wax injections in the first half of the 19th century at the Royal London Hospital outlined earlier. The Anatomic Instructor also described how wax or plaster models could be made of organs that did not preserve well. Dry bone specimens were prepared by boiling the corpse to remove the soft tissues, following by cleaning and whitening of the bones. He recommended that this was performed either by boiling the bones in pearl-ash solution or leaving them on the seashore (Pole, 1790, p. 148). In the mid 19th century larger specimens and indeed whole bodies were being preserved by a combination of injections and soaking. In one described method the hollow organs and vessels of the dissected preparation were injected with volatile oils, balsams and resin dissolved in alcohol. The preparation was then soaked in a solution of oxymuriate of mercury and spirits of wine for 15 days, and then painted with varnish (Gannal, 1840, p. 147).
Some organs remained particularly challenging to preserve with their natural appearance. In the 1860s at Moorfields Eye Hospital in London, eyes were preserved in their museum with spirit, but this caused them to shrink and rendered transparent parts opaque. The alternative was to preserve them in glycerine, which preserved their transparency but caused them to swell. The introduction of formaline by Leber in 1894 solved this problem by preserving specimens while hardening the eye and still maintaining the colour present during life (Collins, 1929).
Ongoing research on specimens and catalogues from the museums of the Westminster Hospital, Old Charing Cross Hospital and St. Mary's Hospital in London is attempting to establish the constituents of mounting fluid of these teaching specimens from the 1880s to the beginning of the 20th century and how these mounting fluids would have affected the final preparation. Evidence so far suggests that methylated spirit was used as a fixative and a preservative agent until the 1890s when formalin became preferred, and this was then superseded by Kaiserling solution in the late 1890s (Pulvertaft, 1950; Proger & Chambers, 1963).
Conclusion
Anatomy was a key area of scientific investigation in Britain during the enlightenment. Anatomists dissected humans and animals to improve the understanding how the human body worked and how it differed from other species on earth. One of the main sources of income for anatomists was from the teaching of anatomy to medical students, and so private anatomy schools flourished in the 18th century. By the 19th century medical schools taught anatomy themselves and many anatomy specimens were transferred to the museums of these medical schools and the royal colleges, where they remain today. The way in which anatomical specimens were obtained for teaching and research during the 18th and 19th centuries has become infamous. Archaeological evidence, historical descriptions of these dissections, records in hospital archives, artwork depicting dissection at that time, newspaper stories, court case records of body snatchers, and museum catalogues all allow us to construct a vivid picture of how anatomical research and training took place during the enlightenment up to the dawn of the 20th century.
Acknowledgments
We are grateful to Ashgate Publishing for allowing us to print ideas here that are explored in greater detail in the forthcoming book Anatomical Dissection in Enlightenment Britain and Beyond: Autopsy, Pathology and Display (P. D. Mitchell, editor; Aldershot: Ashgate Publishing, in press). MOLA would like to thank Skanska Innisfree for providing funding for the Royal London Hospital project.
Authors' contributions
Mitchell initiated the project, co-ordinated the contributions and edited the text. Boston, Chamberlain, Fowler, Powers, Walker, Webb and Witkin undertook the archaeological research. Chaplin, Chauhan, Evans and Mitchell undertook the historical research.
References
- Alberti S. The museum effect: visiting collections of anatomy and natural history in Victorian Britain. In: Fyfe A, Lightman B, editors. Science in the Marketplace: Nineteenth-Century Sites and Experiences. Chicago: University of Chicago Press; 2007. pp. 371–403. [Google Scholar]
- Alberti S. Medical museums past, present and future. Bull R Coll Surg Engl. 2011;93:56–58. [Google Scholar]
- Anonymous . A Bill, Entituled an Act for Better Preventing the Horrid Crime of Murder. London: 1752. [Google Scholar]
- Anonymous . Catalogue of the Hunterian Collection of the Royal College of Surgeons of London. London: R. Taylor; 1830. –31. [Google Scholar]
- Anonymous . An Act for Regulating Schools of Anatomy, Anno Secundo & Terio Gulielmi IV. Regis. Cap LXXV. London: 1832. [Google Scholar]
- Auden RR. A hunterian pupil: Sir William Blizard and the London Hospital. Ann R Coll Surg Engl. 1978;60:345–349. [PMC free article] [PubMed] [Google Scholar]
- Bailey JB. The Diary of a Resurrectionist 1811–1812, to which are Added an Account of the Resurrection Men in London and a Short History of the Passing of the Anatomy Act. London: Swan Sonnenschein; 1896. [Google Scholar]
- Bailey B. Hangmen of England: A History of Execution from Jack Ketch to Albert Pierrepoint. London: WH Allen; 1989. [Google Scholar]
- Bennett JA, Johnston SA, Simcock AV. Solomon's House in Oxford – New Finds from the First Museum. Oxford: Museum of the History of Science Publications; 2000. [Google Scholar]
- Bhanji S. William Cooke of Exeter; apothecary, surgeon and grave-robber. Lancet. 1995;346:1212–1214. doi: 10.1016/s0140-6736(95)92907-x. [DOI] [PubMed] [Google Scholar]
- Burch D. Digging Up the Dead; the Life and Times of Astley Cooper, an Extraordinary Surgeon. London: Chatto and Windus; 2007. [Google Scholar]
- Chamberlain A. Teaching surgery and breaking the law. Br Archaeol. 1999;48:6–7. [Google Scholar]
- Chaplin S. John Hunter and the anatomy of a museum. Hist Today. 2005;55:19–25. [Google Scholar]
- Chaplin S. Nature dissected, or dissection naturalized? The case of John Hunter's museum. Mus Soc. 2008;6:135–151. [Google Scholar]
- Clark-Kennedy AE. The London: A Study in the Voluntary Hospital System, Volume One. London: Pitman Medical Publishing; 1962. [Google Scholar]
- Cole FJ. The history of anatomical injections. In: Singer C, editor. Studies in the History and Method of Science. Vol. 2. Oxford: Oxford University Press; 1921. pp. 285–343. [Google Scholar]
- Collins ET. The History and Traditions of the Moorfields Eye Hospital. London: HK Lewis; 1929. [Google Scholar]
- Cook HJ. Times bodies: crafting the preparation and preservation of Naturalia. In: Smith PH, Findlen P, editors. Merchants and Marvels: Commerce, Science and Art in Early Modern Europe. New York: Routledge; 2002. pp. 223–247. [Google Scholar]
- Cope VZ. Some Famous General Practitioners and other Medical Historical Essays. London: Pitman Medical Publishing Co; 1961. [Google Scholar]
- Craske M. ‘Unwholesome’ and ‘Pornographic’: a reassessment of the place of Rackstrow's Museum in the story of Eighteenth-Century anatomical collection and exhibition. J Hist Collect. 2010 published online in advance of print: doi: 10.1093/jhc/fhq018. [Google Scholar]
- Crossley A, Elrington CR, Chance E, et al., editors. The Victoria History of the County of Oxford. Vol. 4. London: Oxford University Press; 1979. Parish Government and Poor-Relief. [Google Scholar]
- Cunningham A. The Anatomical Renaissance: The Resurrection of the Anatomical Projects of the Ancients. Aldershot: Scolar Press; 1997. [Google Scholar]
- Cunningham A. The Anatomist Anatomis'd: An Experimental Discipline in Enlightenment Europe. Farnham: Ashgate; 2010. [Google Scholar]
- Davies M. Stories of Oxford Castle: From Dungeon to Dunghill. Oxford: Towpath Press; 2005. [Google Scholar]
- Durey MJ. Bodysnatchers and Benthamites: the implications of the Dead Body Bill for the London Schools of Anatomy, 1820–42. Lond J. 1976;2:200–225. [PubMed] [Google Scholar]
- French RK. Dissection and Vivisection in the European Renaissance. Aldershot: Ashgate; 1999. [Google Scholar]
- Gannal JN. History of Embalming, and Preparations in Anatomy, Pathology and Natural History: Including an Account of a New Process for Embalming. Philadelphia: Judah Dobson; 1840. Trans Harlan B. [Google Scholar]
- Haviland TN, Parish LC. A brief account of the use of wax models in the study of medicine. J Hist Med Allied Sci. 1970;25:52–75. doi: 10.1093/jhmas/xxv.1.52. [DOI] [PubMed] [Google Scholar]
- Hitchcock T, Shoemaker R. Tales from the Hanging Court. London: Hodder Arnold; 2006. [Google Scholar]
- Hull G. The excavation and analysis of an 18th century deposit of anatomical remains and chemical apparatus from the rear of the first Ashmolean Museum (now the Museum of the History of Science), Broad Street, Oxford. Post-Mediev Archaeol. 2003;37:1–28. [Google Scholar]
- Hurren ET. Protesting About Pauperism: Poverty, Politics and Poor Relief in Late Victorian England 1870–1900. Woodbridge: Boydell Press; 2007. [Google Scholar]
- Jerdan W. National Portrait Gallery of Illustrious and Eminent Personages of the Nineteenth Century. London: Fisher, Son and Jackson; 1834. [Google Scholar]
- Knapman P. Benjamin Franklin and the Craven Street bones. Trans Med Soc Lond. 1999;116:9–17. –2000. [PubMed] [Google Scholar]
- Lawrence SC. Charitable Knowledge: Hospital Pupils and Practitioners in Eighteenth-Century London. Cambridge: Cambridge University Press; 1996. [Google Scholar]
- Linebaugh P. The Tyburn riot against the surgeons. In: Hay D, Linebaugh P, Rule JG, Thompson EP, Winstow C, editors. Albion's Fatal Tree: Crime and Society in Eighteenth Century England. London: Penguin; 1975. pp. 65–117. [Google Scholar]
- London Hospital Medical College Board Ad hoc and special committees: minutes. 1880. –1896 Royal London Hospital Archives, ref. MC/A/4/1-2.
- Loudon I. Medical Care and the General Practitioner 1750–1850. Oxford: Clarendon Press; 1986. [Google Scholar]
- MacGregor A. Curiosity and Enlightenment: Collectors and Collections from the Sixteenth to the Nineteenth Century. New Haven: Yale University Press; 2007. [Google Scholar]
- Marshall AJ. Catalogue of the Anatomical Preparations of Dr William Hunter in the Museum of the Anatomy Department. Glasgow: University of Glasgow; 1970. [Google Scholar]
- Medvei VC, Thornton JL. The Royal Hospital of Saint Bartholomew 1123–1973. London: The Royal Hospital of Saint Bartholomew; 1974. [Google Scholar]
- Millard A. An Account of the Circumstances Attending the Imprisonment and Death of the late Mr William Millard. London: 1825. [Google Scholar]
- Miller FJW. The infirmary on the Forth, Newcastle upon Tyne, 1753–1906. Archaeol Aeliana. 1986;14:143–165. [Google Scholar]
- Nunn PG. The museum 1853–1975. Lond Hosp Gaz. 1975;77:10–12. [Google Scholar]
- Olry R. Medieval neuroanatomy: the text of Mondino dei Luzzi and the plates of Guido da Vigevano. J Hist Neurosci. 1997;6:113–123. doi: 10.1080/09647049709525696. [DOI] [PubMed] [Google Scholar]
- Park K. The criminal and the saintly body: autopsy and dissection in renaissance Italy. Renaiss Q. 1994;47:1–33. [PubMed] [Google Scholar]
- Payne L. “With much nausea, loathing, and foetor”: William Harvey, dissection, and dispassion in early modern medicine. Vesalius. 2002;8:45–52. [PubMed] [Google Scholar]
- Peachey G. John Heaviside, Surgeon. London: St. Martin's Press; 1931. [Google Scholar]
- Perry J. Syllabus of a Course of Lectures on the Principles of Surgery, delivered by Mr John Hunter, F.R.S. Eur Mag. 1782;1:245–247. [Google Scholar]
- Pole T. The Anatomical Instructor. London: Crouchman and Fry; 1790. [Google Scholar]
- Porter R. The gift relation: philanthropy and provincial hospitals in eighteenth-century England. In: Granshaw L, Porter R, editors. The Hospital in History. London: Routledge; 1989. pp. 149–178. [Google Scholar]
- Proger LW, Chambers HW. Colour preservation in pathological museum specimens. Ann R Coll Surg Engl. 1963;33:245–248. [PMC free article] [PubMed] [Google Scholar]
- Pulvertaft RJV. Museum techniques: a review. J Clin Pathol. 1950;3:1–23. doi: 10.1136/jcp.3.1.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reinarz J. The age of museum medicine: the rise and fall of the medical museum at Birmingham's school of medicine. Soc Hist Med. 2005;18:419–437. [Google Scholar]
- Richardson R. A potted history of specimen-taking. Lancet. 2000;355:935–936. doi: 10.1016/S0140-6736(00)00040-4. [DOI] [PubMed] [Google Scholar]
- Richardson R. Death, Dissection and the Destitute. 2nd edn. London: Phoenix Press; 2001. [Google Scholar]
- Richardson R. The Making of Mr Gray's Anatomy. Oxford: Oxford University Press; 2008. [Google Scholar]
- Royal London Hospital Archives 1746. London Hospital House Committee minutes September 1745–May 1748, RLHLH/A/5/2.
- Sinclair HM, Robb-Smith AHT. A Short History of Anatomical Teaching in Oxford. Oxford: Oxford University Press; 1950. [Google Scholar]
- Southwood-Smith T. The use of the dead to the living. Westminst Rev. 1824;1:3–40. [Google Scholar]
- Start M. Morbid osteology. In: Arnott R, editor. The Archaeology of Medicine, British Archaeological Reports International Series 1046. Oxford: Archaeo Press; 2002. pp. 113–124. [Google Scholar]
- Townsend J. Burke and Hare: The Body Snatchers. Cheltenham: Nelson Thomas; 2001. [Google Scholar]
- Trombley S. Sir Frederick Treves: The Extra-Ordinary Edwardian. London: Routledge; 1989. [Google Scholar]
- Vesalius A. De Humani Corporis Fabrica Libri Septem. Basel: J Oporini; 1543. [Google Scholar]
- Waddington K. Medical Education at St Bartholomew's Hospital 1123–1995. Woodbridge: Boydell Press; 2003. [Google Scholar]
- Willis T. Cerebri Anatome, cui Accessit Nervorum Descriptio et Usus. London: J Martyn & J Allestry; 1664. [Google Scholar]
- Woodward J. To Do the Sick No Harm: A Study of the British Voluntary Hospital System to 1875. London: Routledge & Kegan Paul; 1974. [Google Scholar]