

Abstract
Since platelets possess A and B antigen, mismatched ABO platelets could, theoretically, become activated or hypofunctional by exposure to anti-A or anti-B antibodies found in transfused or recipient plasma. Following normal baseline platelet aggregation to adenosine diphosphate (ADP), platelets from normal donors of different blood types were incubated at 37°C for 10 minutes with 50μl of normal saline (NS), O plasma, or AB plasma. Aggregation was then induced with ADP. No significant changes from baseline were seen in platelet aggregation studies following incubation with NS. However, platelet aggregations of type A and type B platelets were significantly inhibited when incubated with O plasma (mean of 41 and 22%, respectively). Our findings indicate that mediators in group O plasma, very likely anti-A and anti-B antibodies, cause impaired platelet aggregation of ABO non-identical platelets.
Keywords: Platelet transfusion, platelet aggregation, blood transfusion, transfusion medicine, transfusion complications, ABO blood group, anti-ABO antibodies, platelet function
Platelet function is the key cellular mechanism of primary hemostasis. Bleeding diatheses occur as a result of quantitative or qualitative disorders of platelets, which may be due to congenital or acquired causes. Acquired platelet dysfunction can be chronic, such as in leukemia, lymphoma, or bone marrow failure, or acute, such as in trauma, disseminated intravascular coagulation (DIC), or uremia. Maintaining platelet function and correcting defects in hemostasis in bleeding critically ill patients sometimes requires platelet transfusion from normal donors. At the blood donation center platelet units are provided in two forms: pooled multiple-donor whole-blood-derived or single-donor concentrates. The latter are collected via an apheresis instrument from a single donor, tested for bacterial contamination, and then stored at room temperature on a shaker until transfusion, which should occur within five days of collection. Whole blood (sometimes called random donor) platelet units, on the other hand, are collected via a separation technique from single whole blood units and stored on a shaker at room temperature until released within five days of collection. At that time, three to six random units are pooled in a single bag (one dose), tested for bacterial contamination, and then released for transfusion.
Transfusion of ABO-mismatched red blood cells (RBCs) can cause significant immune-mediated hemolytic transfusion reactions. As a result, critical complications including renal failure, DIC, end organ damage, and even death may occur. Therefore, only identical ABO RBCs are transfused, except in emergencies, when group O RBCs are transfused, despite containing anti-A and anti-B antibodies. In practice, this rule has been overlooked in fresh frozen plasma (FFP) and platelet transfusions in most centers despite reports of hemolytic reactions (acute or delayed) and some unexplained complications, such as multi-organ failure syndromes, transfusion-related lung injury (TRALI), and poor control of bleeding.1,2 Platelet transfusion is a critical component of tertiary medical care, with over nine million platelet concentrate equivalent units (about two million doses) transfused per year in the US.3 The frequency of complications is estimated to be approximately one in 1,000 platelet doses. Recent findings demonstrate that transfusion of ABO-non-identical platelets is associated with increased bleeding in surgical patients.4,5 Blunt trauma patients who received at least one ABO-non-identical blood product transfusion demonstrated significantly higher RBC usage.6 The pathogenesis of these complications remains controversial, but some evidence indicates that they may be caused by the effects of ABO incompatibility. Furthermore, in clinical practice specific ABO type platelets are required occasionally, and are considered a first-line therapy in the management of certain patients, such as those with leukemia, lymphoma, or poor responsiveness to platelet transfusion (platelet refractoriness).7,8
Considering these findings, along with our clinical observations in a blood bank/transfusion medicine practice, we formulated the following hypothesis. Since platelets possess A and B antigen on their surfaces (similar to RBCs but with lesser density),9,10 mismatched transfused or recipient platelets could become activated and/or hypofunctional by exposure to anti-A and anti-B antibodies found in the transfused or recipient plasma. Once activated, platelets undergo a shape change from the typical discoid shape to a globular form with pseudopodia. This change allows platelets to release a number of different coagulation factors, inflammatory mediators, and platelet-activating factors from their granules. This activation process mediates the transport of negatively charged phospholipids to the platelet surface, which provides a catalytic surface for clot formation.11,12 Therefore, an ABO-non-identical transfusion will cause platelet activation (either the patient’s platelets or the transfused platelets) by the anti-A and anti-B antibodies found in either the patient’s plasma or the transfused product. As a result, bleeding will be exaggerated in trauma patients, leading to more transfusion, whereas in some clinical settings excessive clot formation may occur in transfusion-dependent patients. Thus, to further characterize our preliminary clinical observations, we decided to investigate a model system to determine whether anti-A and anti-B antibodies found in plasma can mediate platelet or other hemostatic dysfunction.
Methods and Materials
Study Population
After providing consent, 30 normal donors from different blood types (O, A, B, and AB) were employed for this study. In order to minimize any confounding effects on platelet function, donors were required to be healthy at the time of each testing and to have not taken any medications for a period of at least 10 days prior to blood collection.
Sample Processing
Antecubital venipuncture was performed using a 21-gauge needle, and 18ml of blood was collected in four 3.2% sodium citrated tubes after discarding the first 2ml of blood. Samples were allowed to rest at room temperature for 15–20 minutes before processing. Tubes were then centrifuged at 100g for 10 minutes, and platelet-rich plasma (PRP) was removed and collected in a 10ml plastic tube. Platelet-poor plasma (PPP) was also collected following a second centrifugation at 1,200g for 10 minutes. The PRP platelet count was measured on Cell-Dyne 1700 (Abbott, Abbott Park, IL) and then diluted with PPP to adjust the platelet count to approximately 250×103/μl.
Platelet Function Test
The baseline quantitative platelet aggregation studies of all donors were performed as per manufacturer’s instructions on a Chrono-log Lumi aggregometer (560VS, Chrono-Log Corp., Havertown, PA), which measures the turbidity of the plasma. Briefly, 500μl of PRP with a platelet count of about 250×103/μl was delivered into an aggregometer glass cuvette. A sterile stir bar was placed at the bottom of each glass cuvette. At testing, the cuvette was placed in the instrument and a baseline platelet function was evaluated employing 20μM adenosine diphosphate (ADP) (ADP-Reagent, Chrono-Log Corp.). Aggregation of 70% or greater was considered normal. Following a normal response, 500μl of PRP (group A or B) was incubated in the aggregometer at 37°C for 10 minutes with 50μl of normal saline (NS), group O plasma (anti-A titer at antiglobulin phase of 1:1,024 and anti-B titer of 1:512), or group AB plasma. Aggregation was then induced with 20μM ADP. Changes in light transmission after adding the ADP to PRP were measured continuously and recorded for 12 minutes. All results were analyzed, and differences were calculated and compared between type A, type B, and controls using paired t-tests.
Results
Normal baseline platelet aggregation to ADP of seven type A and six type B normal blood donors was demonstrated. Following the incubation of their PRP with O plasma, platelet aggregation was significantly inhibited in comparison with NS by a mean of 41 and 22% for group A and B platelets, respectively (p≤0.005) and by 31 and 22%, respectively, in comparison with AB plasma (p≤0.005) (see Table 1). Compared with the baseline platelet aggregation studies, no significant changes were detected in either type when incubated with NS. Figure 1 shows a representative example of platelet aggregation of a type A donor. Platelet aggregation following incubation with NS was 81%, which was not different from the baseline aggregation of 80% (not shown). After incubation with O plasma (contains anti-A antibodies, titer of 1:1,024), aggregation dropped to 58% with inhibition of 29%. Platelet aggregation following incubation with AB plasma was normal at 75%.
Table 1.
Average Maximal Percentage of Platelet Aggregation with O Plasma, AB Plasma, or Normal Saline
| Average Percentage of Platelet Aggregation (SD) | |||||||
|---|---|---|---|---|---|---|---|
| Blood Donor Type | n | Normal Saline | AB Plasma | O Plasma | p-value AB versus NS | p-value O versus AB | p-value O versus NS |
| A | 7 | 92 (7.4) | 78 (2.9) | 54 (9.9) | 0.187 | <0.005 | <0.005 |
| B | 6 | 85 (6.8) | 85.3 (7.9) | 67 (9.8) | 0.939 | 0.005 | 0.005 |
NS = normal saline; SD = standard deviation.
Figure 1. Typical Platelet Aggregation of a Type A Donor.
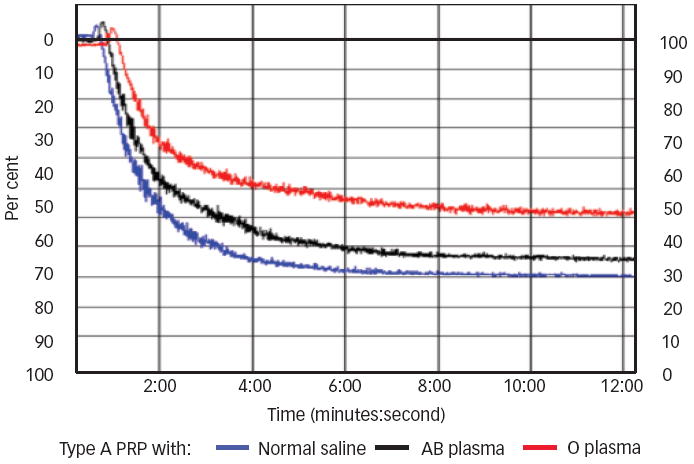
500μl of platelet-rich plasma (PRP) of platelet (PLT) type A was tested against 20μM of adenosine diphosphate (ADP) after 10 minutes of incubation at 37°C with 50μl of normal saline (blue line: aggregation of 81%), AB plasma (black line: aggregation of 75%), or O plasma (red line: aggregation of 58%, 29% inhibition).
An example of platelet aggregation of type B donor is shown in Figure 2. Platelet aggregation with NS was 78%, which was also not different from baseline aggregation of 80%. Following a 10 minutes incubation with O plasma at 37°C, aggregation dropped to 60% (an inhibition of 23%). Similar to type A, platelet aggregation after incubation with AB plasma didn’t differ from baseline (75%). To eliminate possible effects of different plasmas on platelet function, the same O and AB plasma donors, which were also negative for anti-HLA antibodies, were used in all aggregation studies. However, pilot studies on additional O and AB plasma donors (n=5) were performed and provided comparable results. As a negative control, platelet aggregation was also tested using the same ABO-type plasma as the PRP type but from a different donor, and produced consistent results.
Figure 2. Typical Platelet Aggregation of a Type B Donor.
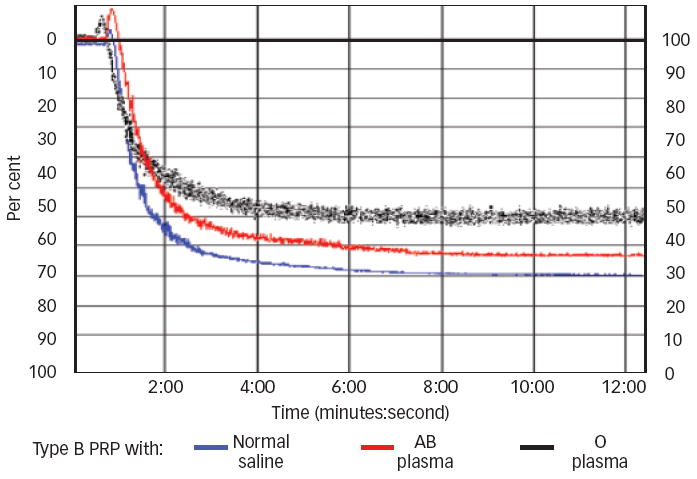
500μL platelet-rich plasma (PRP) of platelet (PLT) type B was tested against 20μM of ADP after 10 minutes of incubation at 37°C with 50μL of normal saline (blue line: aggregation of 78%), AB plasma (red line: aggregation of 75%), or O plasma (black line: aggregation of 60%, 23% inhibition).
Discussion
Our findings indicate that mediators in group O plasma, very likely anti-A and anti-B antibodies, cause impaired platelet aggregation of ABO-non-identical platelets. HLA antibodies were assessed and found to be absent in both O and AB plasmas. The ratio of plasma to platelet used in these experiments was 1:10 (50 to 500μl), which equals a transfusion of two units of either FFP or platelets to an average-size adult. The in vitro percentage of platelet inhibition may not be significant in vivo; however, patients receiving multiple transfusions, such as massively bleeding patients, may show clinically significant inhibition. In addition, platelet inhibition may also be clinically significant in transfusion-dependent patients with nadir platelet count.
Although it is rare to transfuse ABO-incompatible RBCs, except in emergency cases, it is common to transfuse other ABO-non-identical blood components, including platelets, cryoprecipitate, and FFP. In addition, it is widely acceptable in transfusion medicine practice to transfuse group O platelets (containing about 250ml plasma) to non-O patients.
However, transfusion of group O FFP (about 250ml) to non-O patients is considered inappropriate due to several reports of serious hemolytic reactions.4,13-15 Similar transfusion practices are also followed in cryoprecipitate, which contains about 150ml of plasma in a regular dose of 10 units. In fact, many blood banks distribute platelets prioritizing expiration dates rather than the ABO type. Recent findings showed that transfusion of ABO-mismatched platelets is associated with increased bleeding and hemolysis in surgical patients.4,5,16 In a recent study, Blumberg et al. showed that ABO-identical platelet transfusions in leukemia patients were a significant predictor of survival.17 Fialkow et al. also reported that blunt trauma patients who received at least one ABO non-identical blood product transfusion demonstrated a significantly higher RBC usage (12.3±6.9 SD versus 8.4±9.9 SD, p=0.0011) compared with those patients who received only ABO-identical transfusions.6
In a multicenter retrospective analysis of more than one million cancer patients over a period of nine years, Khorana et al. demonstrated an overall venous thromboembolism (VTE) rate of 4.1%. In multivariate risk factor analysis, the association between blood transfusions and VTE had an odds ratio of 1.35 (95% confidence interval [CI] 1.31–1.39) with a p-value of <0.001.18 Thus transfusion, a mainstay of many therapeutic regimens, has recently been associated with a variety of unfavorable clinical outcomes, including increased bleeding and, in some patients, thrombosis. Our in vitro findings provide potential explanations for some of these clinical observations. However, further investigation is warranted. If the in vitro findings and clinical associations are confirmed, they could have significant effects on transfusion medicine practice. Management of trauma patients and transfusion-dependent patients, which routinely ignores ABO except for RBC transfusions, might be modified to improve clinical outcomes. Financially and resource-wise, fewer transfusions might be required for massive trauma patients, and fewer complications could occur in transfusion-dependent cancer patients. Additional benefits might also accrue, including shortened hospital stays and even decreased mortality. In addition, these findings may provide a possible scientific rationale that explains, in part, the reason for increased probability of VTE in cancer patients. In summary, platelet aggregation is partially inhibited by exposure to anti-A and anti-B antibodies in ABO-non-identical plasma.
Acknowledgments
Richard P Phipps, PhD, and Neil Blumberg, MD, are supported by National Institutes of Health (NIH) grants ES01247, HL095467, and HL100051
Footnotes
Disclosure: Majed A Refaai, MD, receives clinical research funding from CSL Behring. The remaining authors have no conflicts of interest to declare.
References
- 1.Goodnough LT. Risks of blood transfusion. Anesthesiol Clin North America. 2005;23:241–52. doi: 10.1016/j.atc.2004.07.004. [DOI] [PubMed] [Google Scholar]
- 2.Dellinger EP, Anaya DA. Infectious and immunologic consequences of blood transfusion. Crit Care. 2004;8:S18–23. doi: 10.1186/cc2847. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Sullivan MT, Wallace EL. Blood collection and transfusion in the United States in 1999. Transfusion. 2005;45:141–8. doi: 10.1111/j.1537-2995.2004.03288.x. [DOI] [PubMed] [Google Scholar]
- 4.Blumberg N, Heal JM, Hicks GL, Jr, Risher WH. Association of ABO mismatched platelet transfusions with morbidity and mortality in cardiac surgery. Transfusion. 2001;41:790–3. doi: 10.1046/j.1537-2995.2001.41060790.x. [DOI] [PubMed] [Google Scholar]
- 5.Blumberg N, Gettings KF, Heal JM. ABO mismatched platelet, plasma and cryoprecipitate transfusions and bleeding in transfused surgical patients. Blood. 2005;106:122b. abstract. [Google Scholar]
- 6.Fialkow LB, Zucchiatti A, Cheng J, et al. ABO non-identical transfusions and red blood cell usage in blunt trauma patients. Transfusion. 2007;47:192A–3A. abstract. [Google Scholar]
- 7.Delaflor-Weiss E, Mintz PD. The evaluation and management of platelet refractoriness and alloimmunization. Transfus Med Rev. 2000;14:180–96. doi: 10.1016/s0887-7963(00)80007-3. [DOI] [PubMed] [Google Scholar]
- 8.Friedberg RC. Clinical and laboratory factors underlying refractoriness to platelet transfusions. J Clin Apheresis. 1996;11:143–8. doi: 10.1002/(SICI)1098-1101(1996)11:3<143::AID-JCA5>3.0.CO;2-B. [DOI] [PubMed] [Google Scholar]
- 9.Ogasawara K, Ueki J, Takenaka M, Furihata K. Study on the expression of ABH antigens on platelets. Blood. 1993;82:993–9. [PubMed] [Google Scholar]
- 10.Curtis BR, Edwards JT, Hessner MJ, et al. Blood group A and B antigens are strongly expressed on platelets of some individuals. Blood. 2000;96:1574–81. [PubMed] [Google Scholar]
- 11.Weyrich AS, Zimmerman GA. Platelets: signaling cells in the immune continuum. Trends Immunol. 2004;25:489–95. doi: 10.1016/j.it.2004.07.003. [DOI] [PubMed] [Google Scholar]
- 12.Wagner DD, Burger PC. Platelets in inflammation and thrombosis. Thromb Vasc Biol. 2003;23:2131–7. doi: 10.1161/01.ATV.0000095974.95122.EC. [DOI] [PubMed] [Google Scholar]
- 13.Brandt JT, Julius CJ, Osborne JM, Anderson CL. The mechanism of platelet aggregation induced by HLA-related antibodies. Thromb Haemost. 1996;76:774–9. [PubMed] [Google Scholar]
- 14.Blumberg N, Heal JM, Rowe JM. A randomized trial of washed red blood cell and platelet transfusions in adult acute leukemia. BMC Blood Disord. 2004;4:6. doi: 10.1186/1471-2326-4-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Shanwell A, Andersson TM, Rostgaard K, et al. Post-transfusion mortality among recipients of ABO-compatible but nonidentical plasma. Vox Sang. 2009;96:316–23. doi: 10.1111/j.1423-0410.2009.01167.x. [DOI] [PubMed] [Google Scholar]
- 16.Fung MK, Downes KA, Shulman IA. Transfusion of platelets containing ABO-incompatible plasma: a survey of 3156 North American laboratories. Arch Pathol Lab Med. 2007;131:909–16. doi: 10.5858/2007-131-909-TOPCAP. [DOI] [PubMed] [Google Scholar]
- 17.Blumberg N, Heal JM, Liesveld JL, et al. Platelet transfusion and survival in adults with acute leukemia. Leukemia. 2007;22:631–5. doi: 10.1038/sj.leu.2404920. [DOI] [PubMed] [Google Scholar]
- 18.Khorana AA, Francis CW, Blumberg N, et al. Blood transfusions, thrombosis and mortality in hospitalized cancer patients. Arch Intern Med. 2008;168:2377–81. doi: 10.1001/archinte.168.21.2377. [DOI] [PMC free article] [PubMed] [Google Scholar]