

Abstract
Giant cell tumor (GCT) of hand bones is rare. We present two cases of GCT of metacarpal bone. One case was treated successfully with ray amputation. The second patient underwent wide resection and tricortical iliac crest bone grafting. Till the last follow-up (at 26 and 70 months respectively) both patients have been recurrence free and have returned to their previous occupational activities.
Keywords: Giant cell tumor, metacarpal, recurrence
INTRODUCTION
Giant cell tumor (GCT) of the bones of the hand has some special features as compared to GCT at other sites. GCT of the metacarpal bones is rare. Unni1 reports an incidence of 1.7% for giant cell tumour of metacarpals. Biscaglia has reported an incidence of 1% for GCT of the metacarpal. Averill et al. reported an incidence of less than 1.5% in the metacarpal bones,2 while Huvos reported 3.7%, and Mirra et al. 4%.3,4 GCT of hand, including metacarpal bones. It occurs predominantly in the younger age-groups and displays more aggressive behavior.
The local recurrence rate following curettage and bone grafting has been reported to be as high as 90%.2,5–7 The relatively high recurrence rate after simple curettage often enforces extensive enbloc excision.8 Wide resection and reconstruction with structural bone grafting has also been reported to be associated with high recurrence rates.6 The metaphyseal region of the metacarpal is reported to be the common site for GCT.5,9,10 Procedures like local resection or ray amputation are used to eradicate the disease. However, local tumor control may not be absolute even with single or double ray resection for primary or recurrent GCT of the hand.
We report 2 cases of GCT of metacarpals out of 139 cases of GCT of bone treated at our institute between 1992 and 2008.
CASE REPORTS
Case 1
A 24-year-old lady presented to the outpatient department with a swelling on the dorsal aspect of her left hand of 4 months’ duration. There was a history of progressive increase in the size of the swelling. She also complained of pain that was aggravated on movement of the ring finger. There was no history of trauma. Examination revealed a tender diffuse swelling of 6 × 5 × 4 cm size along the 4th metacarpal [Figure 1A (a)]. A radiograph of the hand showed a large expansile lytic lesion with an associated soft tissue mass around the 4th metacarpal bone [Figure 1A (b)]. CT scan was also performed [Figure 1A (c)] and diagnosis of companacci Grade III GCT of the 4th metacarpal was made. Laboratory tests revealed normal serum calcium, phosphorus, and alkaline phosphatase levels. An open biopsy showed an expanded, lytic, greyish mass with hemorrhagic areas. There were few mitotic figures and the tumor was diagnosed to be a low-grade GCT.
Figure 1A.
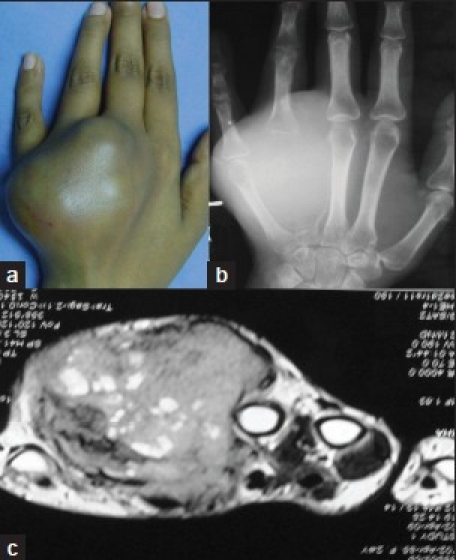
Clinical photograph (a) shows diffuse swelling on the dorsum of the hand (b) The radiograph of hand (anteroposterior view) revealed a large expansile lytic lesion with soft tissue involvement (c) MRI scan confirming grade III GCT with soft tissue involvement
On surgical exposure, friable tumor tissue was found to have replaced the entire 4th metacarpal except for the base. Primary ray resection of the ring finger was done [Figure 1B]. The patient was followed up regularly clinically and radiographically. At 28 months, there was recurrence arising from the base of the excised metacarpal, which had been left behind. This portion was excised immediately and the patient has been recurrence free since then, with good hand function [Figure 1C]. No distant metastasis had been detected.
Figure 1B.

Clinical photograph (a) showing stitch line and excised ray (b) radiograph (anteroposterior view) of the hand at 2 weeks followup. The arrow shows remnant of base of metacarpal bone
Figure 1C.
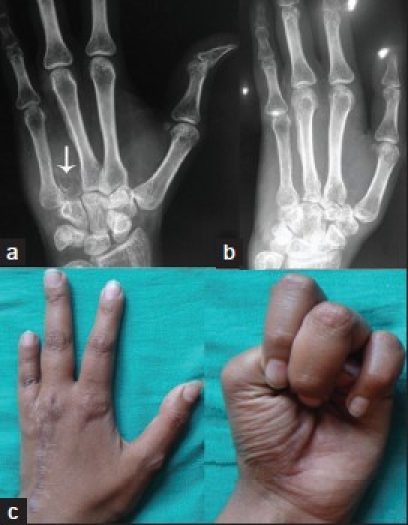
Anteroposterior X-rays (a) of hand showing recurrence (arrow) a from base of the 4th metacarpal and followup X-rays (b) at 28 months and after excision of the recurrence Clinical photograph (c) of same patient showing most recent functional status
Case 2
A 49-year-old male presented with a progressive painful swelling of 8 months’ duration on the right thumb. Local examination revealed a diffuse, tender, 5 × 4 × 4 cm swelling on the dorsoventral aspect of the thumb [Figure 2A (a)]. Physical examination showed a fusiform tender osseous mass of the right thumb. The radiograph demonstrated a large expansile lesion involving the entire 1st metacarpal, with thin septae and an associated soft tissue mass [Figure 2A (b)]. The chest radiograph was normal. Screening laboratory studies were within normal limits. Histopathology confirmed the diagnosis of GCT, demonstrating giant cells admixed with stromal cells [Figure 2B].
Figure 2A.
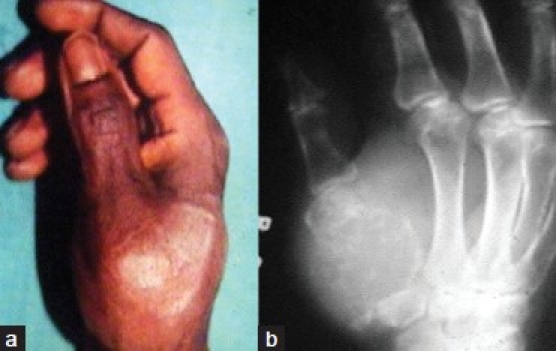
Clinical photograph (a) reveals expansile swelling on the dorsoventral aspect of the thumb (b) Radiograph of hand (oblique view) shows lytic expansile lesion involving the entire 1st metacarpal
Figure 2B.
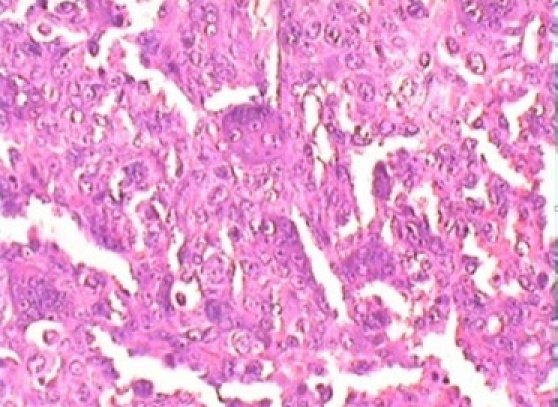
Histological picture shows osteoclastic giant cells with highly cellular stroma; mononuclear cells have marked pleomorphism
On surgery, the tumor was found to consist of brown cheesy material and was seen involving the surrounding soft tissues. The tumor was carefully removed along with a cuff of normal tissue and the proximal and distal joints were inspected. There was no articular cartilage on the trapeziometacarpal joint. A tricortical iliac crest graft was taken, inserted into the troughs created in the trapezium, and the proximal phalanx was fixed with K-wires both proximally and distally, aiming at fusion [Figure 2C]. A thumb spica was applied for 3 months postoperatively. The thumb was mobilized, following K-wire removal. The graft was well incorporated at 6 months. There has been no recurrence both clinically and radiologically at the last follow-up at 70 months post surgery [Figure 2C].
Figure 2C.

Postoperative X-ray (a) (anteroposterior and oblique view) demonstrating tricortical iliac graft with K-wire fixation (b) follow-up X-ray anteroposterior view showing good incorporation of graft and no recurrence (at 70 months followup)
Informed consent was obtained from both the patients for publication of their clinical case reports.
DISCUSSION
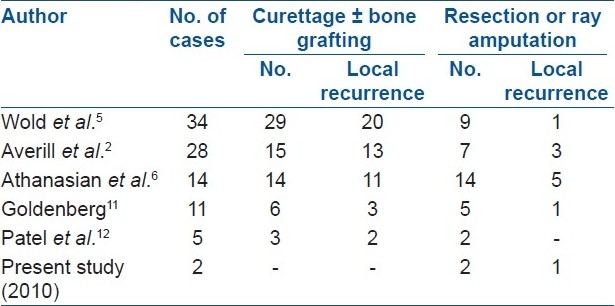
GCT of the hand seems to represent a different lesion from the conventional GCT in the rest of the skeleton. GCTs recur more rapidly in the hand than at other locations. The incidence of multicentric foci for GCTs of hand is 18%, indicating that a bone scan should be part of the routine workup in these tumors.2 Goldenberg et al.11 in their analysis of 218 cases of GCT reported 5 cases involving metacarpals. One of the largest series was reported by Averill et al.2 Their multi-institutional study included 21 patients and 28 lesions. In two other large series of 327 and 411 cases of GCTs, the authors found only 5 and 4 instances, respectively, of GCT of the hand.13,14 A review by Athanasian et al.6 reported 14 patients presenting at the Mayo clinic over a period of 50 years [Table 1].
Table 1.
Comparison of local recurrence with other studies
The various treatment modalities of GCT of hand described in literature are curettage, curettage and bone grafting, wide resection and reconstruction, irradiation, amputation, and ray amputation.2,6,11,12,15–17 Curettage alone or with bone graft resulted in recurrence rates of up to 90%.2 Most local recurrences of the GCTs of the hand are reported to occur within 1 year of primary surgery.2,6
For GCT of the metacarpal, local resection with autograft or allograft replacement is the preferred surgical treatment. We used this modality of treatment in our case 2, because of low functional demands. Wide resection or ray resection is recommended by Sanjay et al. and Ozalp et al.17,18 We choose ray resection for the grade III GCT of the metacarpal (case 1) with the aim of preventing recurrence. Following ray resection there was no functional loss of the hand and the cosmetic acceptance was better. But this resection should be complete and should include the base so as to remove the possibility of a future recurrence. Most cases of recurrent GCT require ray amputation for preventing further recurrences. Reports with ray resection or amputation are there at the cost of losing a functional finger.12,15 Singhal et al reported the successful use of radiation in a dose of 50–55 Gy to treat metacarpal GCTs.16 Prosthetic replacement has also been reported by Dingles et al.19 However, it should be borne in mind that multiple surgical procedures may increase the chances of converting a benign tumor into a malignant one and, therefore, a definitive procedure should be opted for initially.14
To conclude ray excision and reconstruction with tricortical graft for metarcarpal giant cell tumors have given good functional results.
Footnotes
Source of Support: Nil
Conflict of Interest: None.
REFERENCES
- 1.Unni KK. 5th ed. Philadelphia: Lippincott-Raven; 1996. Dahlin's bone tumours: General aspects and data on 11087 cases; pp. 263–83. [Google Scholar]
- 2.Averill RM, Smith RJ, Campbell CJ. Giant cell tumours of the bones of the hand. J Hand Surg Am. 1980;5:39–50. doi: 10.1016/s0363-5023(80)80042-6. [DOI] [PubMed] [Google Scholar]
- 3.Huvos AG. Philadelphia: W. B. Saunders; 1991. Bone tumors: Diagnosis, treatment and prognosis; pp. 429–67. [Google Scholar]
- 4.Mirra JM, Picci P, Gold RH. Philadelphia: Lea and Febiger; 1989. Bone tumours: Clinical, radiologic, and pathologic correlations; pp. 941–1020. [Google Scholar]
- 5.Wold LE, Swee RG. Giant cell tumour of small bones of hands and feet. Semin Diagn Pathol. 1984;1:173–84. [PubMed] [Google Scholar]
- 6.Athanasian EA, Wold LE, Amadio PC. Giant cell tumour of the bones of the hand. J Hand Surg Am. 1997;22:91–8. doi: 10.1016/S0363-5023(05)80187-X. [DOI] [PubMed] [Google Scholar]
- 7.Williams J, Hodari A, Janevski P, Siddiqui A. Recurrence of giant cell tumors in the hand: A prospective study. J Hand Surg Am. 2010;35:451–6. doi: 10.1016/j.jhsa.2009.12.004. [DOI] [PubMed] [Google Scholar]
- 8.Eckardt JJ, Grogan TJ. Giant cell tumour of bone. Clin Orthop Relat Res. 1986;204:45–58. [PubMed] [Google Scholar]
- 9.Feldmann F. Primary bone tumours of the hand and carpus. Hand Clin. 1987;3:269–89. [PubMed] [Google Scholar]
- 10.Dahlin DC. Giant cell bearing lesion of the bone of the hands. Hand Clin. 1987;3:291–7. [PubMed] [Google Scholar]
- 11.Goldenberg RR, Campbell CJ, Bonfiglio M. Giant cell tumour: An analysis of 218 cases. J Bone Joint Surg Am. 1970;52:619–64. [PubMed] [Google Scholar]
- 12.Patel MR, Desai SS, Gordon SL, Nimberg GA, Sclafani SJ, Vigorita VJ, et al. Management of skeletal giant cell tumour of the phalanges of the hand. J Hand Surg Am. 1987;12:70–7. doi: 10.1016/s0363-5023(87)80163-6. [DOI] [PubMed] [Google Scholar]
- 13.Campanacci M, Baldioni N, Boriami S, Sudonese A. Giant cell tumour of the bone. J Bone Joint Surg Am. 1987;69:106–13. [PubMed] [Google Scholar]
- 14.Dahlin DC. Caldwell Lecture.Giant cell tumor of bone: highlights of 407 cases. AJR Am J Roentgenol. 1985;144:955–60. doi: 10.2214/ajr.144.5.955. [DOI] [PubMed] [Google Scholar]
- 15.Slesarencko YA, Sampson SP, Gould ES. Giant cell tumour of the distal phalanx of hand. Hand Surg. 2005;10:289–91. [Google Scholar]
- 16.Singhal RM, Mukhopadhyay S, Tanwar RK, Pant GS, Julka PK. Case report: Giant cell tumour of metacarpals: report of three cases. Br J Radiol. 1994;67:408–10. doi: 10.1259/0007-1285-67-796-408. [DOI] [PubMed] [Google Scholar]
- 17.Sanjay BK, Raj GA, Younge DA. Giant cell tumours of the hand. J Hand Surg Br. 1996;21:683–7. doi: 10.1016/s0266-7681(96)80161-6. [DOI] [PubMed] [Google Scholar]
- 18.Ozalp T, Yercan H, Okçu G, Ozdemir O, Coskunol E, Bégué T, et al. Giant cell tumour of hand: Midterm results in five patients. Rev Chir Orthop Reparatrice Appar Mot. 2007;93:842–7. doi: 10.1016/s0035-1040(07)78468-4. [DOI] [PubMed] [Google Scholar]
- 19.Dingles WR, Rolle HJ. Case report of a giant cell tumour of the second metatcarpal bone and implantation of a cement prosthesis. Hand Chirurgie. 1979;11:251. [PubMed] [Google Scholar]