

Abstract
A newborn infant with multiple congenital oral swellings can be a striking sight for both parents and healthcare professionals involved in neonatal care. Neumann first described congenital epulis of a newborn in 1871, hence it is also known as Neumann's tumor. Congenital epulis occurs at birth and has a predilection for females. Congenital epulis clinically appears as a pedunculated protuberant mass. In cases with large lesions, mechanical, oral, and nasal obstruction can impair fetal deglutition or interfering with feeding and / or respiratory impairment. We are reporting a case of a six-day-old, 3.5 kg newborn female, who had reported to our institution with multiple congenital oral swellings arising from the maxilla and mandible.
Keywords: Congenital granular cell epulis, multiple congenital epulis, Neumann's tumor, oral tumors
INTRODUCTION
Congenital epulis is a reactive or degenerative lesion with a mesenchymal origin rather than a true neoplasm.[1,2] Neumann first described congenital epulis in 1871, hence it is also known as Neumann's tumor.[3–5] Congenital epulis occurs as a well-defined, pedunculated mass, with a smooth or lobulated surface. Congenital epulis commonly arises from the anterior maxillary alveolar ridge of the newborn, and isnot associated with any other congenital malformations.[3,4] Thislesion is rare as reviewed by Zuker and Buenecha in 1993, who have described only 167 reported cases in literature.[5] Congenital epulis has a female predilection, with an 8:1 ratio; an endogenous (intrauterine) hormonal stimulus is proposed, but has been disproved because of the absence of a receptor for estrogen and progesterone.[3–6]
Congenital epulis usually occurs as a single mass, although 10% of the cases occur as multiple masses. In our case there were multiple congenital epulis originating from both the mandible and maxilla.[3,4,6]
CASE REPORT
A six-day-old female child was referred from the Department of Pediatrics, with multiple swellings protruding from the mouth, which were noticed at birth.[Figure 1]. Antenatal history of pregnancy was uneventful and normal vaginal delivery occurred at 37 completed weeks. There was no family or hereditary history of this type of a case. The baby weighed 3.5 kg, and had two large lesions on the alveolar ridge of the maxilla and three smaller lesions on the mandible [Figure 1].
Figure 1.

Shows multiple oral tumors
The masses were pedunculated and covered with mucosa, which was macroscopically normal and had brisk capillary refill. On clinical examination, a round, pedunculated, 3 cm diameter, soft tissue mass, exhibiting an erythematous and smooth surface, was found in the midline and was attached to the anterior gingiva. The masses were preventing normal closure of the mouth. Three other soft tissue masses of 1.5 cm each were also found attached to the mandibles, which were smooth surfaced. Two masses were attached laterally and one at the midline of the mandible. At presentation there was no respiratory difficulty. A nasogastric tube had been placed due to feeding difficulties and the baby was breathing normally. The swellings had not increased in size in the last six days. The patient also had a depressed nasal bridge, with decreased nasal patency; however, no other structural abnormality was detected. All other mile stones were normal [Figure 1].
The general physical examination, along with laboratory tests, was otherwise normal. The patient underwent fine needle aspiration cytology (FNAC), which showed a benign fibrous lesion. The midline lesion was gently pushed laterally and subsequently oral intubation could be performed with some effort. The lesion was completely excised under general anesthesia, with minimal intraoperative hemorrhage. A regular oral feed was started on the seventh postoperative day and was well tolerated. The patient was discharged with her mother on the ninth day. At a three-week follow-up, the patient was thriving and gaining weight. Follow up for two months showed no recurrence.[Figure 2]
Figure 2.

After surgical excision of the tumor
The cut surface of the specimen showed a homogenous, grayish white tissue, which on histopathological examination showed a growth covered with mildly acanthotic squamous epithelium and underlying connective tissue showing closely packed polygonal cells, with centrally placed nuclei and a markedly granular cytoplasm and inflammatory cells. No cross striations were seen. Vascularity was increased. There was no evidence of malignancy. These findings were consistent with congenital granular cell epulis [Figure 3, histopathological picture].
Figure 3.
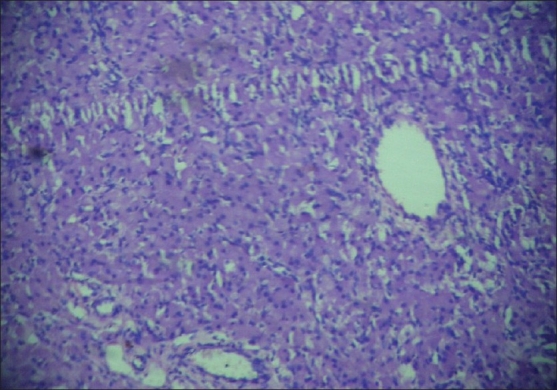
Histopathological picture of the tumor
DISCUSSION
Congenital epulis occurs in the mucosa of the maxillary alveolus as a smooth-surfaced pink mass, usually not associated with any other abnormality of the teeth or other congenital abnormalities. Congenital epulis causing superior deviation of the upper lip, flat nose with absence of the anterior nasal spine, and reduced anteroposterior dimension of the maxilla has been reported,[3] as in our case, where there was a depressed nose with deviated upper lip. The masses were not interfering with sucking [Figure 1].
Congenital epulis has a 3:1 predilection for maxillary alveolar region.[3,6] In our case the lesions occurred both in the maxilla and mandible. Congenital epulis usually occurs as a single mass although 10% of the cases occur as multiple masses. In our case there were multiple congenital epulides originating from both the mandible and maxilla.[3,4,6]
Congenital epulis (CE) of the newborn is the widely accepted term and is preferred over congenital granular cell tumor (CGCT), which is of neoplastic origin. The absence of local recurrence even after incomplete excision, the possibility of spontaneous regression, and the lack of a malignant counterpart all favour that CE is a non-neoplastic lesion.[2,4,7]
The exact histogenesis of CE is still uncertain. The various proposed cells of origin are of the odontogenic epithelium, undifferentiated mesenchymal cells, pericytes, fibroblasts, smooth muscle cells, nerve related cells, and histiocytes.[3] Based on the above findings, it is concluded that the biologic behavior of congenital epulis is compatible with embryonic hamartoma. The use of the term epulis has been disagreed upon because of the presence of the same type of lesion in another part of the body, apart from the alveolar ridge. Congenital epulis is considered to be a reactive or degenerative lesion. Histologically, these lesions appear similar to granular cell tumors; however, congenital epulis is negative for S-100 and other markers found in granular cell tumors. Congenital epulis is vimentin positive, whereas, granular cell tumor is not.
Pseudoepitheliomatous hyperplasia, a frequent finding in granular cell tumors, is generally not present in congenital epulis.[8] Malignant congenital epulis has not been reported. The differential diagnosis of a large mass in the fetal or neonatal oral cavity should include congenital malformations, such as, CE, teratoma, encephalocele, lymphatic malformation, hemangiomas, and neuroectodermal tumors.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Yvonne Nam RT. Prenatal sonographic diagnosis of congenital Epulis. J Diagn Med Sonogr. 2003;19:255–7. [Google Scholar]
- 2.Shaw L, Al-Matt A, Carlan SJ, Plumley D, Greenbaum L, Kosko J. Congenital Epulis. Three dimensional ultrasonographic findings and clinical implications. J Ultrasound Med. 2004;23:1121–4. doi: 10.7863/jum.2004.23.8.1121. [DOI] [PubMed] [Google Scholar]
- 3.Koch BL, Myeriii C, Egelhoff JC. Congenital Epulis. AJNR. 1997;18:739–41. [PMC free article] [PubMed] [Google Scholar]
- 4.Leocata P, Bifaretti G, Saltarelli S, Corbacelli A, Ventura L. Congenital (Granular Cell) Epulis of the newborn: A case report with immunohistochemical study on the histiogenesis. Ann Saudi Med. 1999;19:527–9. doi: 10.5144/0256-4947.1999.527. [DOI] [PubMed] [Google Scholar]
- 5.Lapid O, Shaco-Levy R, Krieger Y, Kachko L, Sagi A. Congenital Epulis. Pediatrics. 2001;107:1–3. doi: 10.1542/peds.107.2.e22. [DOI] [PubMed] [Google Scholar]
- 6.Wittebole A, Bayet B, Veyckemans F, Gosseye S, Vanwijck R. Congenital Epulis of newborn. Acta Chir Belg. 2003;103:235–7. doi: 10.1080/00015458.2003.11679415. [DOI] [PubMed] [Google Scholar]
- 7.Dash JK, Sahoo PK, Das SN. Congenital Granular Cell Lesion “Congenital Epulis”- Report of a case. J Indian Soc Prev Dent. 2004;22:63–7. [PubMed] [Google Scholar]
- 8.Zarbo RJ, Lloyd RV, Beals TF, McClatchey KD. Congenital gingival granular cell tumor with smooth muscle cytodifferentiation. Oral Surg Oral Med Oral Pathol. 1983;56:512–20. doi: 10.1016/0030-4220(83)90099-3. [DOI] [PubMed] [Google Scholar]