

Abstract
Objective
To examine the impact of out-migration on Kenya's nursing workforce.
Study Setting
This study analyzed deidentified nursing data from the Kenya Health Workforce Informatics System, collected by the Nursing Council of Kenya and the Department of Nursing in the Ministry of Medical Services.
Study Design
We analyzed trends in Kenya's nursing workforce from 1999 to 2007, including supply, deployment, and intent to out-migrate, measured by requests for verification of credentials from destination countries.
Principle Findings
From 1999 to 2007, 6 percent of Kenya's nursing workforce of 41,367 nurses applied to out-migrate. Eighty-five percent of applicants were registered or B.Sc.N. prepared nurses, 49 percent applied within 10 years of their initial registration as a nurse, and 82 percent of first-time applications were for the United States or United Kingdom. For every 4.5 nurses that Kenya adds to its nursing workforce through training, 1 nurse from the workforce applies to out-migrate, potentially reducing by 22 percent Kenya's ability to increase its nursing workforce through training.
Conclusions
Nurse out-migration depletes Kenya's nursing workforce of its most highly educated nurses, reduces the percentage of younger nurses in an aging nursing stock, decreases Kenya's ability to increase its nursing workforce through training, and represents a substantial economic loss to the country.
Keywords: Human resource information systems, Kenya, nursing workforce, emigration, database, professional regulatory bodies
BACKGROUND
Out-migration of nurses from low-income countries with health personnel shortages continues to exacerbate the human resources for health (HRH) crisis and pose challenges to the attainment of the Millennium Development Goals (MDGs; World Health Organization 2006). Nurses in low-income countries encounter several “push” and “pull” factors that influence out-migration.
Push factors are home country conditions that make out-migration an attractive option. They are often described as barriers to workforce retention. Key push factors that influence nurse migration include low wages (Kingma 2006, 2007; Dovlo 2007), the unemployment of trained workers (Dovlo 2007; Kingma 2007;), limited career development opportunities (Kingma 2006, 2007; World Health Organization 2006), increased workloads (Joint Learning Initiative 2004; Dussault and Franceschini 2006;), a high prevalence of HIV/AIDS (Ross, Polsky, and Sochalski 2005; Dovlo 2007;), increased risk of occupational exposure (Dussault and Franceschini 2006; Kingma 2006; World Health Organization 2006; Dovlo 2007;), political violence (Blanchet, Keith, and Shackleton 2006), and social instability (World Health Organization 2006; Kingma 2007; Nguyen et al. 2008;), among other factors.
Pull factors—which often directly mirror push factors—are destination country conditions that motivate nurses to out-migrate. Common pull factors include enhanced compensation (Ross, Polsky, and Sochalski 2005; Dussault and Franceschini 2006;), the nursing shortage in destination countries (Stilwell et al. 2004; Dussault and Franceschini 2006; Troy, Wyness, and McAuliffe 2007; Arudo 2008;), active recruitment (Ross, Polsky, and Sochalski 2005; Dussault and Franceschini 2006; Kingma 2007; Riley et al. 2007;), educational opportunities (Blanchet, Keith, and Shackleton 2006; Dussault and Franceschini 2006; Troy, Wyness, and McAuliffe 2007;), career advancement (Blanchet, Keith, and Shackleton 2006), and lower patient-to-nurse ratios (Stilwell et al. 2004; World Health Organization 2006;). Key push and pull factors affecting Kenya include the unemployment of trained nurses (Arudo 2008) and destination countries' recruitment policies (Riley et al. 2007), among other factors.
The benefits in remuneration to the individual nurse migrant, as well as the economic costs to the home country, are substantial. The gap in nurse remuneration between low-income and high-income countries is expansive. While the true disparity is somewhat smaller when cost of living is taken into consideration (McCoy et al. 2008), a newly qualified nurse in the United Kingdom making approximately U.S.$33,290 earns about 10 times the annual compensation of a newly qualified nurse in Kenya (Arudo 2008). From 1999 to 2007, 728 Kenyan nurses out-migrated to the United Kingdom alone (2009). For every nurse that out-migrates, Kenya loses U.S.$43,180 in educational costs and an estimated U.S.$338,868 return on that educational investment (Kirigia et al. 2006). While the WHO recommends countries allocate U.S.$136 million annually to scale-up training by 2015, training alone will not solve Kenya's HRH issues (World Health Organization 2006).
Several factors contribute to Kenya's nursing workforce attrition, including retirement and out-migration. A facility-level survey covering all eight Kenyan provinces revealed that retirement is the number one cause of attrition among nursing staff (Chankova, Muchiri, and Kombe 2009). However, many nurses are also unemployed (Adano 2008), which further contributes to nurses' intent to out-migrate (Arudo 2008). The unemployment of Kenyan nurses is due, in part, to poverty reduction strategies that limit public sector hiring regulated by international finance institutions (World Health Organization 2006; Kingma 2007;). Kingma explains, “Structural adjustments in the developing countries have created severe workforce imbalances and shortfalls [that] often coexist with large numbers of unemployed health professionals … Although half of all nursing positions in Kenya are unfilled, a third of all Kenyan nurses are unemployed” (Volqvartz 2005; Kingma 2007;). The unemployment of trained nurses may be a key push factor relevant to the out-migration of nurses from Kenya.
Although the problem of out-migration is well appreciated, few peer-reviewed articles supply the necessary quantitative data to inform policy analysis for HRH (Kingma 2006; Department of Human Resources for Health, World Health Organization 2008;), especially related to out-migration (Troy, Wyness, and McAuliffe 2007). Out-migration proves difficult to measure, as “much of the quantitative research on nurse migration is based on qualification verifications that document an intent or interest to migrate and not actual employment abroad” (Kingma 2007). While the United Kingdom has a centralized nurse registry, which facilitates tracking the entry of overseas nurses into their workforce, registration often occurs at the provincial or state level in the United States, Canada, and Australia, making it difficult to calculate the actual immigration of nurses (Ogilvie et al. 2007). In an effort to enhance the monitoring and evaluation of HRH issues, researchers acknowledge that health professional regulatory bodies and national ministries of health can provide valuable information regarding workforce education, specialization, distribution, employment, migration, nationality, gender, and age from their administrative databases, even if this data are generally not comparable at the international level (Diallo et al. 2003; Diallo 2004;). To facilitate greater international comparability, supply-side data can be converted into workforce-to-population ratios and compared with established workforce benchmarks needed to adequately supply services (2008).
The out-migration of nurses contributes to the HRH crisis in low-income countries, like Kenya, as they struggle to progress toward the MDGs. HRH policies are needed to enhance the management of nursing resources, including the out-migration of nurses. Using data from the Kenya Health Workforce Informatics System (KHWIS) (Riley et al. 2007), which collects information on all nurses registered in Kenya, this study aims to provide descriptive and quantitative information on (1) Kenya's nursing workforce; (2) trends in intent to out-migrate; (3) the impact of out-migration on Kenya's nursing workforce; and (4) the sociopolitical context in which out-migration occurs.
METHODS
Study Context and Data Source
This study analyzed de-identified nursing data from the KHWIS, an information system developed through a collaboration between the Kenya Department of Nursing (DON), the Nursing Council of Kenya (NCK), the Centers for Disease Control and Prevention (CDC), and the Lillian Carter Center for International Nursing at Emory University, Atlanta, GA, USA. The nursing information system consists of a database housing regulatory information (e.g., training, licensure) linked to a database housing deployment information. The regulatory database is managed by the NCK; while the deployment database is managed by the DON in the Ministry of Medical Services (MoMS), which along with the Ministry of Public Health and Sanitation (MoPHS), comprise Kenya's two health ministries. Preliminary findings from the KHWIS were published by Riley et al. (2007).
After receiving permission from the DON and NCK to analyze KHWIS data, a deidentified copy of the dataset was cleaned, organized, and analyzed with the assistance of project analysts familiar with data collection methods and data coding. The study protocols were approved by the Emory University Institutional Review Board.
Study Population
The KHWIS captured data on all nurses in Kenya who have ever been registered by the NCK. Although the two ministries of health intend to collect data on the deployment of all nurses in Kenya, at the time of the study, deployment data were available primarily on nurses working for the national government, which supplies between 50 percent and 60 percent of health care to the Kenyan population (Chankova et al. 2006, 2009). The geographic monitoring area included all eight Kenyan provinces. This study included all three classes of nurses in Kenya: enrolled, registered, and baccalaureate. Baccalaureate-prepared nurses receive a bachelor of science in nursing (B.Sc.N.), representing the highest level of nursing education in Kenya. Registered nurses receive post-secondary diploma after completing clinical training, community health, and leadership courses. Enrolled nurses are certified entry-level nurses that work under the supervision of registered nurses (Munjanja, Kibuka, and Dovlo 2005).
Data Analysis
The study period was from 1999 to 2007 and aimed to describe (1) Kenya's nursing workforce; (2) trends in nurses' intent to out-migrate; (3) the impact of out-migration on Kenya's nursing workforce; and (4) the sociopolitical context in which out-migration occurs. The path to enter the nursing workforce in Kenya includes completing preservice training, passing licensure exams, and, finally, entering the national registry. The workforce analysis included all nurses under 60 years of age trained in Kenya with initial registration dates before 2007. Kenya's nurse training capacity was analyzed using a nurse's initial registration date and index number, a unique identifier assigned at the commencement of nursing education and retained throughout his/her career.
Intent to out-migrate was measured by a destination country's request for verification of credentials submitted to the NCK. Nurses' unique index numbers were used to calculate the number of nurses intending to out-migrate. Only nurses trained in Kenya have index numbers. Nurses trained outside of Kenya were excluded from the out-migration analysis. One nurse can account for more than one request for verification (e.g., a nurse applies to out-migrate to three different countries and each country submits a request for verification to NCK); however, verification requests were linked to each nurse's index number to eliminate duplication when calculating the number of nurses intending to out-migrate. Destination countries were defined as the country submitting a request for verification of nursing credentials. The year of intent to out-migrate was defined as the date the request for verification was received by the NCK.
To evaluate the impact of out-migration on Kenya's ability to add new nurses to its national workforce, an inflow to outflow ratio of nurses was calculated, where inputs were measured by newly trained nurses and outputs were measured by nurses applying to out-migrate. This inflow to outflow ratio was compared across nurse educational preparation to assess out-migration's impact among enrolled, registered, and baccalaureate-trained nurses. The overriding intent was to determine the extent to which out-migration potentially decreases Kenya's educational efforts to maintain its nursing stock.
Additionally, nurses that expressed an intention to out-migrate were compared with the rest of the nursing workforce to determine whether nurses intending to out-migrate are distinct from nurses intending to remain in Kenya. Pearson χ2-tests and logistic regression were used to evaluate the significance of educational status, gender, and age between the two groups. The ages of nurses staying were adjusted to be comparable to the ages of the nurses intending to out-migrate at the year of initial application. Two logistic regression models were run separately to highlight the direct relationships between these demographics and intention to out-migrate. The first model included age and gender. The second model included only education.
To evaluate how closely intent to out-migrate corresponds with actual out-migration, the number of nurses that ever applied to out-migrate to the United Kingdom was compared with the number of nurses that actually out-migrated to the U.K. Data from the KHWIS regarding intent to out-migrate was compared with data on actual migration reported by the U.K. Nursing and Midwifery Council (2009). Because the timeline for applying to out-migrate to actual out-migration can take anywhere from 3 months to over a year, intent to out-migrate and actual out-migration to the United Kingdom within a 1-year timeframe may not represent the same nurses.
To understand how sociopolitical factors influence out-migration, trends in the number of nurses intending to out-migrate to the United Kingdom and United States were examined in relationship to changes in each country's nursing recruitment policies. U.K. and U.S. policies were defined by key legislation, regulations, and guidelines from each country.
RESULTS
Kenya's Nursing Workforce
There were 41,367 Kenyan trained nurses with initial registration dates before 2007 between the ages of 18 and 60. Of these, 77 percent were females and 23 percent males. The educational composition of Kenya's nursing workforce was 53 percent enrolled, 46 percent registered, and 1 percent B.Sc.N. While the mean age at initial registration was 24.5 years, the mean age of Kenya's nursing workforce was 43 years. However, in the next 10 years, 25 percent of Kenya's nursing workforce will reach the public sector retirement age of 60.
The MoMS/MoPHS actively employed 32 percent of Kenya's nursing workforce (13,615 nurses). An additional 4 percent of Kenya's nursing workforce was employed through emergency hiring programs (1,836 nurses) and assigned to government health facilities. Two national referral hospitals—Kenyatta and Moi Hospitals—which are parastatal organizations within the public sector, employed 5 percent of Kenya's nursing workforce (2,157 nurses).
For Kenya's nursing workforce, the rate of nurses trained varies by home province. Adjusting for population, nurses—at the time they enter training—are less likely to be from North Eastern, Coast, and Rift Valley provinces and more likely to be from Eastern and Central. Rates for Nairobi, Nyanza, and Western provinces are the same as the national rate, 119 nurses per 100,000 population (Figure 1).
Figure 1.
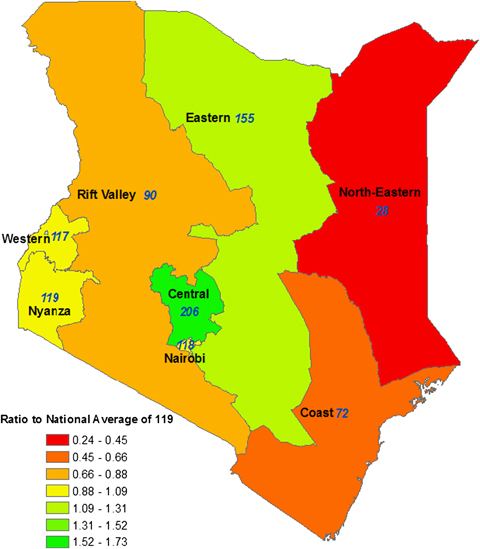
Ratio of the Rate of Nurses per 100,000 Population by Home Province to the National Rate of 119 Nurses per 100,000 Population
Note: Rates per 100,000 are shown in blue numbers on the map. The ratio of these rates to the national rate of 119 per 100,000 are indicated by color:Yellow indicates being at or close to the national average (Western, Nyanza, and Nairobi).Orange and red indicate being below the national average (Rift Valley, Coast, and North Eastern).Light green to darker green indicate being above the national average (Eastern and Central).
During the 9-year study period, Kenya registered 11,690 new nurses, of which 75 percent were female and 25 percent male. The educational composition of newly trained nurses includes 43 percent enrolled, 52 percent registered, and 5 percent B.Sc.N. On average, Kenya added 1,300 nurses annually to its national registry, indicating that the rate of training (1,300 nurses/year) is sufficient to replace the rate of nurses retiring (1,034 nurses/year) and out-migrating (184 nurses/year), but not sufficient to scale-up Kenya's nursing workforce.
Intention to Out-Migrate among Nurses
From 1999 to 2007, 2,581 nurses applied to out-migrate, potentially decreasing Kenya's ability to increase its nursing workforce through training by 22 percent. While Kenya added 11,690 newly trained nurses to its nursing workforce, 2,581 nurses in the workforce applied to out-migrate. Thus, for every 4.5 nurses Kenya adds to the nursing workforce through training, 1 nurse in the workforce applies to out-migrate. The outflow from out-migration has the potential to decrease Kenya's ability to scale-up its national nursing workforce by 19 percent for B.Sc.N. nurses, 35 percent for registered nurses, and 7 percent for enrolled nurses (Figure 2).
Figure 2.
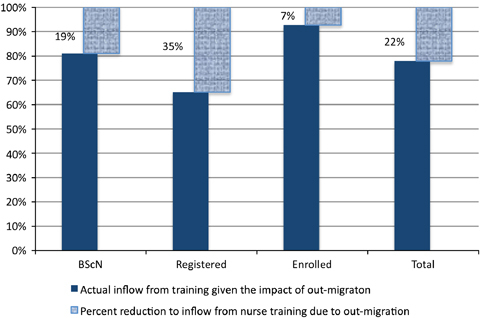
Percentage That Intent to Out-Migrate Reduces Kenya's Ability to Maintain Its Nursing Workforce through Training (N = 11,690)
Note: For every 4.5 nurses that Kenya adds to the nursing workforce through training, 1 nurse in the workforce applies to out-migrate. The inflow to outflow ratio approximates 5:1 for B.Sc.N. nurses, 3:1 for registered nurses, and 14:1 for enrolled nurses.
Because nurses applying to out-migrate represented 6 percent of Kenya's nursing workforce, nurses intending to out-migrate were compared with the rest of the nursing workforce to identify characteristics of a typical nurse migrant. Nurses intending to out-migrate were more likely to be female (85 percent of those intending to out-migrate were female compared with 77 percent female for those staying, χ2=87.701 (df=1), p-value <0.001). The odds of out-migration for females was 1.7 times higher than for males (Table S1). Additionally, nurses intending to out-migrate were more likely to be highly educated (85 percent of those intending to out-migrate were registered or B.Sc.N. nurses compared with 44 percent for those staying, χ2=1825.2 (df=2), p-value <0.001). The odds of out-migration for registered nurses was 7.7 times higher than enrolled nurses, while the odds of out-migration for B.Sc.N. nurses was 15.5 times higher than enrolled nurses (Table S1). The B.Sc.N. nurses applying to out-migrate constituted 20 percent of the B.Sc.N. nurses in Kenya's nursing workforce.
There were also significant relationships between age and intention to out-migrate (Table S1). Nurses in age groups 26–30, 31–35, and 36–40 were significantly more likely to out-migrate (2.2, 1.6, and 1.4 times, respectively) than nurses aged 21–25. Nurses aged 56–60 were 3.4 times more likely to out-migrate than nurses aged 21–25. The age of nurses at application to out-migrate explained when out-migration occurs in the natural history of a nurse's career. Thirty-one percent of nurses that applied to out-migrate applied within 5 years of entering the national registry and 18 percent applied within 6–10 years, yielding a cumulative 49 percent of nurses that applied to out-migrate within the first 10 years of entering Kenya's nursing workforce.
Nurses from all eight Kenyan provinces expressed intent to out-migrate at a national rate of 7.85 nurses/100,000 population; however, the rate of intent to out-migrate among nurses from Central and Nairobi provinces was over two times the national rate. The rate of intent to out-migrate among nurses from the following provinces was less than the national rate by 73 percent for North Eastern, 52 percent for Coast, 43 percent for Rift Valley, 25 percent for Western, 24 percent for Eastern, and 6 percent Nyanza.
For the 2,581 Kenyan trained nurses that applied to out-migrate between 1999–2007, 68 percent applied once, 23 percent applied twice, 7 percent applied three times, 2 percent applied four or more times, accounting for 3,684 applications. Eighty-two percent of first-time applications to out-migrate were to either the United States or United Kingdom, with other OECD or African countries accounting for 10 percent and 7 percent of applications, respectively (Figure 3). Comparing the number of nurses that applied to out-migrate to the United Kingdom (1,143 nurses) to the number of nurses that actually out-migrated to the United Kingdom (728 nurses), approximately 64 percent of applicants actually immigrated to the United Kingdom based on data from the U.K. Nursing and Midwifery Council register (2009).
Figure 3.
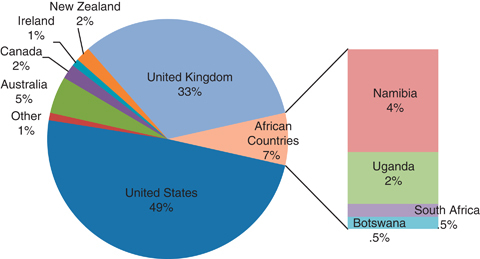
Percentage of Nurses' First Applications to Out-Migrate by Country (N = 2,581)
Data Source: Kenya health workforce information system.
Out-Migration in the Context of Sociopolitical Factors
Trends in intent to out-migrate were not consistent over the 9-year study period. Intent to out-migrate peaked between 2002–2004, accounting for 66 percent of all initial applications. The volume of applications to out-migrate corresponded with major push factors in Kenya, such as unemployment, and pull factors in the United States and the United Kingdom, such as the issuing of visas and scaling-up of the National Health Service (NHS), respectively (Figure 4). Nationally, Kenya's unemployment peaked in 2003–2004 at 25 percent, up from 16 percent over the previous 10 years (International Monetary Fund 2005). However, from 2005 to 2007, Kenya hired an additional 1,836 public sector nurses through an Emergency Hiring Plan (Gross et al. 2010). Trends in applications to the United Kingdom rose steadily from 1999 to 2004, when the NHS added 59,347 nurses from 1997 to 2004 (Buchan 2007). Trends in applications to the United States increased sharply after 2001 and peaked in 2003. Key U.S. policies included the passage of the Nursing Relief for Disadvantaged Areas Act of 1999 (Commission on Graduates of Foreign Nursing Schools [CGFNS], 1999) and the U.S. Emergency Supplemental Appropriations for Defense, the Global War on Terror and Tsunami Relief in 2005 (Chaguturu and Vallabhaneni 2005; Aiken 2007;), which issued H-1C visas and EB-3 green card visas, respectively (Table S2).
Figure 4.

Number of Applications from Kenyan Trained Nurses to Out-migrate in the Context of Sociopolitical Factors, 1999–2007
Data Source: Kenya health workforce information system, Commission on Graduates of Foreign Nursing Schools (CGFNS) (1999), Buchan (2007), Aiken (2007), Chaguturu and Vallabhaneni (2005), International Monetary Fund (2005), and Gross et al. (2010).
DISCUSSION
Out-migration affects Kenya's nursing workforce in several ways, but the most striking impact is that it decreases Kenya's ability to increase the nursing workforce through training by 22 percent. From 1999–2007, Kenya added 11,690 nurses from training; however, during this same time-period, 2,581 nurses applied to out-migrate. Thus, for every 4.5 nurses Kenya adds to its nursing workforce, 1 nurse in the workforce applies to out-migrate, making the inflow to outflow ratio 4.5:1. Kenya's capacity to maintain its nursing workforce through training decreases by 19 percent for B.Sc.N. nurses, 35 percent for registered nurses, and 7 percent for enrolled nurses (Figure 2).
Although intent to out-migrate during the 9-year study period accounted for only 6 percent of Kenya's nursing workforce, Kenya is losing a large percentage of its well-trained nurses. Eighty-five percent of applicants were registered or B.Sc.N. prepared and the B.Sc.N. nurses that applied to out-migrate constituted 20 percent of all B.Sc.N. nurses in Kenya's workforce.
Kenya's inability to absorb its younger, newly trained nurses may be an important factor contributing to nurse out-migration. Nurses applying to out-migrate are disproportionately younger, with 70 percent of nurses being between the ages of 21 to 40. The out-migration of nurses at an early age is concerning because it greatly reduces nurses' contribution to Kenya's workforce over their life span (Kirigia et al. 2006). As 49 percent of nurses applying to out-migrate apply within the first 10 years of entering the registry, introducing pay-grades that are linked to length of service (Stilwell et al. 2003) and cost of living increases may be a possible incentive for retaining newly trained nurses.
The out-migration of nurses represents a significant economic loss to Kenya. Kirigia et al. (2006) conducted a study with sensitivity analyses to assess the cost of nurse out-migration to Kenya, examining the cost of educating a nurse from primary through nursing school and the loss of return on educational investment per nurse. For every nurse that out-migrates, Kenya loses U.S.$43,180 in educational investments alone. However, when factoring in an interest rate of 5 percent over a 32-year career, the cumulative loss of return on educational investment per nurse is estimated at U.S.$205,750 (Kirigia et al. 2006). Our comparison of intent to out-migrate with actual migration revealed 64 percent of nurses that applied to out-migrate to the United Kingdom eventually out-migrated. Using this percentage as a proxy for actual out-migration, Kenya's loss of 1,652 nurses represents an economic loss of U.S.$71,333,360 in educational investments and a cumulative loss of return approximating U.S.$339,899,000.
It is also important to consider the sociopolitical context, both nationally and internationally, in which nurse out-migration is occurring. In Kenya, unemployment peaked in 2003–2004 at 25 percent (International Monetary Fund 2005). Intent to out-migrate among Kenyan nurses also peaked in 2003 (Figure 4). The unemployment of trained nurses is a key push factor contributing to out-migration in Kenya, which in turn exacerbates Kenya's nursing shortage. Even if Kenya absorbed its entire nursing registry of 42,028 nurses into its national workforce, including currently qualified but unemployed nurses and nurses trained both inside and outside of Kenya (Volqvartz 2005; Arudo 2008;), Kenya's nursing workforce to population ratio of 121 per 100,000 would still be less than the WHO recommended ratio of 200 per 100,000 needed to attain MDG benchmarks (Arudo 2008).
In the United Kingdom, the NHS Plan utilized active international recruitment to expand the NHS, fill vacancies, and add 59,347 nurses to the national registry from 1997 to 2004 (Buchan 2007). In 1999, the Department of Health in the United Kingdom issued Guidelines on International Nursing Recruitment instructing NHS employers not to recruit nurses from South Africa or the Caribbean countries U.K. Department of Health (1999). In 2001 the guidelines were expanded into the U.K. Code of Practice, which was strengthened in 2004 to discourage active recruitment from developing countries and encourage discernment in the use of recruitment agencies (U.K. Department of Health 2004; Buchan 2007;). In 2003, the Commonwealth Secretariat issued the Commonwealth Code of Practice for the International Recruitment of Health Workers, which provided ethical guidelines whereby high-income countries agreed not to actively recruit nurses from low-income countries (2007). Despite the issuing of several codes on the international recruitment of health care workers, intent to out-migrate to the United Kingdom continued to rise steadily from 1999 to 2004 (Figure 4).
In the United States, the CGFNS won a lawsuit in 1999 requiring the U.S. Immigration and Naturalization Service to issue rules for a screening program for the application of permanent residence through employment (Aiken 2007). Later that year, the U.S. President signed into law the Nursing Relief for Disadvantaged Areas Act of 1999, issuing 500 H-1C visas annually for foreign nurses, which granted 3-year stays with no possibility of extension; this law expired in 2003 (CGFNS 1999). In 2005, the United States offered the NCLEX-RN in London, Hong Kong, and Seoul, removing yet another barrier in the recruitment process (Aiken 2007) and the U.S. president signed into law the Emergency Supplemental Appropriations for Defense, the Global War on Terror and Tsunami Relief, which reallocated 50,000 EB-3, green card visas to nurses wishing to immigrate to the United States (Stilwell et al. 2004; Chaguturu and Vallabhaneni 2005;). Further research is needed to understand the relationship between the issuing of visas (i.e., nursing workforce demand as a pull factor) and intent to out-migrate.
The recently released World Health Assembly WHO Global Code of Practice on the International Recruitment of Health Personnel encourages member states to establish and support health personnel information systems that track workforce migration and its impact on national health systems (2010). The KHWIS exemplifies one such system, which allows Kenya's health ministries and professional council to track nursing migration dynamics, thereby developing more appropriate workforce strategies that not only minimize out-migration push factors but also facilitate the assimilation of returning nurses. Furthermore, with support from the President's Emergency Plan for AIDS Relief (PEPFAR), Kenya's expertise in implementing functional workforce information systems is being shared with Zimbabwe's Nursing Council and Ministry of Health and Child Welfare. Through south-to-south collaborations, Kenyan officials are orienting Zimbabwe counterparts on lessons learned and the benefits of systematic workforce information. Although PEPFAR investments are initially underwriting the system development, the design and implementation are local, thereby ensuring local ownership and sustainability over time.
Strengths and Limitations
This study has several strengths and limitations. Study strengths include the availability of accurate nursing workforce data spanning several years, which facilitates a thorough analysis of trends in training capacity, immigration, and out-migration dynamics in Kenya. By using a unique identifier for each nurse, the KHWIS can track the number of nurses applying to out-migrate and how many times they apply. This study also provides an estimate for how often intent to out-migrate ends in actual out-migration. Finally, this study places intent to out-migrate in the context of national and international policies to evaluate specific push and pull factors, such as unemployment within Kenya and the nursing shortage and issuing of visas in destination countries.
This study has some limitations. The nursing workforce may be underestimated due to the lag in data entry for nurses entering the Kenyan registry from 2007 to the present and overestimated due to the lack of attrition data recording death or change in profession. Data on current employment sector are only available for those nurses working in the public sector (MoMS/MoPHS) and do not include nurses working for the private- and faith-based health sectors, making the employment sector unknown for 59 percent of the nursing workforce and thereby limiting the assessment of percent unemployment within Kenya's nursing workforce.
Additionally, the NCK did not record requests for verification from destination countries before the early 1990s. Consistent recording of this information began after 1999; therefore, some nurses intending to out-migrate may be misclassified in our comparison group for the analysis comparing nurses intending to out-migrate to the rest of the nursing stock. However, many studies indicate that nursing out-migration did not begin to accelerate significantly until the late 1990s (Aiken 2007; Buchan 2007;).
CONCLUSIONS
Because Kenya has a critical shortage of health care workers, policies are needed to facilitate workforce absorption of approximately 1,300 new nurses entering the registry annually, as well as to address the management of out-migration. The issuing of recruitment guidelines, such as the recently released World Health Assembly WHO Global Code of Practice on the International Recruitment of Health Personnel (World Health Organization 2010), may have little impact on curbing out-migration from Kenya when destination countries continue to issue work permits and visas to fill vacant nursing positions. The World Health Assembly code of practice encourages destination countries, like the United States and the United Kingdom, to consider ways to enhance their domestic nursing workforce supply independent of immigration through workforce planning, sufficient training, and enhanced retention (2010). Simultaneously, Kenya must address critical push factors related to nurse out-migration, including the unemployment of trained nurses, nurse recruitment, and workforce retention.
The out-migration of nurses depletes Kenya's nursing workforce of its most well trained and highly educated nurses, reduces the percentage of younger nurses in an aging nursing stock, decreases Kenya's ability to increase its nursing workforce through training, and represents a substantial economic loss to the country. For these reasons, it is important that Kenya pursue a policy of managed migration that upholds individual rights and facilitates return migration, while seeking to mitigate push factors and the loss of its valuable HRH.
Acknowledgments
Joint Acknowledgment/Disclosure Statement: This project is supported by the CDC and funded with resources provided by the PEPFAR. CDC's Global AIDS Program awarded the project and oversees project activity. The findings and conclusions in this report are those of the author(s) and do not necessarily reflect the views of the Centers for Disease Control and Prevention. The Global Field Experience program at the Rollins School of Public Health, Emory University, with a gift from the O.C. Hubert Charitable Trust, provided additional support for field activities for which the authors are extremely grateful.
The authors would like to thank the staff of the Kenya Health Workforce Project for their support, as well as John Macharia for his contribution to the design and development of the Kenya Health Workforce Information System. The authors would also like to acknowledge Tom Oluoch, CDC-GAP Kenya Project Officer, for his technical assistance. A special thanks to the data clerks at the NCK, Peter Otieno Wauna, Enoch Barasa Wekesa, George Aguya Shadrack, Gladys Njoki, and Dan Nashali, who worked tirelessly on data entry and cleaning and to Rankesh Willy in the DON, MoMS, for his assistance with nurse deployment data.
Disclosures: None.
Disclaimers: None.
SUPPORTING INFORMATION
Additional supporting information may be found in the online version of this article:
Appendix SA1: Author Matrix.
Table S1: Logistic Regression Results: Comparing Nurses Intending to Out-Migrate to the Rest of the Nursing Stock
Table S2: Out-Migration in the Context of International Policies
Please note: Wiley-Blackwell is not responsible for the content or functionality of any supporting materials supplied by the authors. Any queries (other than missing material) should be directed to the corresponding author for the article.
REFERENCES
- Adano U. The Health Worker Recruitment and Deployment Process in Kenya: An Emergency Hiring Program. Human Resources for Health. 2008;6:19. doi: 10.1186/1478-4491-6-19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aiken LH. US Nurse Labor Market Dynamics Are Key to Global Nurse Sufficiency. Health Services Research. 2007;42(3, Part 2):1299–320. doi: 10.1111/j.1475-6773.2007.00714.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arudo J. Evaluation of Employment and Migration Status of Nurses from KENYA. Nairobi, East Africa: Aga Khan University; 2008. [Google Scholar]
- Blanchet K, Keith R, Shackleton P. 2006. “One Million More: Mobilising the African Diaspora Healthcare Professionals for Capacity Building in Africa.” Save the Children [accessed on March 15, 2009]. Available at http://www.hrhresourcecenter.org/node/604.
- Buchan J. International Recruitment of Nurses: Policy and Practice in the United Kingdom. Health Services Research. 2007;42(3, Part 2):1321–35. doi: 10.1111/j.1475-6773.2007.00710.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chaguturu S, Vallabhaneni S. Aiding and Abetting—Nursing Crises at Home and Abroad. New England Journal of Medicine. 2005;353(17):1761–63. doi: 10.1056/NEJMp058201. [DOI] [PubMed] [Google Scholar]
- Chankova S, Kombe G, Muchiri S, Decker C, Kimani G, Pielemeier N. Rising to the Challenges of Human Resources for health in Kenya: Developing Empirical Evidence for Policy Making. Bethesda, MD: USAID, Partners for Health Reformplus; 2006. Available at http://www.hrhresourcecenter.org/node/592. [Google Scholar]
- Chankova S, Muchiri S, Kombe G. Health Workforce Attrition in the Public Sector in Kenya: A Look at the Reasons. Human Resources for Health. 2009;7:58. doi: 10.1186/1478-4491-7-58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Commission on Graduates of Foreign Nursing Schools (CGFNS) 1999. “Nursing Relief for Disadvantaged Areas Act of 1999 Passed” [accessed on March 15, 2009]. Available at http://www.cgfns.org/sections/newsandalerts/1999/12-02-99_act.shtml. [Google Scholar]
- Department of Human Resources for Health, World Health Organization. Establishing Monitoring Benchmarks for Human Resources for Health: The Workforce Density Approach. Spotlight on health workforce statistics. Geneva, Switzerland: Department of Human Resources for Health, World Health Organization; 2008. Available at http://www.who.int/hrh/statistics/spotlight/en/index.html. [Google Scholar]
- Diallo K. Data on the Migration of Health-Care Workers: Sources, Uses, and Challenges. Bulletin of the World Health Organization. 2004;82(8):601–7. [PMC free article] [PubMed] [Google Scholar]
- Diallo K, Zurn P, Gupta N, DalPoz M. Monitoring and Evaluation of Human Resources for Health: An International Perspective. Human Resources for Health. 2003;1(1):3. doi: 10.1186/1478-4491-1-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dovlo D. Migration of Nurses from Sub-Saharan Africa: A Review of Issues and Challenges. Health Services Research. 2007;42(3, Part 2):1373–88. doi: 10.1111/j.1475-6773.2007.00712.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dussault G, Franceschini MC. Not Enough There, Too Many Here: Understanding Geographical Imbalances in the Distribution of The Health Workforce. Human Resources for Health. 2006;4:12. doi: 10.1186/1478-4491-4-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gross JM, Riley PL, Kiriinya R, Rakuom C, Willy R, Kamenju A, Oywer E, Wambua D, Waudo A, Rogers MF. The impact of an Emergency Hiring Plan on the Shortage and Distribution of Nurses in Kenya: The Importance of Information Systems. Bulletin of the World Health Organization. 2010;88(11):824–30. doi: 10.2471/BLT.09.072678. [DOI] [PMC free article] [PubMed] [Google Scholar]
- International Monetary Fund. 2005. “Kenya: Poverty Reduction Strategy Annual Progress Report–2003/2004.” Available at http://imf.org/external/pubs/ft/scr/2007/cr07158.pdf.
- Joint Learning Initiative. 2004. “Human Resources for Health: Overcoming the Crisis” [accessed on March 15, 2009]. Available at http://www.hrhresourcecenter.org/node/31.
- Kaiser Network, Global Health Workforce Alliance. 2007. A call to action: Ensuring Global Human Resources for Health. Proceedings report. Geneva. [accessed on March 15, 2009]. Available at http://www.hrhresourcecenter.org/node/1363.
- Kingma M. Nurses on the Move: Migration and the Global Health Care Economy. Ithaca: Cornell University Press; 2006. [Google Scholar]
- Kingma M. Nurses on the Move: A Global Overview. Health Services Research. 2007;42(3, Part 2):1281–98. doi: 10.1111/j.1475-6773.2007.00711.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kirigia JM, Gbary AR, Muthuri LK, Nyoni J, Seddoh A. The Cost of Health Professionals' Brain Drain in Kenya. BMC Health Services Research. 2006;6:89. doi: 10.1186/1472-6963-6-89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCoy D, Bennett S, Witter S, Pond B, Baker B, Gow J, Chand S, Ensor T, McPake B. Salaries and Incomes of Health Workers in Sub-Saharan Africa. Lancet. 2008;371(9613):675–81. doi: 10.1016/S0140-6736(08)60306-2. [DOI] [PubMed] [Google Scholar]
- Munjanja O, Kibuka S, Dovlo D. The Nursing Workforce in Sub-Saharan Africa. The Global Nursing Review Initiative, Issue 7. Geneva, Switzerland: International Council of Nurses; 2005. Available at http://www.hrhresourcecenter.org/node/630. [Google Scholar]
- Nguyen L, Ropers S, Nderitu E, Zuyderduin A, Luboga S, Hagopian A. Intent to Migrate among Nursing Students in Uganda: Measures of the Brain Drain in the Next Generation of Health Professionals. Human Resources for Health. 2008;6(1):5. doi: 10.1186/1478-4491-6-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ogilvie L, Mill JE, Astle B, Fanning A, Opare M. The Exodus of Health Professionals from Sub-Saharan Africa: Balancing Human Rights and Societal needs in the Twenty-First Century. Nursing Inquiry. 2007;14(2):114–24. doi: 10.1111/j.1440-1800.2007.00358.x. [DOI] [PubMed] [Google Scholar]
- Riley PL, Vindigni SM, Arudo J, Waudo AN, Kamenju A, Ngoya J, Oywer EO, Rakuom CP, Salmon ME, Kelley M, Rogers M, St Louis ME, Marum LH. Developing a Nursing Database System in Kenya. Health Services Research. 2007;42(3):1389–405. doi: 10.1111/j.1475-6773.2007.00715.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ross SJ, Polsky D, Sochalski J. Nursing Shortages and International Nurse Migration. International Nursing Review. 2005;52(4):253–62. doi: 10.1111/j.1466-7657.2005.00430.x. [DOI] [PubMed] [Google Scholar]
- Stilwell B, Diallo K, Zurn P, DalPoz MR, Adams O, Buchan J. Developing Evidence-Based Ethical Policies on the Migration of Health Workers: Conceptual and Practical Challenges. Human Resources for Health. 2003;1(1):8. doi: 10.1186/1478-4491-1-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stilwell B, Diallo K, Zurn P, Vujicic M, Adams O, Dal Poz M. Migration of Health-Care Workers from Developing Countries: Strategic Approaches to Its Management. Bulletin of the World Health Organization. 2004;82(8):595–600. [PMC free article] [PubMed] [Google Scholar]
- Troy PH, Wyness LA, McAuliffe E. Nurses' Experiences of Recruitment and Migration from Developing Countries: A Phenomenological Approach. Human Resources for Health. 2007;5:15. doi: 10.1186/1478-4491-5-15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- U.K. Department of Health. 1999. “Guidance on International Nursing Recruitment” [accessed on March 15, 2009]. Available at http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4073317.
- U.K. Department of Health. 2004. “Code of Practice for the International Recruitment of Healthcare Professionals.” Available at http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4097730.
- U.K. Nursing and Midwifery Council. 2009. “Statistical Analysis of the Register.” Available at http://www.nmc-uk.org/About-us/Statistics/Statistics-about-nurses-and-midwives/
- Volqvartz J. The Brain Drain. Guardian. 2005 [Google Scholar]
- World Health Organization. 2006. Working Together for Health. World Health Report. Available at http://www.who.int/whr/2006/en/
- World Health Organization. 2010. WHO Global Code of Practice on the International Recruitment of Health Personnel. World Health Assembly 63.16. Available at http://my.ibpinitiative.org/?m3mq7w6w.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.