

Abstract
Sinus histiocytosis with massive lymphadenopathy (Rosai–Dorfman disease) is a rare benign disease of unknown etiology presenting with massive lymphadenopathy. These cases can often be misdiagnosed as lymphoma. Hence, it is important to distinguish Rosai–Dorfman disease from lymphoma and other causes of histiocytosis because of the different treatment modalities. We report here a case of Rosai–Dorfman presenting with massive bilateral cervical lymphadenopathy. We conclude that fine needle aspiration cytology is a useful and reliable tool for the diagnosis of Rosai-Dorfman disease due to which biopsy can be avoided in these patients, thus, reducing inconvenience to patients.
Keywords: Emperipolesis, fine needle aspiration cytology, sinus histiocytosis with massive lymphadenopathy
Introduction
Sinus histiocytosis with massive lymphadenopathy (SHML), is a benign, self-limiting disorder that commonly involves the lymph nodes.[1] First described by Rosai and Dorfman in 1969, many more cases have been added to the literature but the cytomorphology has been documented in relatively few cases.[2] It is characterised by painless, bilateral, cervical lymphadenopathy accompanied by fever, leukocytosis, elevated erythrocyte sedimentation rate (ESR), and hypergammaglobulinemia.[1] Other lymph nodes as well as extranodal sites such as the eyes and ocular adnexa, head and neck, upper respiratory tract, skin, subcutaneous tissue, bone, skeletal muscle, central nervous system, gastrointestinal tract, salivary glands, genitourinary tract, thyroid, breast, liver, kidney, heart, uterine cervix, etc., may also be involved.[3] Whereas patients presenting with lymphadenopathy are commonly diagnosed as having malignant lymphomas, cases with extranodal involvement are suspected of having various neoplasms, depending on the site of involvement.[1]
Cytological features of SHML are virtually diagnostic and can obviate the need for a biopsy in most cases.[3]
Case Report
A 23 year-old male presented in the fine needle aspiration cytology (FNAC) clinic with multiple, bilateral, soft to firm, nontender, upper, deep cervical and submandibular lymphadenopathy of eight months’ duration, accompanied by low-grade fever. The lymph nodes had been gradually increasing in size and number during this period; there was no history of weight loss. Clinical examination showed multiple, enlarged, bilateral, cervical and submandibular lymph nodes, ranging in size from 1 × 1cm to 3 × 3 cm. They were nontender, discrete, firm, and mobile. The peripheral blood cell count showed leukocytosis (15,000/cu. mm) with neutrophilia. ESR was 40 mm at the end of one hour and the serum gammaglobulins were raised. Ultrasonography of the abdomen did not reveal any organomegaly; the patient was clinically diagnosed as having Hodgkin's lymphoma.
FNAC of the cervical nodes was performed from multiple sites. Smears were stained with giemsa stain and found to be cellular. Low-power microscopic examination revealed the presence of diffusely distributed histiocytes throughout the smears. These cells showed single to multilobated or multiple nuclei; no nuclear atypia or nuclear grooving was noted. Histiocytes had fine chromatin and inconspicuous to prominent nucleoli. These histiocytes had abundant pale cytoplasm and exhibited numerous intact lymphocytes (emperipolesis) and plasma cells [Figure 1]. A few histiocytes also showed the presence of neutrophils in their cytoplasm. In some histiocytes, the phagocytosed cells were so numerous that they obscured the nucleus. The background had mature lymphocytes, plasma cells, neutrophils, and tingible body macrophages. Based on this characteristic cytomorphology, a diagnosis of Rosai-Dorfman was made.
Figure 1.
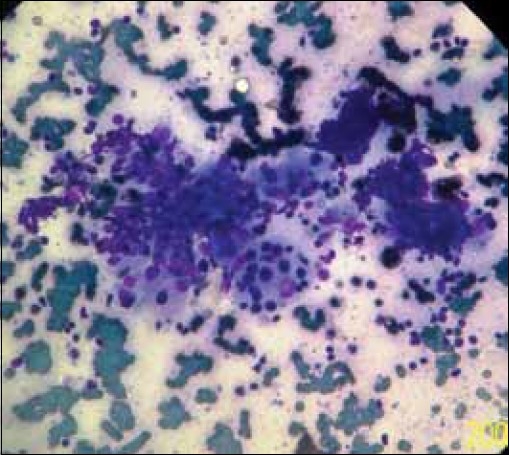
Smears showing numerous histiocytes with evidence of emperipolesis (Giemsa, ×400)
Subsequently, biopsy of a cervical lymph node was done wherein paraffin-embedded sections of lymph node biopsy showed fibrous thickening of the lymph node capsule and an altered nodal architecture. The sinuses were dilated and packed with large histiocytes having abundant pale cytoplasm and phagocytosed lymphocytes (emperipolesis), plasma cells, and occasional neutrophils.
The patient was put on steroids which resulted in marked clinical improvement.
Discussion
SHML or Rosai-Dorfman disease is a rare but well-defined, histiocytic, proliferative disorder of unknown etiology. Some investigators consider it to be of bone marrow stem cell origin.[1]
Most cases of SHML occur during the first or second decade of life. However, any age group may be affected; males are affected more than females.[3]
The clinical presentation of this entity, as described in the initial publications, consists of painless, bilateral, cervical lymphadenopathy associated with fever, leukocytosis, elevated ESR, and hypergammaglobulinemia, but a wide range of extranodal presentation has been noted in recent years.[1] Most common extranodal sites involved are the eyes and ocular adnexa, head and neck, upper respiratory tract including the nose, skin, subcutaneous tissue, bone, skeletal muscle, central nervous system, gastrointestinal tract, salivary glands, genitourinary tract, thyroid, breast, liver, kidney, heart, uterine cervix, etc.[3]
Exact pathogenesis of the disease is still not known. Theories implicating an infectious cause and immunodeficiency state have been suggested. The presence of human herpes virus 6 genome was demonstrated by in situ hybridization;[3] relationship with Klebsiella, Epstein-Barr virus, Brucella, or Cytomegalovirus were also suggested.[3,4]
Our case was a young male who presented with multiple cervical and submandibular lymphadenopathy, fever, leukocytosis, hypergammaglobulinemia, and an elevated ESR. However, the possibility of Rosai–Dorfman disease was not considered until FNAC was performed.
Cytological features of SHML usually reveal numerous large histiocytes with abundant, pale cytoplasm, and phagocytosed lymphocytes (emperipolesis). The background typically shows lymphocytes, plasma cells, and occasional neutrophils[1,2] [Figure 2]. These features were also present in our case.
Figure 2.
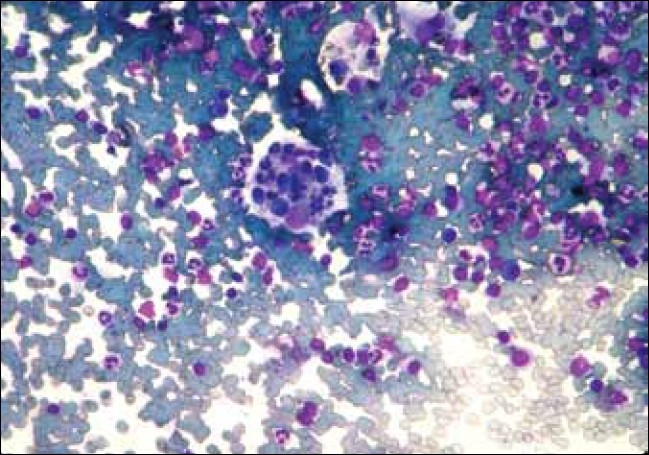
Benign histiocytes showing intact lymphocytes (emperipolesis), plasma cells, and neutrophils in their cytoplasm (Giemsa, ×400)
Histiocytes show positive immunostaining for S100 protein; CD11c, CD14, CD33, and CD68 antigens in cytological smears.[3]
Although histological findings are well documented, there have been few reports on FNAC.[2]
Differential diagnoses include reactive sinus histiocytosis, malignant histiocytosis, hemophagocytic syndrome, tuberculosis, and lymphoma.[3]
In Langerhans cell histiocytosis, Langerhans cells have grooved and twisted nuclei and the background has eosinophilic microabscess. Reactive sinus histiocytosis shows loose clusters of histiocytes, accompanying which are reactive lymphocytes, germinal center cells, immunoblasts, and tingible body macrophages; emperipolesis is absent. Hemophagocytic syndromes should be differentiated from Rosai–Dorfman disease on the basis of the presence of hemophagocytosis, absence of emperipolesis, and the presence of pancytopenia and hepatosplenomegaly. Tuberculous lymphadenitis show epithelioid cell granuloma with or without caseous necrosis, which are absent in Rosai–Dorfman disease.[2,3]
Smears from patients with Hodgkin's disease show lymphocytes, plasma cells, histiocytes, eosinophils, and Reed–Sternberg cells. In Rosai-Dorfman disease, Reed-Sternberg cells and eosinophils are not seen.[2,3]
Thus, the cytomorphology of Rosai–Dorfman disease is so distinctive that it can be diagnosed by FNAC. FNAC is a reliable and sensitive means to establish conclusive diagnosis, obviating the need for biopsy.
Footnotes
Source of Support: Nil,
Conflict of Interest: None declared.
References
- 1.Das DK, Gulati A, Bhatt NC, Sethi RG. Sinus histiocytosis with massive lymphadenopathy (Rosai–Dorfman disease): Report of two cases with fine needle aspiration cytology. Diagn Cytopathol. 2001;24:42–5. doi: 10.1002/1097-0339(200101)24:1<42::aid-dc1007>3.0.co;2-n. [DOI] [PubMed] [Google Scholar]
- 2.Deshpande AH, Nayak S, Munshi MM. Cytology of sinus histiocytosis with massive lymphadenopathy (Rosai–Dorfman disease) Diagn Cytopathol. 2000;22:181–5. doi: 10.1002/(sici)1097-0339(20000301)22:3<181::aid-dc10>3.0.co;2-6. [DOI] [PubMed] [Google Scholar]
- 3.Kumar B, Karki S, Paudyal P. Diagnosis of sinus histiocytosis with massive lymphadenopathy (Rosai–Dorfman disease) by fine needle aspiration cytology. Diagn Cytopathol. 2008;36:691–5. doi: 10.1002/dc.20904. [DOI] [PubMed] [Google Scholar]
- 4.Lampert F, Lennert K. Sinus histiocytosis with massive lymphadenopathy: Fifteen new cases. Cancer. 1976;37:783–9. doi: 10.1002/1097-0142(197602)37:2<783::aid-cncr2820370226>3.0.co;2-l. [DOI] [PubMed] [Google Scholar]