

Abstract
Objectives:
To estimate the prevalence of RTI/STI among women in urban and rural areas of Surat and analyze the influence of socioeconomic, socio-demographic and other determinants possibly related to RTI/STI.
Method:
A community-based cross-sectional study. Women aged 15-49 years (n = 102) were interviewed and underwent a gynecological examination. Specimens were collected for laboratory diagnosis of chlamydia, gonorrhea, trichomonas, bacterial vaginosis (BV), candidiasis, hepatitis B, HIV, and syphilis.
Results:
Out of 51 women in rural areas, 27 (53%) and among 51 women in urban areas, 35 (69%) were identified having RTI/STI. In total, the prevalence of trichomoniasis was found to be 41% by culture, 22% by wet mount, and 16% by Gram staining among urban women, while trichomoniasis among rural women was found to be 27% by culture, 18% by wet mount, and 14% by Gram staining. The prevalence of candidiasis was found to be 14% among urban women and 12% among rural women. By using Gram staining Nugent's criteria, the prevalence of bacterial vaginosis was found to be 24% among urban women and 25% among rural women. The prevalence of syphilis was found to be 2% by VDRL both among urban as well rural women.
Keywords: Sexually transmitted infections, reproductive tract infections
INTRODUCTION
Despite the ability to cure reproductive tract infections (RTIs), including sexually transmitted infections (STIs), they continue worldwide to be a major public health problem. RTI/STI cause serious health, economic, and social consequences. In general, information pertaining to high risk or clinic-based populations is useful, though of limited value, since it is atypical and not totally representative of a population. However, in the last few years, a number of community-based prevalence studies of gynecological morbidity among women have been undertaken in India. The study findings have provided invaluable insights into the problem of gynecological morbidity in general and RTI/STI in particular, in what may be termed as “low risk women.”
MATERIALS AND METHOD
Design and sample size
A uniform sample design as of the National Family Health Survey (NFHS) was adopted. In each region, the rural sample was selected in two stages: the selection of primary sampling units (PSUs) which are villages, with a probability proportional to population size at the first stage. It was followed by random selection of households within each PSU in the second stage during the actual survey. In urban areas, the three-stage procedure was followed. In the first stage, wards or town were selected with a probability proportional to size (PPS) sampling. In the next stage, one census enumeration block (CEB) or one segment of population was selected from each ward/town. In the final stage, households were randomly selected within each sample CEB/segment.
Sample selection
Villages were selected systematically with a probability proportional to the population size of village. As per necessity, small villages were linked with nearest bigger village to form a PSU of minimum 150 households. Also sample villages with more than 500 households were segmented and two segments per village were selected using the PPS method.
The procedure was similar in urban areas. The sample of wards/towns was selected systematically with a probability proportional to population size. One census enumeration block/segment consisting of 150-200 households was selected from each ward or town. In each household, only one of a couple (husband or wife) per household was selected. As there was a need for a larger number of subjects, therefore 100 households were targeted for inclusion of adults aged 15-49 years of age. Females who were pregnant and those on antibiotics in the previous 2 weeks were excluded.
RESULTS
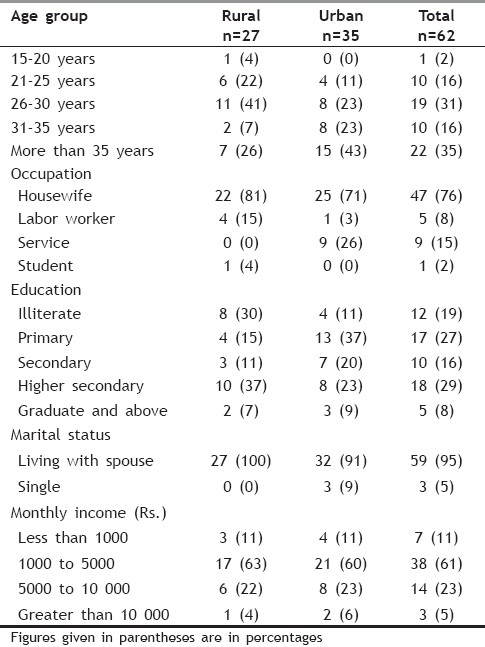
In this study, 27 (53%) women in rural and 35 (69%) women in urban areas were identified having RTI/STI. Among these women, identified with RTI/STI, majority were in age group 26 to 30 years. The prevalence of RTI/STI was found to be higher among housewives both in rural 22(81%) as well as in urban 25(71%) areas. Regarding education status, 8(30%) women of rural and 4(11%) of urban areas, identified with RTI/STI, were illiterate. In the present study, majority 17 (63%) respondents from rural areas and 21(60%) from urban areas reported their monthly income from Rs 1000 to Rs 5000 per month [Table 1].
Table 1.
Socio-demographic characteristics of women identified having RTI/STI
When asked about the knowledge of symptoms of RTI/STI, 14% were aware about the presence of discharge, as indication for infection. Dyspareunia was reported by 8% of women, whereas 9% reported dysuria, pelvic pain, and infertility as an important symptom of RTI/STI. Genital ulcer was reported as a main symptom by 8% of women. When the participants were asked about the possible ways of contracting disease, 32% replied that disease is acquired from the infected spouse. The knowledge about this fact was considerably different among rural (22%) and urban (41%) women [Table 2].
Table 2.
Knowledge regarding RTI/STI among women
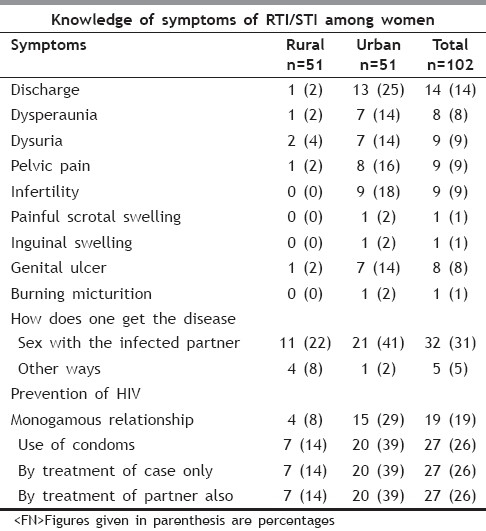
During the study, an effort was made to assess the knowledge regarding prevention of HIV among participants. About 26% reported that disease can be prevented by the use of condoms while 26% replied that it can only be prevented, if the cases are treated well, an equal number of respondents, 26% said that the treatment of partners is equally important for the prevention of disease. Maintaining monogamous relationship was reported as an important way of prevention of disease by 19% of women [Table 2].
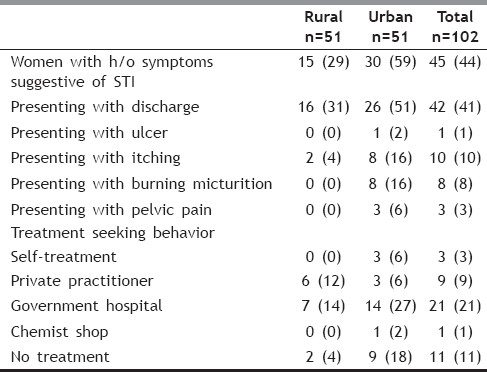
Out of all respondents, 45% reported having symptoms suggestive of RTI/STI in past. Out of 102 women, 42 (41%) presented with discharge, 10 (10%) with itching, 8 (8%) with burning micturition, 3 (3%) with pelvic pain, and only 1 (1%) presented with ulcer. Out of 45 women, having symptoms suggestive of RTI/STI, 21(21%) reported consulted government hospital for seeking treatment while only 9(9%) consulted private hospital, 3(3%) took self-treatment, while 11(11%) did not take any treatment for RTI/STI [Table 3].
Table 3.
Distribution of respondents with history of symptoms suggestive of RTI/STI and their treatment seeking behavior
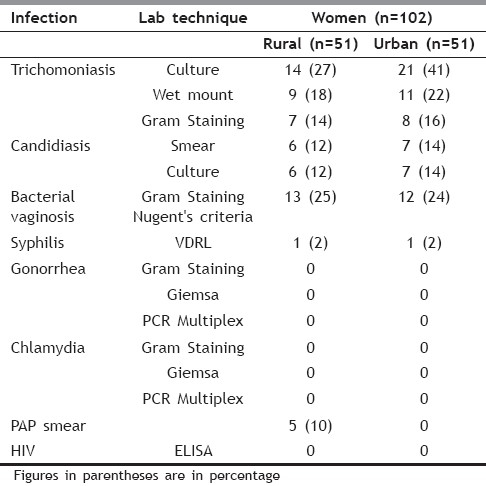
The prevalence of trichomoniasis was found to be 41% by culture, 22% by wet mount, and 16% by Gram staining among urban women, while trichomoniasis among rural women was found to be 27% by culture, 18% by wet mount, and 14% by Gram staining. The prevalence of candidiasis was found to be 14% among urban women and 12% among rural women. By using Gram staining Nugent's criteria, the prevalence of bacterial vaginosis was found to be 24% among urban women and 25% among rural women [Table 4].
Table 4.
Laboratory findings: Prevalence of RTI/STI among Women
DISCUSSION
Socio demographic profile
In this study, 27 (53%) women in rural and 35 (69%) women in urban areas were identified having RTI/STI. In a similar study conducted in Agra by Nandan et al,[1] the prevalence of RTIs/STIs came out to be 35.2% with rural prevalence higher (49%) than urban (27%). In the present study, the higher prevalence among urban population can possibly be attributed to greater proportion of migratory population residing in urban areas of Surat. Among 27 women from rural areas, identified with RTI/STI, majority 11 (41%) were in age group 26 to 30 years, while out of 35 urban women 16 (46%) were in age group 26 to 35 years. Similar findings were reported by Nandan et al.[1] where more than two-third of symptom-positive women were less then 34 years of age, which may be attributed to higher sexual activity in this age group. The prevalence of RTI/STI was found to be higher among housewives both in rural 22(81%) as well as urban 25(71%) areas. Regarding education status, 8(30%) women of rural and 4(11%) of urban areas were identified with RTI/STI were illiterate. Among these women, all 27(100%) rural and 32(91%) urban were married and living with their husbands. In another study, conducted by Kannan et al.[2] in Salem, Tamil Nadu, the overall prevalence of RTI was calculated to be 44.6% in married women belonging to the age group of 15-45 years. In the present study, majority 17 (63%) respondents from rural areas and 21(60%) from urban areas reported their monthly income from Rs 1000 to Rs 5000 per month. This finding shows that there has been a simultaneous decline in the prevalence of RTI/STI problems among women with increase in family income.
Knowledge of symptoms of RTI/STI
Out of all participants, 14% were aware about the presence of discharge, as indication for infection. Dyspareunia was reported by 8% of women, whereas 9% reported dysuria, pelvic pain, and infertility as an important symptom of RTI/STI. Genital ulcer was reported as a main symptom by 8% of women. Only 1% women could report inguinal swelling, painful scrotal swelling, and burning micturition as a symptom for RTI/STI. Urban-rural differences, however, are consistent in awareness of sexually transmitted diseases in these women.
During the study, 32% of respondents replied that disease is acquired from the infected spouse. The knowledge about this fact was considerably different among rural (22%) and urban (41%) women.
Prevention of HIV
During the study an effort was made to assess the knowledge regarding prevention of HIV among participants. About 26% reported that disease can be prevented by the use of condoms, while 26% replied that it can only be prevented if the cases are treated well, an equal number of respondents, 26% said that the treatment of partners is equally important for the prevention of disease. Maintaining monogamous relationship was reported as an important way of prevention of disease by19% of women.
Previous history of infection
Out of all respondents, 45% reported having symptoms suggestive of RTI/STI in past. Out of 102 women 42 (41%) presented with discharge, 10 (10%) with itching, 8 (8%) with burning micturition, 3 (3%) with pelvic pain, and only 1 (1%) presented with ulcer. This parallels to the study by Srivastava et al.[3] where vaginal discharge was found as most common presenting symptom in 43.48% women in urban slums.[7] In another study, conducted by Kannan et al.[2] in Salem, Tamil Nadu, the complaints of vaginal discharge was described as presenting complaint in 32.5% of respondents.Similar findings were reported by Parashar et al.[4] in a community-based study in Shimla city where vaginal discharge was reported by 36.3% of women.
Treatment-seeking behavior
Out of 45 women, having symptoms suggestive of RTI/STI, 21 (21%) reported consulted Government Hospital for seeking treatment, while only 9 (9%) consulted private hospital, 3 (3%) took self treatment while 11 (11%) did not take any treatment for RTI/STI.
Prevalence of laboratory confirmed RTI/STIs
The prevalence of trichomoniasis was found to be 41% by culture, 22% by wet mount, and 16% by Gram staining among urban women, while trichomoniasis among rural women was found to be 27% by culture, 18% by Wet mount, and 14% by Gram staining. The prevalence of candidiasis was found to be 14% among urban women and 12% among rural women.
By using Gram staining Nugent's criteria, the prevalence of bacterial vaginosis was found to be 24% among urban women and 25% among Rural women.
In different studies, there are wide variations in both the reported prevalence of syphilis and diagnostic criteria used. In the present study, the prevalence of syphilis was found to be 2% by VDRL both among urban and rural women. In a study conducted by Garg et al.[5] among 332 women in Delhi slums, 4.2% seropositivity was reported. Another community-based study, conducted by Prasad et al.[6] among rural women in Tamil Nadu, reported TPHA positivity only in 1.5% of 451 women tested (a further 0.2%, 1 woman, was found to have current syphilis infection, diagnosed by RPR positive serum).
CONCLUSIONS
This study raised an awareness regarding high vulnerability of women in urban areas of Surat for HIV infection. The study reveals that the prevalence of RTI/STI among housewives of reproductive age is quite high, with urban women being worse sufferers. This may be attributed to the fact that the size of the urban population has been steadily increasing and the pace of metropolitanization (the growth of large cities) is accelerating.[7] In Surat, selective migration of males has been a traditional feature of internal migration. Most of these migrants are married, and they leave behind their families in the villages and occasionally return to visit them.[8] An increasing volume of internal migration combined with growing urbanization may have profound implications in terms of the overall incidence of STIs in the country. Knowledge about the symptoms of RTI/STI was not adequate among both rural and urban women. The most common reported symptom of RTI/STD is vaginal discharge. Knowledge about the ways of preventing disease was also inadequate. Such a high frequency of RTI/STI requires suitable diagnostic and treatment facilities. World Health Organization has simplified the diagnosis as well as treatment through adoption of the recommended “syndromic approach” which is an appropriate approach for tackling this huge problem.
Reproductive health needs of women of urban areas should be addressed with greater importance as they may not have primary health care setting in towns and cities.
ACKNOWLEDGEMENTS
The authors acknowledge Surat Municipal Corporation, Jilla Panchayat Surat for local coordination and manpower support. They also acknowledge Resident Doctors of Microbiology, Obstetrics & Gyaenecology and Skin V. D.
Footnotes
Source of Support: Financial & Technical support: Gujarat States AIDS Control Society (GSACS); Laboratory Investigation Support: Department of Microbiology, Government Medical College, Surat and for Muliplex PCR, NARI Pune.
Conflict of Interest: None declared.
REFERENCES
- 1.Nandan D, Misra SK, Sharma A, Jain M. Estimation of prevalence of RTIs/STDs among women of reproductive age group in district Agra. Indian J Community Med. 2002;27:110. [Google Scholar]
- 2.Kannan C, Athmaraman TN, Nayeem A, Sangeetha S, Sudha R, Ponsuganthi K, et al. Prevalence of reproductive tract infections among recently married women in Veerapandi Panchayat union of Salem district, Tamil Nadu. Indian J Community Med. 2007;32:144–5. [Google Scholar]
- 3.Srivastava A, Nandan D, Mehrotra AK, Maheswari BB, Misra SK. Comparative Study of Perception about Reproductive Tract Infections among Married Women in Rural, Urban and Urban Slum areas. Indian J Community Med. 2004;29:67–8. [Google Scholar]
- 4.Parashar A, Gupta BP, Bhardwaj AK, Sharin R. Prevalence of RTIs among women of reproductive age group in Shimla city. Indian J Community Med. 2006;31:15–7. [Google Scholar]
- 5.Garg S, Sharma N, Bhalla P, Sahay R, Saha R, Raina U, et al. Reproductive Morbidity in an Indian Urban Slum: Need for Health Action. Paper presented at the Workshop on Reproductive Health in India: New Evidence and Issues, Pune, February 28-March 1. 2000 [Google Scholar]
- 6.Prasad JH, George V, Lalitha MK, Jayapaul MN, Abraham S, Shetty N, et al. Prevalence of Reproductive Tract Infection among Adolescents in a Rural Community in Tamil Nadu. Paper presented at the Workshop on Reproductive Health in India: New Evidence and Issues, Pune, February 28-March 1. 2000 [Google Scholar]
- 7.Srinivasan K. An overview of demographic transition in India since 1970. In: Srinivasan K, editor. Population Policy and Reproductive Health. New Delhi: Hindustan Publishing Corporation; 1996. pp. 3–66. [Google Scholar]
- 8.Jetley S. Impact of male migration on rural females. Econ Polit Wkly. 1987;22:WS47–53. [Google Scholar]