

Abstract
Aims:
To assess the impact of family and peers on both initiation and continuation of substance use among eighth, ninth and tenth grade adolescent high school students.
Design:
Population based cross-sectional study.
Setting:
Two high schools of West Bengal, India.
Participants:
416 students in class VIII, IX, and X in two schools.
Interventions:
None.
Measurements:
Substance use: initiation, sources, reasons for continuation. Then proportions and chi-square test was used for statistical analysis.
Materials and Methods:
This was a population based cross sectional study conducted among 416 students from class VII, IX and X in two high schools( urban and rural) of West Bengal, India selected by Multistage random sampling. A self administered anonymous pretested close ended questionnaire was used with the main outcome measures of initiation, sources, reasons for continuation of substance use based on WHO study team questionnaire.
Results:
Prevalence of substance use was found to be higher among the urban students (15.1%) than their rural counterparts (10.7%). The proportion of users was higher in the higher grades as compared to the lower grades. Among urban as well as rural students, 16 years and above were significantly more likely than their counterparts aged 15 years and below to report lifetime use. The mean age of initiation ranged from 12.6 to 13.9 years. Family members and friends were found to have a considerable influence not only on initiation but also important sources for money as well as the substance. Easy availability in the neighborhood was also an important correlate to continuation of substances.
Conclusions:
Family environment as well as peer groups has an important bearing on initiation and continuation of substance use. Experimentation of substance use motivated by peer groups is common among adolescents and starts early in life. Hence, it is necessary to provide health promotion programs directed toward students and their families which encourage attitude shaping among school children towards self-confidence and adequacy.
Keywords: Initiation, rural, source, substance use, urban
INTRODUCTION
The use of licit and illicit substances frequently starts among school children during adolescence. Many factors are thought to play a part in the initiation and perpetuation of substances. The interest and expectation of peer groups have an important bearing on whether or not a person will try a dependence-producing drug. The family may also play a role in facilitating or initiating drug use or deterring such use.[1] WHO study report on youth and drugs stated that young persons first try drugs on an experimental basis often motivated largely by curiosity and peer pressure which is one of the most widespread factors with respect to dependence-producing drugs.[2] A number of risk factors have been correlated to substance use. Among these factors, peer and family use are direct correlates to use of substances by adolescents. The social environment where the adolescent lives makes him/her susceptible to use or disuse of various substances. The vulnerability of adolescent age groups puts them at a higher risk to try any of the substances. Use of substances among adolescents in India, therefore, warrants further etiologic investigation especially into factors that facilitate and perpetuate the condition and, ultimately, robust intervention. This type of study on adolescent health was not reported from West Bengal before this study was undertaken by the investigators (e.g. in PubMed).
Objective
To assess the impact of family and peers on both initiation and continuation of substance use among sixth, seventh, and eighth grade adolescent high school students.
MATERIALS AND METHODS
Study design: Population based cross-sectional study
Study period: June 2003–May 2004 (one-year activity).
Setting: Two high schools of West Bengal, India.
Interventions: None.
Study population: 416 students in class VIII, IX, and X in two schools.
Sampling technique: Multistage random sampling.
Main outcome measures: Substance use: initiation, sources, reasons for continuation.
Content validity and reliability of study instruments: The survey module was developed on anonymous self-administered questionnaire designed by adopting the questionnaire suggested by WHO study team[3] prior to the study for ensuring feasibility, acceptability, time management, validity, and reliability. A pilot study was carried out at the Seventh Day Adventist Day School, Kolkata among students in class VIII, IX, and X following which some of the questions from the interview schedule were modified. The study conformed to the Helsinki declaration.
Study instrument: Pretested close-ended questionnaire contained questions relating to addiction and its importance. These were related with the sociodemographic situation prevailing in India. By initial translation, back-translation, retranslation followed by pilot study, the questionnaire was custom-made for the study. The questionnaire was prepared in two languages—English and Bengali (local language spoken in West Bengal). The English questionnaire was used in the urban school which was an English medium school and the Bengali questionnaire was used in the rural school which was a Bengali (vernacular) medium school. The data collection tool used for the study was an interview schedule that was developed at the institute with the assistance from the faculty members and other experts. The interview schedule included the demographic variables which covered their personal characteristics such as age and gender, as well as educational level and socioeconomic status.
Data collection procedure: Out of all the list of urban and rural high schools in West Bengal, one school in each category was chosen randomly. Then all the 478 students in class VIII, IX, and X in two schools (210 students in urban area and 268 in rural area) were initially taken as study population. Out of 478 students, 462 (205 students in urban area and 257 in rural area) could be included. The rest of the students in the sample, not included, were absent on the days of the survey. They were distributed anonymous self-administered questionnaires. The ultimate response rate was 87.02% and 416 students could be covered in our study.
The permission to conduct the study in these two schools was taken from the heads of these schools well ahead of data collection. The school teachers actively cooperated during the whole period of study. All the participants were explained about the purpose of the study and were ensured strict confidentiality, and then verbal informed consent was taken from each of them before the interview. The participants were given the options not to participate in the study if they wanted. The collection of the data was from June 1, 2003 to May 31, 2004 and filled ones were collected on the same day. Details of the questionnaire can be provided, if required.
The principal investigator collected the data and disseminated information on substance use in health education sessions to complement the findings of the study.
Indicators used in the study: Ever users: Used or abused substances irrespective of time and frequency.
Current users: Used or abused substances at least once during past 30 days.
Statistical analysis
The data collected was thoroughly cleaned and entered into Excel spreadsheets and analysis was carried out. The procedures involved were transcription, preliminary data inspection, content analysis, and interpretation. SPSS 10.0 for windows was used to calculate proportions, and Chi-square test was used in this study.
RESULTS
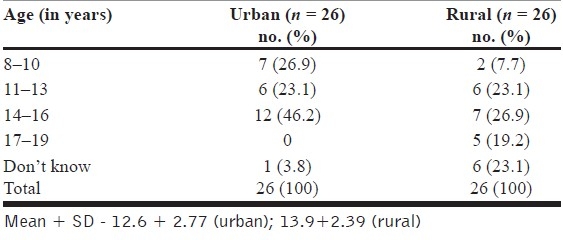
Out of a total of 416 students in the urban and rural school, 26 students(15.1%) in the urban school were ever users and 26 students(10.7%) in the rural school were ever users. The mean age of initiation of substance ranged from 12.6+ 2.77 years among urban students to 13.9+ 2.39 years among rural students. Age of initiation was an open-ended question based on memory recall. Based on the response from the study subject, table was constructed with narrow class intervals to avoid too many rows [Table 1].
Table 1.
Distribution of urban and rural user according to age of initiation of substance use
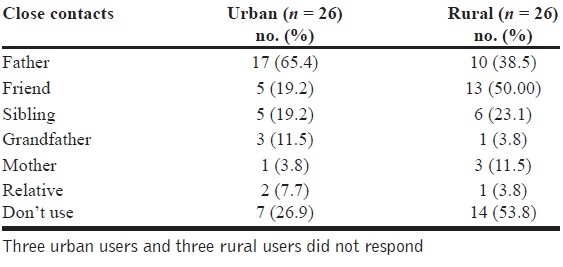
A higher proportion of users were associated with some family member also using one or more substance and fathers were found to be the most frequent of users among the students. Above 65% of urban users stated their father using some form of substance but among rural users, peers groups (50%) were associated more with substance use [Table 2].
Table 2.
Distribution of urban and rural user according to use of substances by close contacts (multiple response)
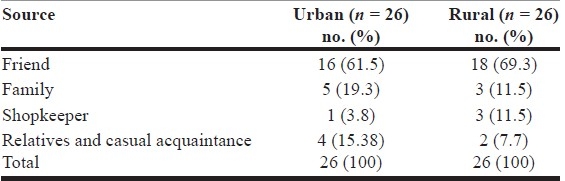
The influence of peer groups (urban = 61.5% and rural = 69.3%) has been seen to be the most important source of initiating substance use but the likelihood of family member using any substance also influenced initiation of smoking by young children. Results highlight the importance of peer and family use in predicting both onset and continuation of use. Whether it was urban or rural users, the source of initiation was similar [Table 3].
Table 3.
Distribution of urban and rural user according to source of initiation of substance use
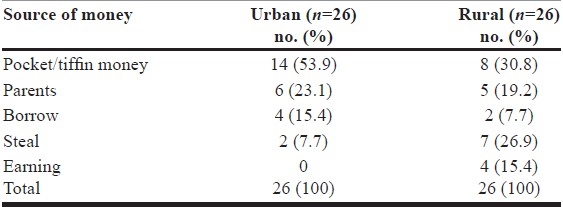
The present study reveals that pocket money was an important source of money for buying substances. The results were similar among the urban (53.85%) as well as the rural users (30.77%). And alarmingly, it was observed that the users indulged in deviant behaviors (stealing) to procure money for buying substances. The problem was higher among the rural users (26.92%) than their urban counterparts (7.69%) [Table 4].
Table 4.
Distribution of urban and rural users according to source of money for buying substances
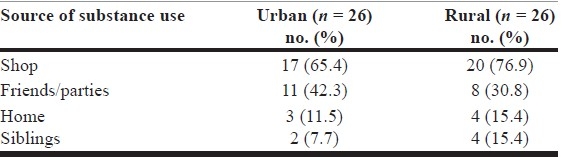
Social sources of substances were the most prevalent source over time. Neighborhood shops were the primary source of substance but accessibility at home and through friends also contributed to frequent sources of substances [Table 5].
Table 5.
Distribution of urban and rural users according to source of substance use (multiple response)
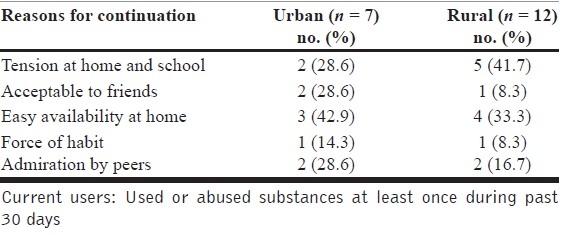
Family and peers had a trivial role in continuation of substance use by adolescents. The picture was almost similar in both the areas where majority of the urban as well as the rural users stated either had tension at home and school or easy availability at home also acceptance by peer groups as major reasons for continuation of substance use in our study population [Table 6].
Table 6.
Distribution of urban and rural current users according to reasons for continuation of substance use (multiple response)
DISCUSSION
The mean age of initiation of substance use estimated from the substance users ranged from 12 to 14 years which was almost similar with that of studies by other authors which ranged from 11 to 15 years.[4–7] Studies in northeastern India and among Croatian high school students found the age of initiation as early as 10 years.[8,9] Our findings regarding age of initiation of drug use is similar to the researchers in other parts of the globe. They found that, early onset of substance use represents significant predictors for subsequent use of other illicit substances. It was also observed that the frequency of use increases as the age advances. Therefore, it shows that all first use of substances occurs before they complete high school. Studies by researchers in this field had comparable findings.[4,5,10,11] Parental substance use and peer use was common among both the urban and rural users. These factors can act as facilitators for use of substance by the children. These findings were also cited in studies from other region.[11–16] Peer influence in initiating substance use was found to be the most important source as well as family member's habits influenced initiation of substance use by young children, as they learn by mimicking at large. This shows that a substance user at home or among friends has got a considerable impact on future use which was also seen in similar studies by other authors.[11,12,17] For an adolescent to start using substance, the facilitating factors are found in the nearest environment itself which is quite disappointing. Pocket money was stated as the most frequent source for buying substances. Students even indulged in deviant behaviors for procuring the money which reveals that substance use results in such behaviors which was observed in other studies also. [18,19] These trends in substance use are disturbing, not only for the individual but also for the society. Students reported of procuring substances from neighborhood shops, apart from that easy accessibility at home and from peers were important predictors of increases in substance use and intentions over time.[11,20] Findings from Global Youth Tobacco Survey reveal that easy availability of tobacco products in stores was particularly associated with continuation of substance use.[21] The above findings reveal that the initiating and continued use remains the same whether it is for an urban user or a rural one and not much variation is seen among different regions where the sociodemographic correlates remain the same. Easy availability of substances at home or through peers and acceptability by peers was the commonest reason for continuation followed by tension at home or school which shows clearly that whether directly or indirectly, family and peers had an important part to play in continuation of substance use in our study population. These reasons have been cited even by other researchers in this field.[22–25] This shows that home and friends itself furnishes the adolescents with ways to procure and continue using substances. And since adolescents are in a transitional phase, therefore confusion sometimes can lead them to become susceptible to take up unfavorable habits.
Limitations
The data set on which the study is based is not particularly large (416 students) and from one urban and one rural high school as there was economic and other constraints (time, manpower). The ever users among the subject was our area of interest for different constraints stated above. Though the study may not be generalized to judge the variation among urban and rural schools still it shows some trends and patterns of drug use among adolescent high school students in this part of the world. The instrument used in this study was the latest WHO validated one available during the planning of the study.
CONCLUSION
Family and peer group effects were contingent on both initiation and continuation of adolescent substance use. Additionally, neighborhood availability of substances, especially the licit ones, acts as facilitators for substance use. Early onset of use of substances is associated with a clustering of health risk behaviors in the future. Substance use prevention programs for adolescents should be directed not only to them but also to the neighborhoods in which they live. Greater attention for reducing social access to substances, particularly among parents, is needed for prevention efforts prior to and during high school. Interventions that enhance parental self-efficacy in conveying and enforcing such policies for their children could reduce adolescent use. It would be important to emphasize creating safer neighborhood environments that support the development of a stronger sense of hope for the future. These results also indicate the importance of urging families to have greater concern for shaping up the behavior of their children, of preventing illegal sale of cigarettes to anyone under the age of 20 years and encourage attitude shaping among school children towards self-confidence and adequacy.
Footnotes
Source of Support: Nil
Conflict of Interest: None.
REFERENCES
- 1.Kramer JF, Cameron DC. Geneva: WHO; 1975. A manual on drug dependence; pp. 19–26. [Google Scholar]
- 2.WHO Tech Rep Series. Youth and drugs. 1969;407:7–27. [Google Scholar]
- 3.Smart RG, Hughes PH, Johnston LD, et al. A methodology of student drug use surveys. WHO offset publication No. 50. 1980 [Google Scholar]
- 4.Maglione T, De Maria C, Assante M, Pennino G. Prevalence of smoking habits among secondary school students in Benevento. Epidemiol Prev. 1994;18:237–40. [PubMed] [Google Scholar]
- 5.Ogwell AE, Aström AN, Haugejorden O. Socio-demographic factors of pupils who use tobacco in randomly-selected primary schools in Nairobi province, Kenya. East Afr Med J. 2003;80:235–41. doi: 10.4314/eamj.v80i5.8693. [DOI] [PubMed] [Google Scholar]
- 6.Franco JA, Pérez Trullén A, García A, Marrón R, Clemente ML, Rubio E. Tobacco use among young people in informal education settings: A survey of behaviors and opinions Arch Bronconeumol. 2004;40:10–6. doi: 10.1016/s1579-2129(06)60185-7. [DOI] [PubMed] [Google Scholar]
- 7.Maglione T, De Maria C, Assante M, Pennino G. Prevalence of smoking habits among secondary school students in Benevento Epidemiol Prev. 1994;18:237–40. [PubMed] [Google Scholar]
- 8.Sinha DN, Gupta PC, Pednekar MS. Tobacco use among students in the eight North-eastern states of India. Indian J Cancer. 2003;40:43–59. [PubMed] [Google Scholar]
- 9.Mpabulungi L, Muula AS. Tobacco use among high shool students in Kampala, Uganda: Questionnaire study. Croat Med J. 2004;45:80–3. [PubMed] [Google Scholar]
- 10.Takakura M, Wake N. Association of age at onset of cigarette and alcohol use with subsequent smoking and drinking patterns among Japanese high school students. J Sch Health. 2003;73:226–31. doi: 10.1111/j.1746-1561.2003.tb06566.x. [DOI] [PubMed] [Google Scholar]
- 11.Kwamanga DH, Odhiambo JA, Amukoye EI. Prevalence and risk factors of smoking among secondary school students in Nairobi. East Afr Med J. 2003;80:207–12. doi: 10.4314/eamj.v80i4.8644. [DOI] [PubMed] [Google Scholar]
- 12.Skolnik N, Diamond JJ. Patterns and correlates of tobacco use among suburban Philadelphia 6th- through 12th-grade students. Fam Med. 1999;31:128–32. [PubMed] [Google Scholar]
- 13.Yang MS, Yang MJ, Liu YH, Ko YC. Prevalence and related risk factors of licit and illicit substances use by adolescent students in southern Taiwan. Public Health. 1998;112:347–52. doi: 10.1038/sj.ph.1900494. [DOI] [PubMed] [Google Scholar]
- 14.Maziak W, Mzayek F. Characterization of the smoking habit among high school students in Syria. Eur J Epidemiol. 2000;16:1169–76. doi: 10.1023/a:1010907724688. [DOI] [PubMed] [Google Scholar]
- 15.Blackford KA, Bailey PH, Coutu-Wakulczyk GM. Tobacco use in northeastern Ontario teenagers: Prevalence of use and associated factors. Can J Public Health. 1994;85:89–92. [PubMed] [Google Scholar]
- 16.Rao EV, Mishra K, Mohapatra B. Prevalence of substance abuse among school going adolescents of various high schools of Cuttack city. IPHA 2004, Bhubaneshwar souvenir; AB. 2002;28:56–7. [Google Scholar]
- 17.D’Amico EJ, McCarthy DM. Escalation and initiation of younger adolescents’ substance use: The impact of perceived peer use. J Adolesc Health. 2006;39:481–7. doi: 10.1016/j.jadohealth.2006.02.010. [DOI] [PubMed] [Google Scholar]
- 18.Drug Addiction: An Overview. Swasth Hind. 1978;6:121–4. [Google Scholar]
- 19.CASA 2003 Teen survey. National center on addiction and substance abuse. [last accessed on 2007 Oct 10]. Available from: http://www.casacolumbia.org .
- 20.Hearst MO, Fulkerson JA, Maldonado-Molina MM, Perry CL, Komro KA. Who needs liquor stores when parents will do? The importance of social sources of alcohol among young urban teens. Prev Med. 2007;44:471–6. doi: 10.1016/j.ypmed.2007.02.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Waren CW, Riley L, Asma S, Eriksen MP, Green L, Blanton C, et al. Tobacco use by youth: A surveillance report from the global youth tobacco survey project. Bull World Health Organ. 2000;78:868–74. [PMC free article] [PubMed] [Google Scholar]
- 22.Komro KA, Maldonado-Molina MM, Tobler AL, Bonds JR, Muller KE. Effects of home access and availability of alcohol on young adolescents’ alcohol use. Addiction. 2007;102:1597–608. doi: 10.1111/j.1360-0443.2007.01941.x. [DOI] [PubMed] [Google Scholar]
- 23.Sargent JD, Beach ML, Dalton MA, Mott LA, Tickle JJ, Ahrens MB, et al. Effect of seeing tobacco use in films on trying smoking among adolescents: Cross sectional study. BMJ. 2001;323:1394–7. doi: 10.1136/bmj.323.7326.1394. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Singh V, Gupta R. Prevalence of tobacco use and awareness of risks among school children in Jaipur. J Assoc Physicians India. 2006;54:609–12. [PubMed] [Google Scholar]
- 25.Sinha DN, Roychowdhury S. Tobacco control practices in 25 schools of West Bengal. Indian J Public Health. 2004;48:128–31. [PubMed] [Google Scholar]