

Abstract
The role of surveillance endoscopic followup in colectomized patients with long standing total colitis is controversial. Here, we aimed to clarify its usefulness for the early detection of dysplasia and cancer in this group of patients. Ninety-seven colectomised UC patients followedup by surveillance endoscopy were retrospectively investigated by reviewing the pathological reports. Patients had received either subtotal colectomy and ileo-rectal anastomosis (IRA) or total proctocolectomy and ileal anal anastomosis (IPAA). Definite dysplasia was diagnosed in 4 patients, who had received IRA; among them, 2 were carcinoma with submucosal invasion, and one was a high-grade dysplasia. Postoperative surveillance endoscopy is useful for the detection of early cancer in the remaining colonic mucosa of UC patients, and those receiving IRA, in which rectal mucosa is left intact, would be good candidates. However, its effectiveness for patients receiving IPAA, in which the rectal mucosa is resected, needs further investigation.
1. Introduction
Long-standing extensive ulcerative colitis (UC) is reported to be a risk factor for the development of colorectal cancer (CRC) [1–3]. Surveillance colonoscopy instead of prophylactic proctocolectomy is generally recommended for those with total colitis for more than 8 years after the onset or left-sided colitis for more than 15 years [4, 5].
Subtotal colectomy with ileo-rectal anastomosis (IRA) had been the surgical treatment of choice for UC until pouch operation was established, but patients undergoing subtotal colectomy have also been reported to carry a certain risk of developing carcinoma in the rectal remnant [6, 7]. Furthermore, Johnson et al. reported that most of them were found in an advanced stage [7]. Although the importance of surveillance colonoscopy for the rectal remnant has been emphasized, few reports describe the effectiveness of surveillance colonoscopy in the colectomized population.
Since the 1980s, total proctocolectomy and ileal pouch-anal anastomosis (IPAA) has become the surgical treatment of choice for UC [8, 9]. Although total proctocolectomy eliminates the risk of colorectal cancer, several cases with cancer in the rectal remnant or ileal pouch have been reported. The major methods of IPAA are stapled IPAA without mucosectomy and handsewn IPAA with mucosectomy. Stapled IPAA is a safer and less complicated method than handsewn IPAA, but the rectal remnant of a few centimeters may retain a malignant potential. Mucosectomy could theoretically remove all the rectal mucosa that might have malignant potential. However, the resected specimens of the patients undergoing pouch excision following mucosectomy revealed that isolated rectal mucosa might remain [10, 11]. Indeed, several cases of “rectal” carcinoma after mucosectomy have been reported [12–14]. Moreover, several cases of dysplasia or cancer in the ileal pouch have been reported after IPAA [15–17].
Although those cases of UC who have undergone colectomy may be at risk of carcinoma in the rectal remnant or the ileal pouch, the effectiveness of surveillance endoscopy after colectomy is still controversial. The aim of this study is to clarify the effectiveness of surveillance endoscopy after colectomy in UC.
2. Methods
2.1. Patients
Ninety-seven UC patients who received colectomy and postoperative surveillance endoscopy in our surgical department, in the period between January 1979 and December 2008, were retrospectively analyzed. Among them, 29 had received IRA, and 68 IPAA (stapled without mucosectomy in 47 and hand-sewn with mucosectomy in 21).
2.2. Endoscopy
Surveillance endoscopy, using flexible endoscopes, was conducted regularly in most of the cases, and in addition to the conventional observation by the experienced colonoscopist, the dye spray method was performed for the better visualization of mucosal lesions. Only those patients who had at least one postoperative biopsy were included. Biopsy specimens were taken from the lesions suggestive of dysplasia as well as from the apparently normal flat rectal mucosa of patients who had received IRA or stapled IPAA (either with or without mucosectomy). Pathological reports from all patients were retrospectively reviewed for the patients' clinicopathological features, the surgical procedures, and the colonoscopic and histological diagnosis.
2.3. Pathology
Dysplasia was graded, according to the Riddell' classification, into high-grade (HGD), low-grade (LGD), indefinite (IND), or negative for dysplasia [18].
2.4. Evaluation
Histopathological reports were retrospectively reviewed, and the patient's clinicopathological features, such as age, duration after onset of UC, time after colectomy, and histopathological diagnosis of the resected surgical specimen, were analyzed according to the presence or absence of dysplasia.
3. Results
A total of 531 surveillance endoscopies were performed. The median followup time after operation was 5.3 and 15.6 years for those who had received IPAA and IRA, respectively. Results of postoperative surveillance endoscopy are summarized in Figure 1.
Figure 1.
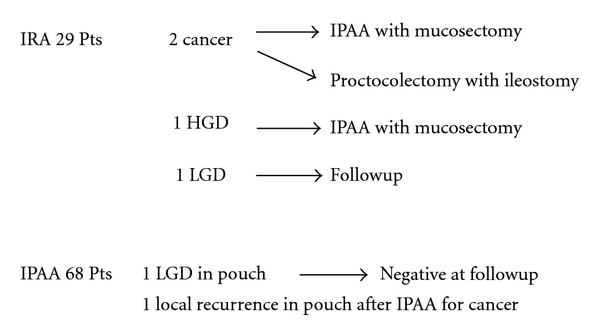
Results of postoperative surveillance endoscopy after colectomy in patients with ulcerative colitis.
By the surveillance endoscopy, 4 patients who had received IRA were diagnosed as definite dysplasia (Table 1, Figure 2). Among them, 2 had received hand-sewn IPAA with mucosectomy, and one rectal excision. One patient was not operated on due to the presence of various extracolonic complications, but the subsequent surveillance endoscopy revealed no abnormalities. Histopathological examination of the resected specimen revealed adenocarcinoma invading the submucosa in 2 of them, and in 1, HGD was diagnosed.
Table 1.
Cases of definite dysplasia or cancer after ileo-rectal anastomosis.
| Case | Age at onset | Age at IRA | IRA duration | Grade of dysplasia at endoscopy | Postoperative diagnosis | Survival |
|---|---|---|---|---|---|---|
| 1 | 29 | 33 | 9 | HGD | sm | Alive |
| 2 | 57 | 58 | 19 | LGD | sm | Alive |
| 3 | 22 | 24 | 23 | LGD | m(HGD) | Alive |
| 4 | 56 | 58 | 20 | LGD | — | Alive |
HGD: high-grade dysplasia: IRA, ileo-rectal anastomosis: LGD: low-grade dysplasia;M: mucosa; sm: submucosa.
Figure 2.
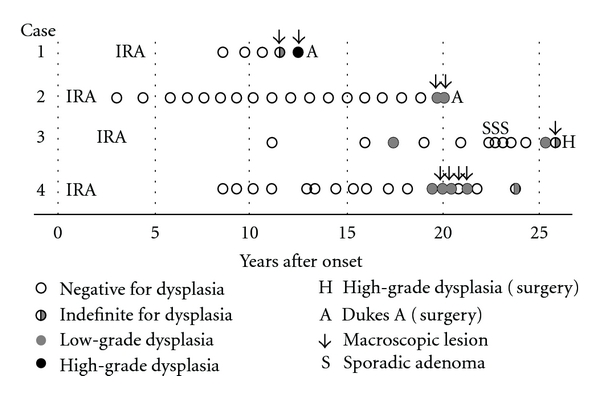
Results of surveillance colonoscopy in patients with definite dysplasia after ileo-rectal anastomosis.
One patient, who had received hand-sewn IPAA, had an ulcerative lesion in the staple line of the pouch, and was diagnosed as LGD. However, the subsequent surveillance revealed no abnormalities. No other patients receiving IPAA had definite dysplasia or cancer detected during the postoperative surveillance.
One patient, who had received IPAA with mucosectomy due to colitic cancer, was diagnosed as HGD during the pouch surveillance conducted 2 years after the operation. The ileal pouch was surgically resected, and the permanent ileostomy was left. The histopathology revealed transmurally invasive signet-ring cells, which was compatible with recurrence of the colitic cancer. No other dysplastic or neoplastic lesions were found during the pouch surveillance.
4. Discussion
It is well recognized that patients receiving subtotal colectomy remain at a risk of developing carcinoma in the remnant rectum; most of the carcinomas of the remnant rectum are diagnosed in an advanced stage. The development of rectal cancer is reported to be associated with the duration of ulcerative colitis and with poor surveillance, and most patients who developed rectal cancer presented with an advanced tumour stage (III and IV) [19]. In our series, by the performance of a meticulous surveillance colonoscopy, definite dysplasia and cancer were found in four (14%) out of 29 patients who had received IRA. Analysis of the resected specimens revelead carcinoma with submucosal invasion in two of them, and HGD in one. Therefore, surveillance colonoscopy was considered effective for the detection of dysplasia or cancer at an earlier stage.
Stapled IPAA is a safer method, with lower incidence of complications than hand-sewn IPAA, but the rectal remnant of few centimeters will theoretically retain the risk of malignant transformation [15]. In a study conducted by the British group, involving 135 patients who had received IPAA with double-stapling technique (DST), and were followed by surveillance colonoscopy for a median period of 56 months [20], no cases of dysplasia or carcinoma were found; thus, it was concluded that cuff surveillance in the first decade after IPAA with DST is not necessary. On the other hand, a study from the Cleveland Clinic diagnosed 2 LGD and 4 HGD among the 178 patients who had received stapled IPAA [21]. They concluded that patients with dysplasia of the colon or the upper third of the rectum can be efficiently managed with stapled IPAA, provided that a postoperative surveillance program is adequately indicated. In our series, no cases of dysplasia of the remnant rectum were found among the patients who had received stapled IPAA. Therefore, taking together our results and those previously reported, we can speculate that the risk of carcinoma development in the remnant rectum is relatively low. On the other hand, although not common, carcinoma or dysplastic lesion may occur in those patients who had received stapled IPAA, since remnant rectum is left similar to those who receive IRA. Although the risk of carcinoma of the remnant rectum is relatively low, we believe that surveillance colonoscopy should be performed in those patients who had received stapled IPAA. The early detection of carcinoma or dysplastic lesion by the surveillance program will allow the indication of anal sphincter saving procedures, such as the pouch advancement method.
Mucosectomy is a technique to remove all the rectal mucosa with malignant potential. In our series, no cases of dysplasia of the rectal remnant were found among those patients who had received hand-sewn IPAA. However, the histological analysis of the resected specimens of patients who had received pouch excision following mucosectomy revealed the presence of remaining isolated rectal mucosa [10, 11]. Moreover, several cases of “rectal” carcinoma after IPAA with mucosectomy have been reported [12–14]. Therefore, mucosectomy is not enough to completely remove the rectal mucosa, in order to eliminate the risk of cancer.
Recently, the risk of carcinoma of the ileal pouch is a major concern among colorectal surgeons. In our series, one patient who had received stapled IPAA was diagnosed as LGD of the staple line ulcer of the pouch, but the subsequent surveillance endoscopic followup of this case revealed no remaining dysplastic lesions. Gullberg et al. found 5 cases of dysplasia in the ileal pouch by the surveillance endoscopy, and all these cases had persistent severely atrophic mucosa [13]. Several reports have shown the detection of dysplasia or cancer in the ileal pouch or in the rectal remnant after restorative proctocolectomy [21, 22]. However, several authors consider that the risk of carcinoma development in the ileal pouch is not high. Hulten et al. conducted a 30-year followup study of the Kock pouch, and concluded that it was very unlikely for invasive carcinoma to develop in the ileal pouch [23]. Thompson-Fawcett et al. examined a retrospective cohort consisting of 1221 patients with ileal pouches, and found only one patient with LGD, who had never had pouchitis [24]. Herline et al. found only one LGD out of 222 biopsies from the ileal pouch [25]. Although the risk of carcinoma development in the ileal pouch is controversial, it is of note that most of the patients with carcinoma of the ileal pouch were diagnosed at an advanced stage. We consider that the appropriate surveillance endoscopy should be indicated for those patients receiving IPAA, until definitive conclusions can be drawn.
In summary, postoperative surveillance endoscopy for UC is useful to detect cancer at an early stage, which will allow the inidication of curative restorative proctocolectomy. Patients receiving IPAA are those who mostly should receive surveillance endoscopy. Although the total risk of cancer development in patients who had undergone IPAA seems to be relatively low, surveillance should be indicated until further investigations deny its effectiveness.
References
- 1.Hata K, Watanabe T, Kazama S, et al. Earlier surveillance colonoscopy programme improves survival in patients with ulcerative colitis associated colorectal cancer: results of a 23-year surveillance programme in the Japanese population. British Journal of Cancer. 2003;89(7):1232–1236. doi: 10.1038/sj.bjc.6601247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ekbom A, Helmick C, Zack M, Adami HO. Ulcerative colitis and colorectal cancer. A population-based study. The New England Journal of Medicine. 1990;323(18):1228–1233. doi: 10.1056/NEJM199011013231802. [DOI] [PubMed] [Google Scholar]
- 3.Eaden JA, Abrams KR, Mayberry JF. The risk of colorectal cancer in ulcerative colitis: a meta-analysis. Gut. 2001;48(4):526–535. doi: 10.1136/gut.48.4.526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Winawer SJ, St John DJ, Bond JH, et al. Prevention of colorectal cancer: guidelines based on new data. WHO Collaborating Center for the Prevention of Colorectal Cancer. Bulletin of the World Health Organization. 1995;73(1):7–10. [PMC free article] [PubMed] [Google Scholar]
- 5.Winawer S, Fletcher R, Rex D, et al. Colorectal cancer screening and surveillance: clinical guidelines and rationale-update based on new evidence. Gastroenterology. 2003;124(2):544–560. doi: 10.1053/gast.2003.50044. [DOI] [PubMed] [Google Scholar]
- 6.Baker WN, Glass RE, Ritchie JK, Aylett SO. Cancer of the rectum following colectomy and ileorectal anastomosis for ulcerative colitis. British Journal of Surgery. 1978;65(12):862–868. doi: 10.1002/bjs.1800651211. [DOI] [PubMed] [Google Scholar]
- 7.Johnson WR, Hughes ES, McDermott FT, et al. The outcome of patients with ulcerative colitis managed by subtotal colectomy. Surgery Gynecology and Obstetrics. 1986;162(5):421–425. [PubMed] [Google Scholar]
- 8.Parks AG, Nicholls RJ, Belliveau P. Proctocolectomy with ileal reservoir and anal anastomosis. British Journal of Surgery. 1980;67(8):533–538. doi: 10.1002/bjs.1800670802. [DOI] [PubMed] [Google Scholar]
- 9.Utsunomiya J, Iwama T, Imajo M, et al. Total colectomy, mucosal protectomy, and ileoanal anastomosis. Diseases of the Colon and Rectum. 1980;23(7):459–466. doi: 10.1007/BF02987076. [DOI] [PubMed] [Google Scholar]
- 10.O’Connell PR, Pemberton JH, Weiland LH, et al. Does rectal mucosa regenerate after ileoanal anastomosis? Diseases of the Colon and Rectum. 1987;30(1):1–5. doi: 10.1007/BF02556908. [DOI] [PubMed] [Google Scholar]
- 11.Heppell J, Weiland LH, Perrault J. Fate of the rectal mucosa after rectal mucosectomy and ileoanal anastomosis. Diseases of the Colon and Rectum. 1983;26(12):768–771. doi: 10.1007/BF02554744. [DOI] [PubMed] [Google Scholar]
- 12.Laureti S, Ugolini F, D’Errico A, Rago S, Poggioli G. Adenocarcinoma below ileoanal anastomosis for ulcerative colitis: report of a case and review of the literature. Diseases of the Colon and Rectum. 2002;45(3):418–421. doi: 10.1007/s10350-004-6194-0. [DOI] [PubMed] [Google Scholar]
- 13.Gullberg K, Stahlberg D, Liljeqvist L, et al. Neoplastic transformation of the pelvic pouch mucosa in patients with ulcerative colitis. Gastroenterology. 1997;112(5):1487–1492. doi: 10.1016/s0016-5085(97)70029-5. [DOI] [PubMed] [Google Scholar]
- 14.Stern H, Walfisch S, Mullen B, McLeod R, Cohen Z. Cancer in an ileoanal reservoir: a new late complication? Gut. 1990;31(4):473–475. doi: 10.1136/gut.31.4.473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Sequens R. Cancer in the anal canal (transitional zone) after restorative proctocolectomy with stapled ileal pouch-anal anastomosis. International Journal of Colorectal Disease. 1997;12(4):254–255. doi: 10.1007/s003840050100. [DOI] [PubMed] [Google Scholar]
- 16.Vieth M, Grunewald M, Niemeyer C, Stolte M. Adenocarcinoma in an ileal pouch after prior proctocolectomy for carcinoma in a patient with ulcerative pancolitis. Virchows Archiv. 1998;433(3):281–284. doi: 10.1007/s004280050248. [DOI] [PubMed] [Google Scholar]
- 17.Heuschen UA, Heuschen G, Autschbach F, Allemeyer EH, Herfarth C. Adenocarcinoma in the ileal pouch: late risk of cancer after restorative proctocolectomy. International Journal of Colorectal Disease. 2001;16(2):126–130. doi: 10.1007/s003840000276. [DOI] [PubMed] [Google Scholar]
- 18.Riddell RH, Goldman H, Ransohoff DF, et al. Dysplasia in inflammatory bowel disease: standardized classification with provisional clinical applications. Human Pathology. 1983;14(11):931–968. doi: 10.1016/s0046-8177(83)80175-0. [DOI] [PubMed] [Google Scholar]
- 19.da Luz Moreira A, Kiran RP, Lavery I. Clinical outcomes of ileorectal anastomosis for ulcerative colitis. British Journal of Surgery. 2010;97(1):65–69. doi: 10.1002/bjs.6809. [DOI] [PubMed] [Google Scholar]
- 20.Coull DB, Lee FD, Henderson AP, Anderson JH, McKee RF, Finlay IG. Risk of dysplasia in the columnar cuff after stapled restorative proctocolectomy. British Journal of Surgery. 2003;90(1):72–75. doi: 10.1002/bjs.4007. [DOI] [PubMed] [Google Scholar]
- 21.Remzi FH, Fazio VW, Delaney CP, et al. Dysplasia of the anal transitional zone after ileal pouch-anal anastomosis: results of prospective evaluation after a minimum of ten years. Diseases of the Colon and Rectum. 2003;46(1):6–13. doi: 10.1007/s10350-004-6488-2. [DOI] [PubMed] [Google Scholar]
- 22.Iwama T, Kamikawa J, Higuchi T, et al. Development of invasive adenocarcinoma in a long-standing diverted ileal J-pouch for ulcerative colitis: report of a case. Diseases of the Colon and Rectum. 2000;43(1):101–104. doi: 10.1007/BF02237251. [DOI] [PubMed] [Google Scholar]
- 23.Hulten L, Willen R, Nilsson O, Safarani N, Haboubi N. Mucosal assessment for dysplasia and cancer in the ileal pouch mucosa in patients operated on for ulcerative colitis—A 30-year follow-up study. Diseases of the Colon and Rectum. 2002;45(4):448–452. doi: 10.1007/s10350-004-6218-9. [DOI] [PubMed] [Google Scholar]
- 24.Thompson-Fawcett MW, Marcus V, Redston M, Cohen Z, McLeod RS. Risk of dysplasia in long-term ileal pouches and pouches with chronic pouchitis. Gastroenterology. 2001;121(2):275–281. doi: 10.1053/gast.2001.26442. [DOI] [PubMed] [Google Scholar]
- 25.Herline AJ, Meisinger LL, Rusin LC, et al. Is routine pouch surveillance for dysplasia indicated for ileoanal pouches? Diseases of the Colon and Rectum. 2003;46(2):156–159. doi: 10.1007/s10350-004-6517-1. [DOI] [PubMed] [Google Scholar]